
Abstract
Endometriosis is a condition which affects many reproductive age women. During pregnancy, an ovarian endometrioma may undergo decidualization, which may take on the sonographic appearance suggestive of malignancy. In this instance, a surgical approach for treatment may be deemed necessary. Three cases are presented with different outcomes, worthy of viewing the contrasting management. In case 1, a patient was diagnosed with a left ovarian cyst at her routine 20-week gestation sonogram. This sonographic examination was suggestive of an ovarian malignancy. The patient underwent laparoscopy with left salpingo-oophorectomy at 23 weeks gestational age, without complications. The pathologic diagnosis of the removed mass was a decidualized endometrioma. In case 2, a female patient presented with bilateral ovarian decidualized endometriomas that were demonstrated sonographically and had the appearance of malignancy. This patient was treated conservatively with serial follow-up sonograms during her pregnancy. At the 2-month post-partum follow-up sonogram demonstrated persistent bilateral endometriomas, without decidualization. However, in case 3, possible decidualization of an endometrioma was seen, and a follow-up sonogram revealed the presence of ovarian carcinoma. There is previously published support for watchful waiting when similar sonographic findings, in pregnancy, are seen.
Keywords
Endometriosis is a common gynecologic disorder affecting about 10% of women of reproductive age, and ovarian endometriomas specifically account for 4% to 5% of ovarian cysts, diagnosed in early pregnancy. 1 The decidualization process is hormonally dependent and normally occurs to prepare the endometrium for the implantation of the early product of conception. It advances in pregnancy, causing changes to occur in ectopic endometrial tissue (outside of the uterus), which would include endometriotic implants (e.g., those found in the ovary, forming endometriomas). Decidualization of an endometrioma (DE) may have sonographic features which are similar to that of ovarian malignancy, 2 which often prompts a surgical extirpative approach. Encountering this entity with sonography may become increasingly frequent, since many pregnant women are having routine obstetrical sonograms, in the first trimester. An endometrioma is often well-characterized, and it is sometimes altered during pregnancy as a result of this decidualization process. DE can resemble a malignant ovarian tumor on a sonogram, which can cause anxiety to a woman (and her doctor) and lead to unnecessary and potentially harmful surgical interventions. This case series is presented to contrast a previous encounter with this condition from 5 years ago, with current instances, and offer a possibly improved modern approach to DE.
Case Reports
Case 1, a 33-year-old G2P0010, was diagnosed with a 2.6 cm × 1.8 cm × 1.7 cm left ovarian cyst at her routine 20-week gestation US. She had no history of ovarian endometrioma on previous sonograms, during earlier gestation. The cyst was unilocular with grounded-glass echogenicity and vascularized papillary projections suggestive of ovarian malignancy. Gynecologic oncology consultation was obtained, and patient underwent laparoscopic left salpingo-oophorectomy at 23 weeks gestational age without complications. The pathology diagnosis of the removed mass was a DE.
Case 2, a 30-year-old G2P0010 female patient, presented for initial sonogram at 11 weeks and 4 days for a nuchal translucency screen. Bilateral ovarian endometriomas were demonstrated with this initial sonogram and revealed homogeneous low-level echoes, without papillary projections or internal blood flow. Bilateral ovarian DEs were suspected during a repeat sonogram at 28 weeks 3 days gestation. This was due to the presence of rounded vascularized papillary projections with smooth contours, within an ovarian cyst and the ground-glass low-level echogenicity of the cyst fluid. The patient was treated conservatively with serial follow-up sonograms during her pregnancy, as no malignancy was suggested. The patient had a normal spontaneous vaginal delivery at 36 weeks 6 days of gestation on August 30, 2020. Follow-up sonograms at 2 months post-partum demonstrated persistent bilateral endometriomas without decidualization and with partial obliteration of the posterior cul-de-sac.
Case 3, a 30-year-old G1 P0010 female, with a spontaneous abortion 1 month previously, presented for evaluation of bleeding. A transvaginal sonogram (TVS) was performed, revealing a retained product of conception (RPOC), a left ovarian endometrioma, and a right possibly DE. Ovarian malignancy could not be ruled out, and a follow-up TVS was planned. Evacuation of the RPOC was performed, and a planned repeat TVS was done 14 weeks later, revealing 40% growth of the ovarian cyst, with an increase in size and color flow in a papillary projection, suggestive of malignancy. A surgical procedure (right salpingo-oophorectomy) was subsequently performed, revealing an endometrioid adenocarcinoma of the ovary.
