
Abstract
Retinoblastoma is a cancer that affects the eye, and if untreated, it can spread to other parts of the body. Retinoblastoma is the most common pediatric eye cancer and accounts for 3% of all childhood cancers. It can be hereditary or sporadic (nonhereditary). This case study presents a unilateral retinoblastoma of the right eye in a pediatric patient. A diagnosis of retinoblastoma was made by correlating sonography, magnetic resonance imaging, and ophthalmology. Treatment for retinoblastoma depends on the severity of the cancer but can include radiation, chemotherapy, focal laser therapy, and/or surgery. This particular case of retinoblastoma was treated with chemotherapy.
Keywords
Retinoblastoma is a rare pediatric cancer, accounting for 3% of pediatric cancers diagnosed each year, with approximately 300 new cases diagnosed annually.1,2 Retinoblastoma is the most common pediatric eye tumor, and it primarily affects children <2 years old, with adults rarely affected. 2 When it occurs unilaterally, which makes up 75% of the cases diagnosed annually, it is typically nonhereditary, while bilateral retinoblastoma is predominantly passed down in families in an autosomal-dominant fashion and accounts for 25% of cases diagnosed annually. 1 Retinoblastoma develops on the retina, which lines the posterior portion of the eyeball. A common early indication of retinoblastoma is leukocoria, or “white reflex,” as observed in pictures. Specifically, leukocoria is the presence of a white flash in the pupil instead of the normal red flash frequently seen in photographs. 2
Early diagnosis and treatment of retinoblastoma is important because with early intervention, the prognosis is generally good. In contrast, with later diagnosis of retinoblastoma, the treatment must be much more aggressive, and the prognosis is worse. However, the prognosis and mortality rates vary greatly by region. Developed countries, such as the United States and Europe, have a low mortality rate of only 3% to 5%, whereas less developed countries, such as parts of Africa, have a more devastating mortality rate of up to 70%. 3 Typically, patients with retinoblastoma will lose sight in the affected eye, especially if the retina detaches from the back of the eye as a result of tumor invasion. When retinoblastoma is diagnosed before retinal detachment occurs, vision may be preserved in the affected eye.
In the case presented, sonography and magnetic resonance imaging (MRI) were used to confirm a suspected diagnosis of retinoblastoma by evaluating a mass in the right posterior eye. The use of sonography was beneficial because it was noninvasive and provided diagnostic information to confirm retinoblastoma.
Case Report
An 11-month-old girl presented with a 1-month history of an apparent lazy eye and leukocoria. She had been seen by an ophthalmologist, who detected a mass in the right posterior eye. The patient was then referred to a pediatric oncology hospital for a bilateral orbit sonogram. The sonogram was completed on a GE LOGIQ E9 ultrasound machine (GE Healthcare, Waukesha, Wisconsin) with a linear transducer with a center frequency of 12 MHz.
A bilateral orbit sonogram was done, which showed an echogenic mass (1.44 × 0.83 × 1.63 cm) in the posterior area of the right eye (Figure 1). The retina of the affected eye was observed to be detached from the posterior portion of the eyeball (Figure 2). The left eye appeared normal (Figure 3). Images were obtained comparing the normal anatomy of the left, unaffected eye with the anatomy of the right, affected eye (Figure 4). Based on the sonographic findings, MRI was done. The MRI results correlated with the sonogram findings, confirming the diagnosis of retinoblastoma. An axial MRI image was obtained that showed the right, affected eye with the optic nerve exiting it and the left, normal eye (Figure 5). Axial MRI imaging distinctly demonstrated the mass in the right orbit as compared with the normal, left orbit (Figure 6). Sagittal MRI imaging also confirmed the mass in the right posterior eye (Figure 7). A separate sagittal image showed the unaffected, left eye with normal anatomy visible (Figure 8).