Figure 1 displays the antepartum sonogram in case 1, which prompted the surgical removal of the endometrioma, due to its appearance suggestive of malignancy. Figure 2 displays the antepartum sonogram of the identified DE in case 2, which was closely followed for the duration of that pregnancy. Figure 3 reveals the sonogram of that same endometrioma in case 2, 9 weeks after delivery, showing the resolution of the decidualization. Figure 4 displays another sonographic example of that DE over 5 months post-partum. Figure 5 displays the first TVS in case 3, and Figure 6 displays the second TVS performed in case 3, revealing the sonographic image of the ovarian carcinoma.
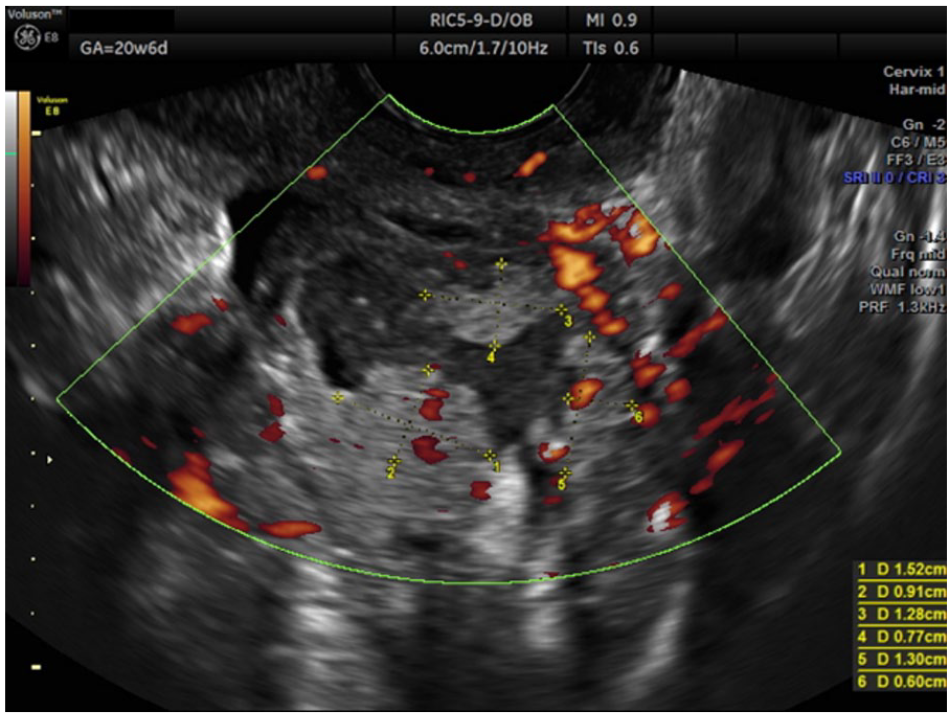
Power Doppler sonography of the right ovary demonstrating unilocular-solid cyst with ground-glass echogenicity and several vascularized papillary projections, suggestive of ovarian malignancy (case 1).
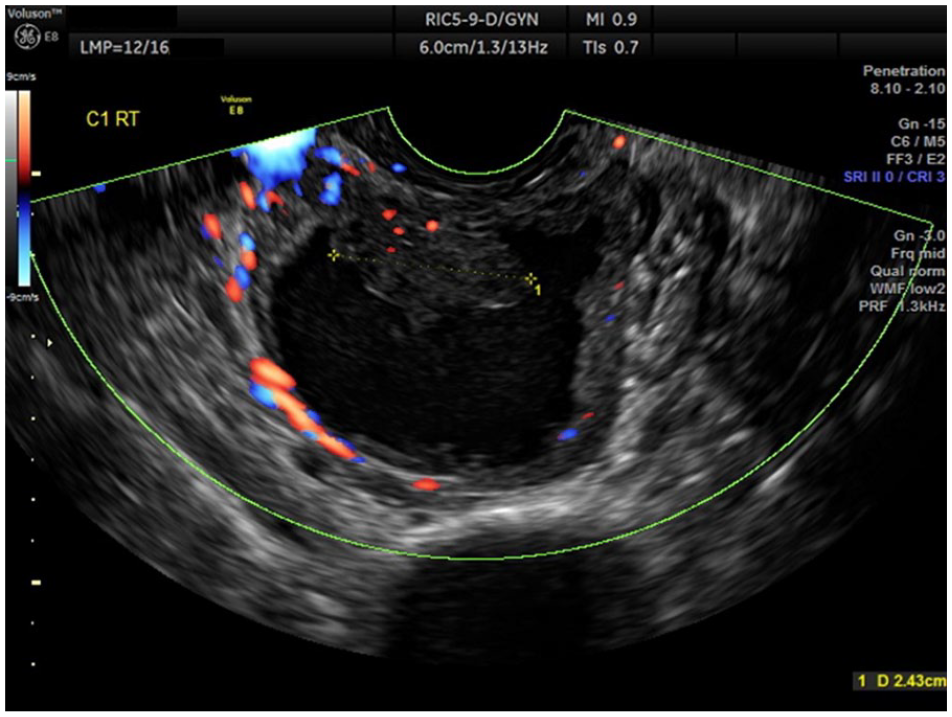
Transvaginal sonography with high-definition color-flow Doppler at 30 weeks 2 days gestational age, demonstrating right ovarian decidualized endometrioma with a 2.43-cm vascularized papillary projection (case 2).

Gray-scale transvaginal sonography at 9 weeks post-partum, demonstrating a right ovarian endometrioma without decidualization (case 2).
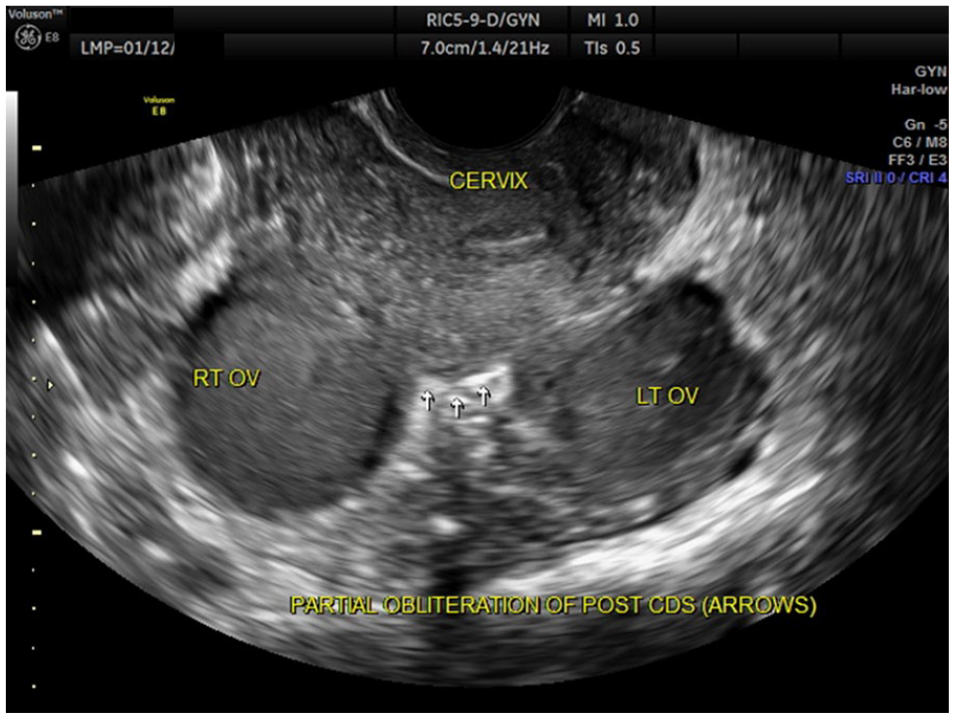
Gray-scale transvaginal sonography at 5.5 months post-partum demonstrating bilateral ovarian endometriomas with partial obliteration of the posterior cul-de-sac (case 2).