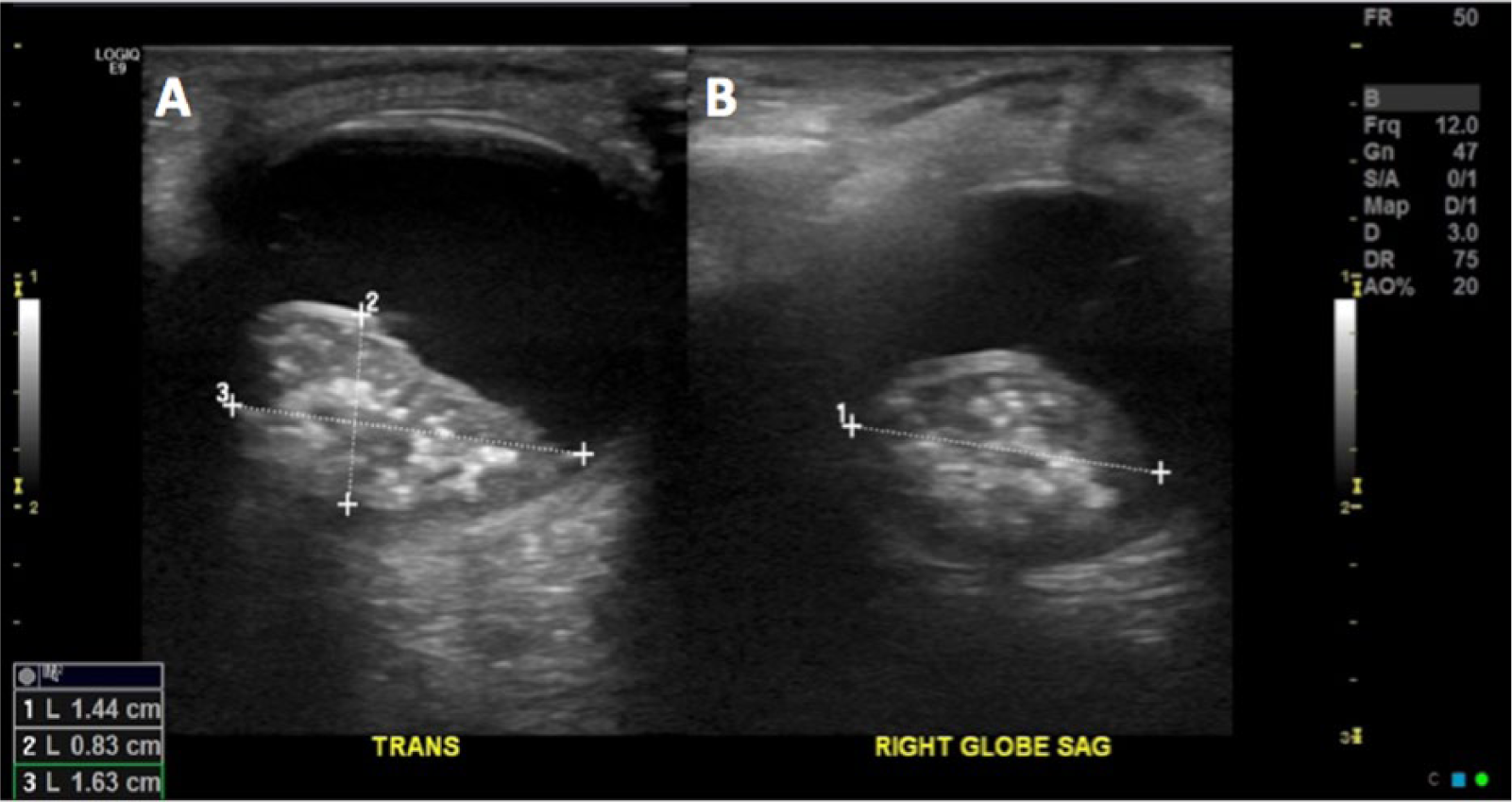
Transverse (A) and sagittal (B) gray-scale sonograms show an echogenic mass (1.44 × 0.83 × 1.63 cm) in the posterior compartment of the right eye.