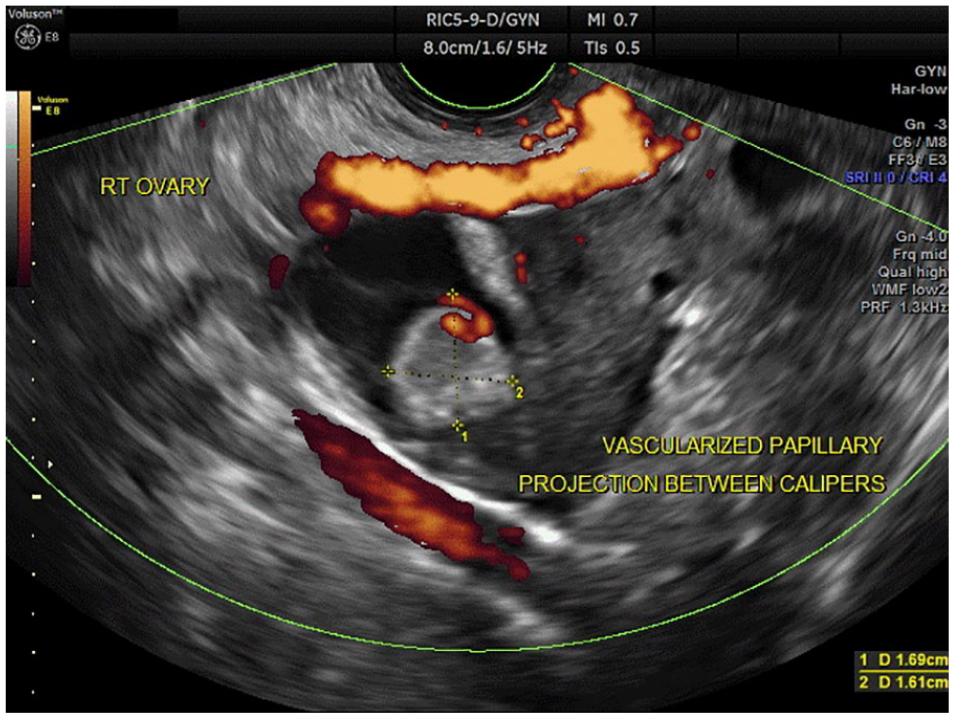
Initial transvaginal sonography with power Doppler angiography demonstrating a unilocular right ovarian cyst with a 1.69 cm × 1.61 cm vascular papillary projection, suspicious for decidualized endometrioma.
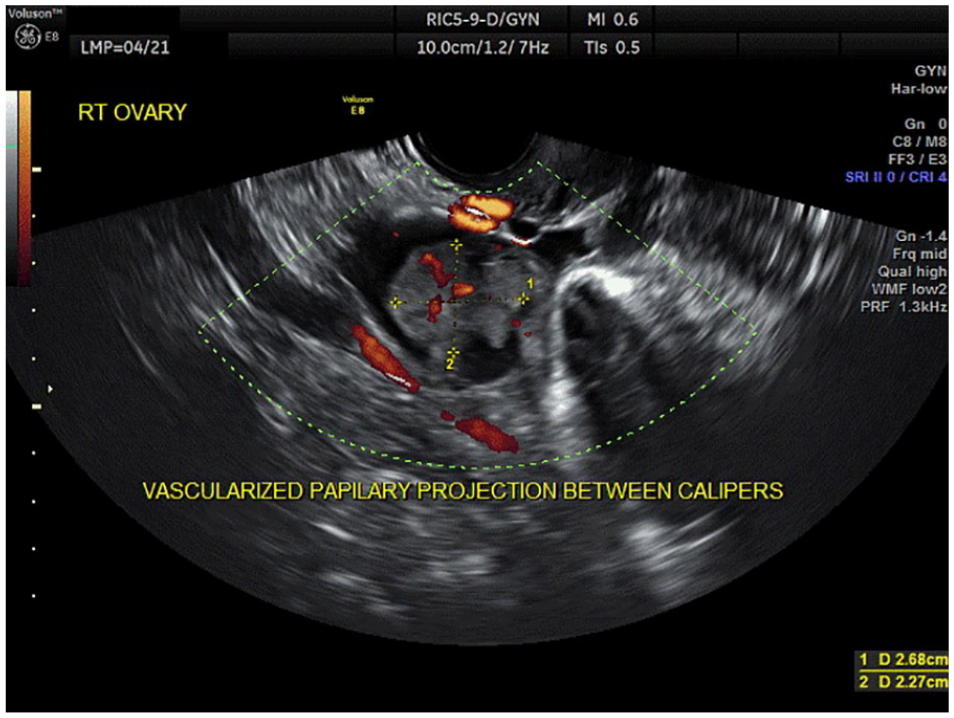
Repeated transvaginal sonography with power Doppler angiography, 14 weeks after initial ultrasound, demonstrating a right ovarian cyst with a 2.68 cm × 2.27 cm vascularized papillary projection between calipers. Suspected right ovarian malignancy was later confirmed.