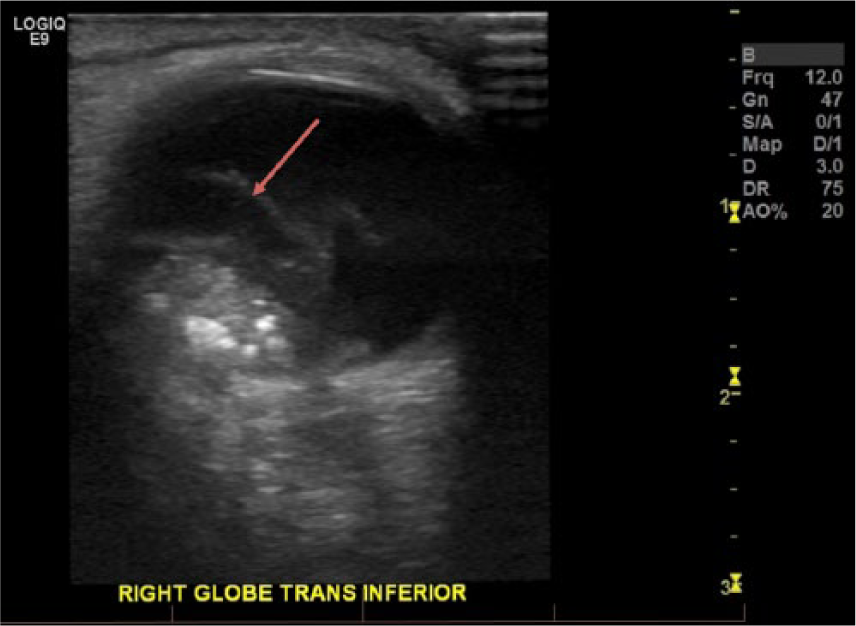
Transverse gray-scale sonogram shows the mass in the inferior portion of the affected, right eye. The detached retina (red arrow) is also visible.
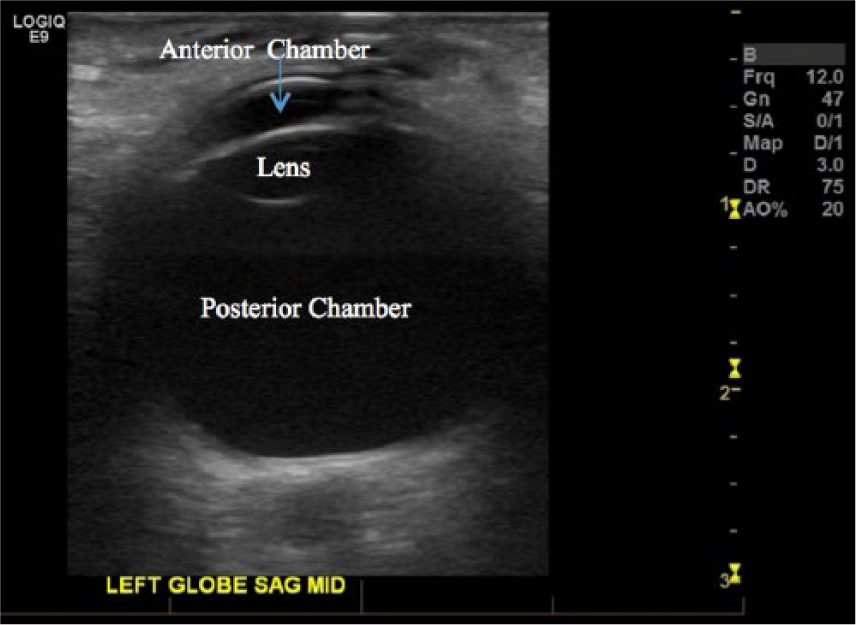
Sagittal gray-scale sonogram illustrates the normal anatomy of the left eye. The anterior chamber (blue arrow) can be visualized at the most anterior aspect of the orbit. The lens can be seen directly behind it, protruding posteriorly into the posterior chamber.