Discussion
The potential for decidualization of ovarian endometriomas has long been recognized to occur at times, which has been previously reported. 3 The concern for the resemblance of the sonographic features of this decidualization, with its suggestion of malignancy, may warrant attention and is of particular concern. A series of 18 such DE cases, which were surgically removed during pregnancy, has been reported. 4 Another series of 17 cases also having surgery for DEs resembling a malignancy was reported, all of which had a benign result. 5 In contrast, a series of 24 cases which were expectantly managed during pregnancy for the sonographically described DEs appearing to be possibly malignant revealed the resolution of this decidualization at the conclusion of each pregnancy, serving to be reassuring for this expectant type of management. 6 Further commentary of the benefit of expectant management of pregnancy-related DEs was recently reinforced. 7
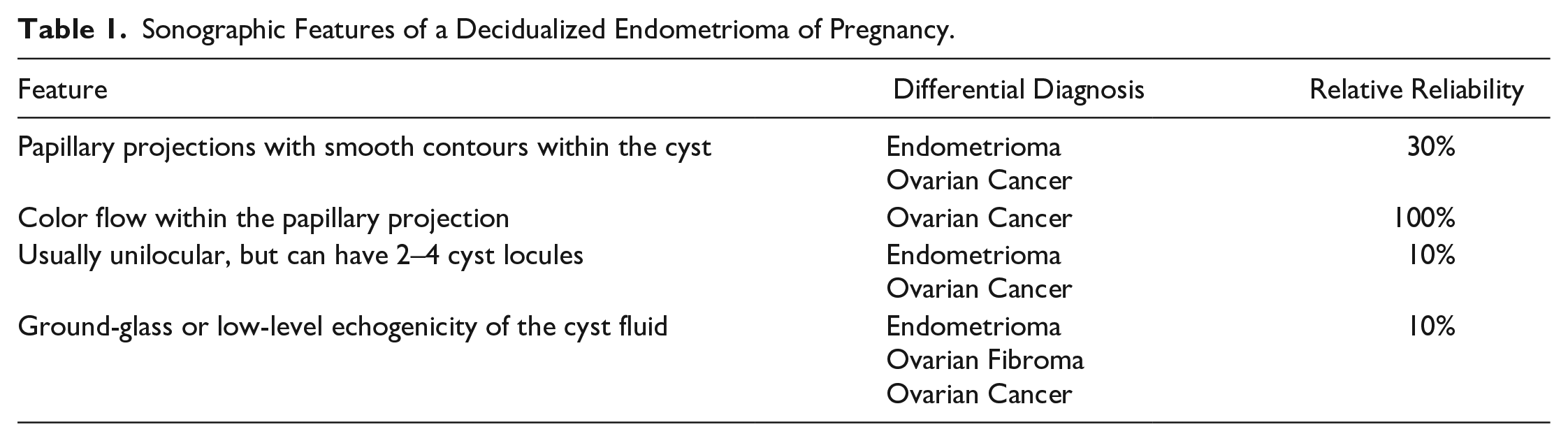
Although prior case series of DEs in pregnancy have failed to identify a single case of malignancy, despite the appearance suggestive of that possibility, the finite possibility of malignancy will always need to be considered in such cases. In fact, in case 3, though an appearance of DE in a recently pregnant woman was seen, follow-up sonograms revealed persistent sonographic evidence of a possible malignant progression, which was ultimately confirmed as ovarian cancer. However, cautiously and carefully following such cases of DE, in pregnancy, seems to be a reasonable option. The contrasting management of these cases described in this report may need to be considered in this context. In case 2, resolution of the appearance of malignancy occurred by the end of the pregnancy without its removal, which could have occurred in case 1, had there not been the removal of the endometrioma. In the first case, surgery was performed, and in the second case, no surgery was performed, yet the results were essentially the same for both of those cases. Specific guidelines from the review of the cases in this series and identification of the lessons learned from the management of these cases, along with a review of the literature, can be seen in Table 1.
Sonographic Features of a Decidualized Endometrioma of Pregnancy.
Conclusion
When DE is sonographically identified during pregnancy in a patient who is otherwise asymptomatic, the patient should be closely monitored with sonography every 4 weeks, during that pregnancy. After delivery of the patient, a repeat sonogram should be performed, and if resolution of the DE is identified, the patient can be reassured. Observation of DE in pregnant patients will likely continue, and patients should receive appropriate counseling for this in the future, mentioning all possible outcomes. Demonstrations such as what is presented here have been reported in the literature previously, and there appears to be support for watchful waiting when similar sonographic findings in pregnancy are seen of the DE.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.