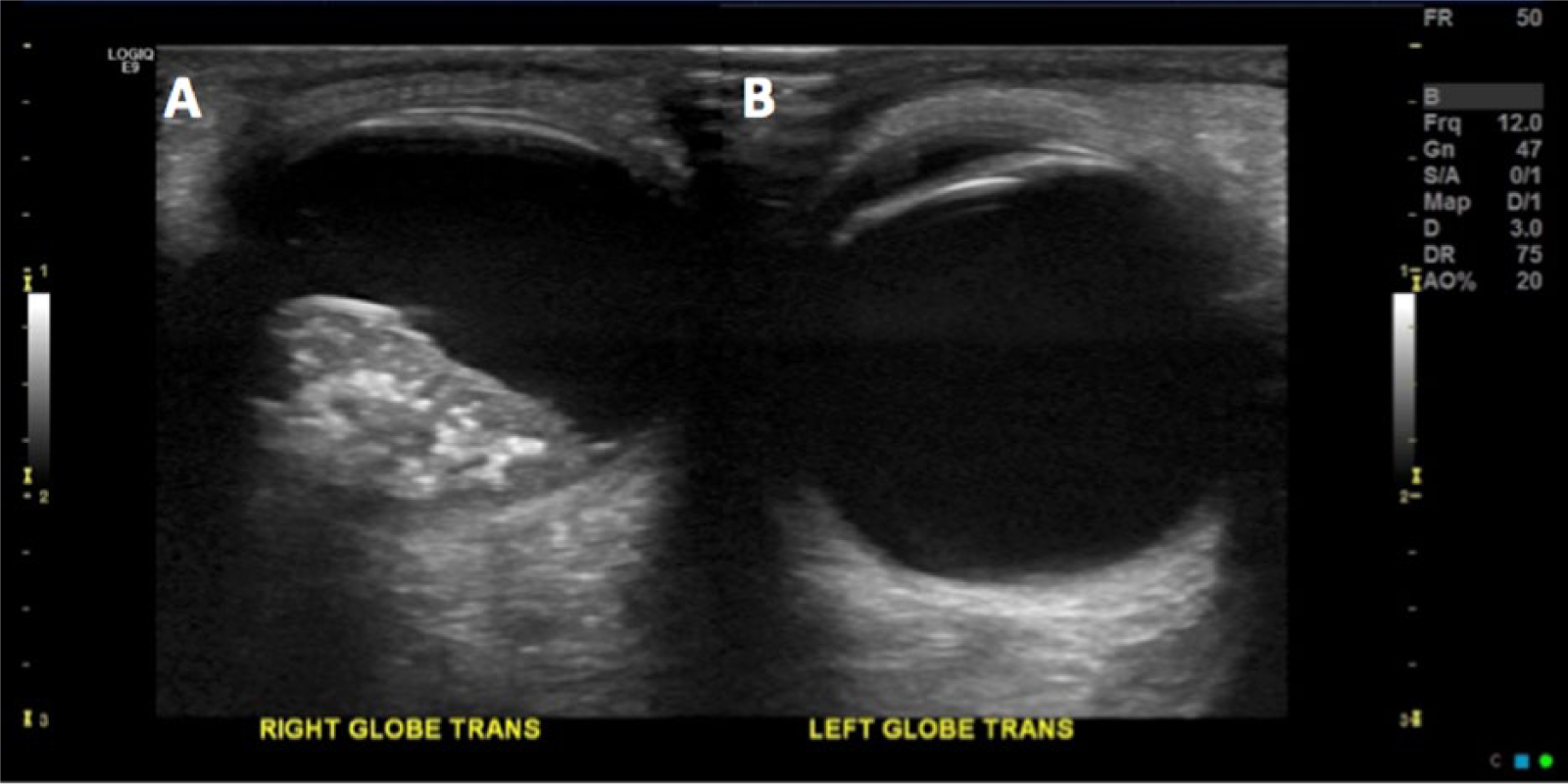
Transverse gray-scale sonographic images compare the affected, right eye (A) with the normal, left eye (B).
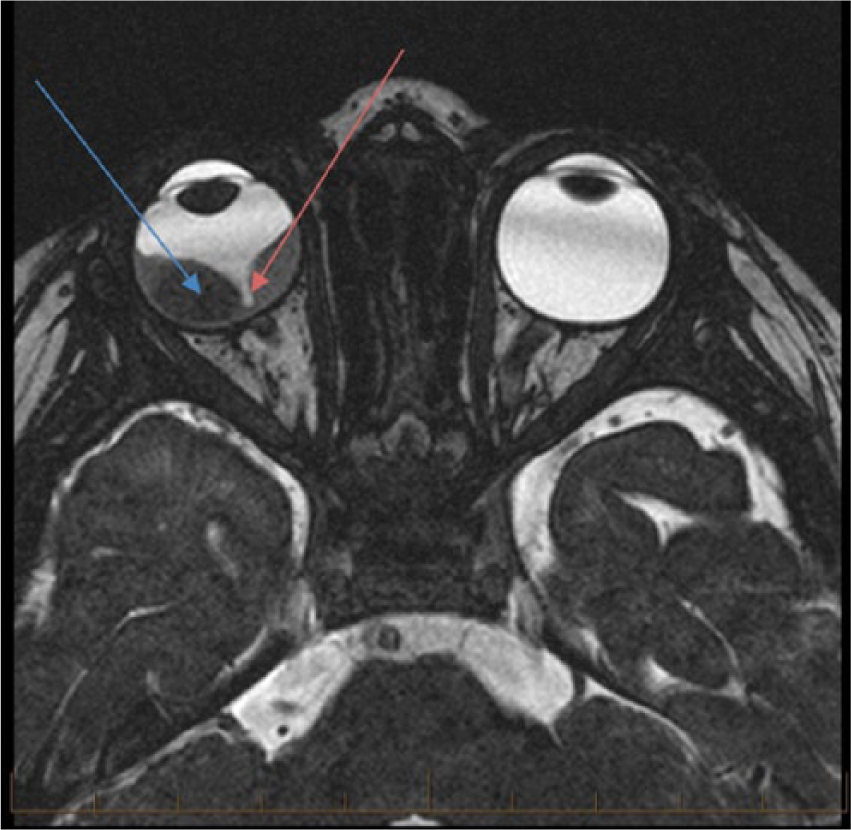
Axial magnetic resonance image shows a mass in the right posterior eye (blue arrow). The optic nerve can be seen exiting the eye (red arrow), with the retina having been displaced by the mass.
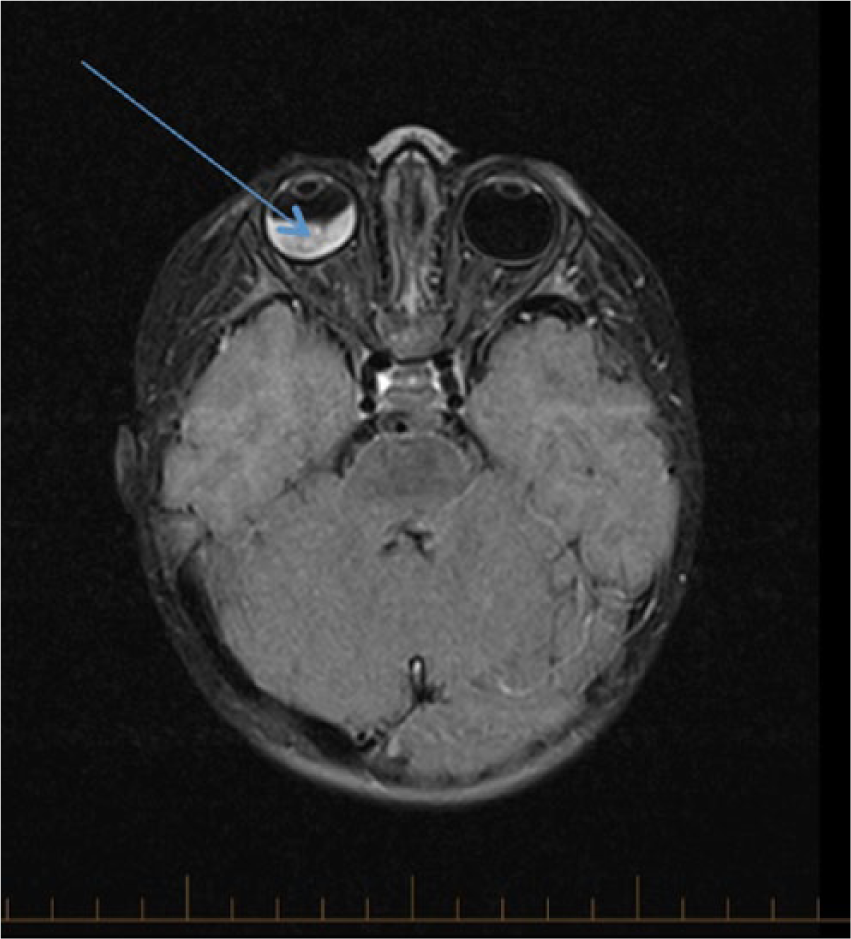
Axial magnetic resonance image presents the mass in the right orbit (blue arrow), as compared with the normal, left orbit.
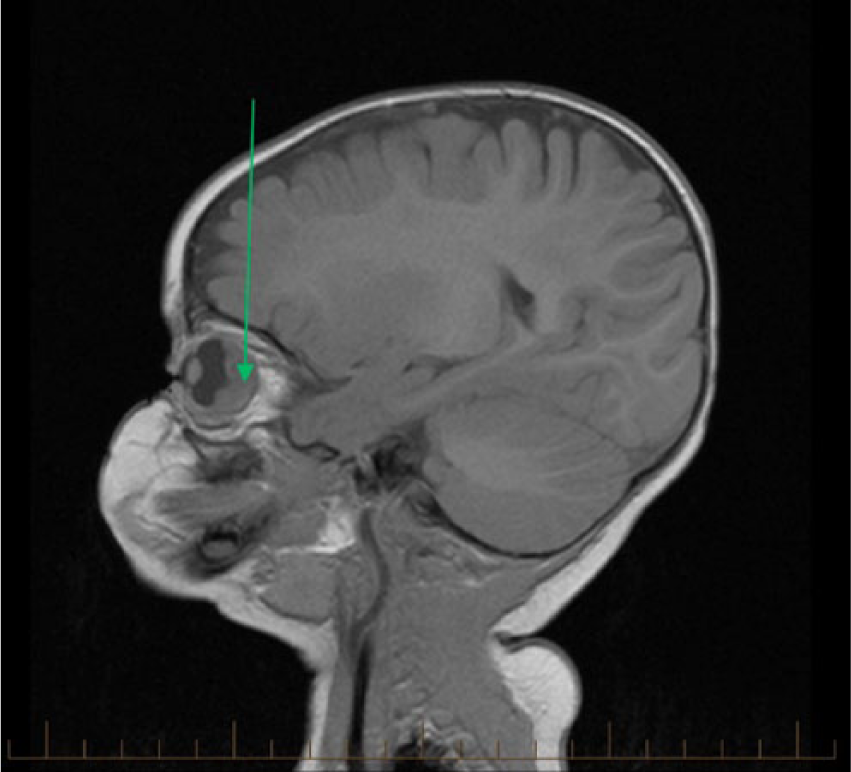
Sagittal magnetic resonance image shows the mass in the posterior portion of the eye (green arrow).
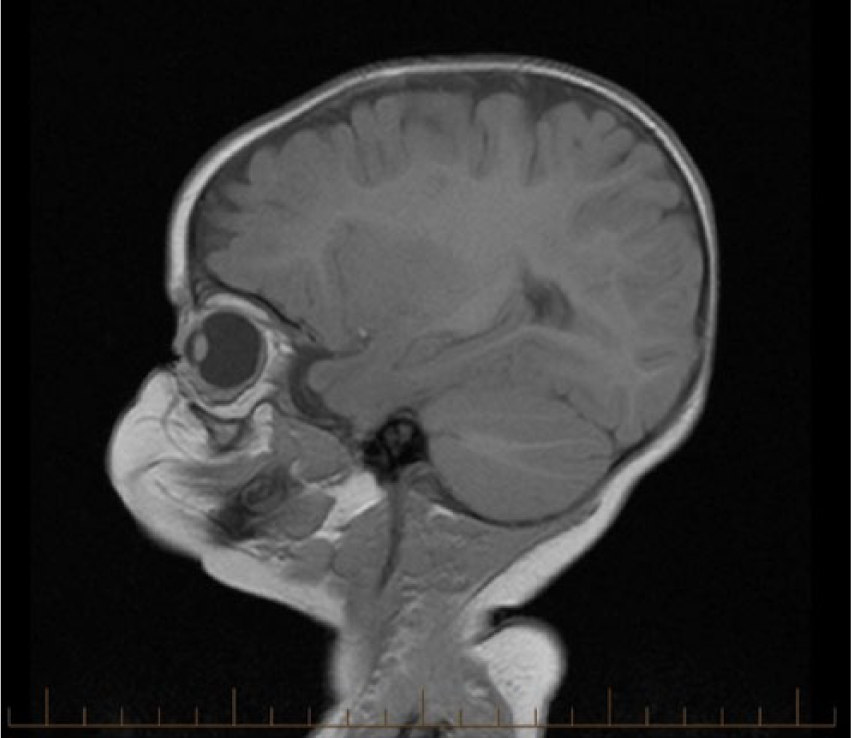
Sagittal magnetic resonance image illustrates the normal, left orbit in contrast.
Discussion
Retinoblastoma can be hereditary or nonhereditary (spontaneous). In most cases of hereditary retinoblastoma, the RB1 gene is responsible and follows an autosomal-dominant pattern. 2 Children who have the RB1 gene are at risk for developing other cancers at different locations during their lifetimes, including a specific brain tumor called pineoblastoma. The development of pineoblastoma in a retinoblastoma patient is known as trilateral retinoblastoma. 1
Children with unilateral, nonhereditary retinoblastoma are not at an increased risk for cancers later in life. Retinoblastoma is typically diagnosed and treated before it spreads outside the eyeball. When it does spread, it can do so to the lymph system, liver, and bone marrow. 1 Retinoblastoma is typically diagnosed through any combination of sonography, MRI, and computed tomography (CT).
Several systems are used to stage retinoblastomas, but one of the newest and most reliable is the international retinoblastoma staging system, based on a scale of 1 to 4. Patients with stage 1 are treated conservatively, with the affected eye enucleated and with all components of the disease removed, with no further treatment needed. Stage 2 patients are typically treated by enucleation, with only small microscopic cellular elements left, which are easily treated. Stage 3 patients have regional extension, and this stage is divided in to “a” and “b.” Stage 3a presents with overt orbital disease, while stage 3b involves preaurical or cervical lymph node extension. Finally, stage 4 is also divided into “a” and “b,” with stage 4a involving hematogenous metastases and further subdivided into two sections based on whether there is a single lesion or multiple lesions. Stage 4b involves central nervous system extension, with three subdivisions under it: stage 4b-1 involves a prechiasmatic mass; stage 4b-2, a central nervous system mass; and stage 4b-3, leptomeningeal disease. 4
Early on in the disease, the mass is typically localized to the affected orbit, but without medical intervention, it can grow significantly and metastasize to other areas of body. 2 Treatment usually involves some combination of radiation, chemotherapy, surgery, and cryotherapy. When diagnosed and treated promptly, retinoblastoma generally has a good prognosis. 1
Sonography can be beneficial in diagnosing suspected cases of retinoblastoma. In retinoblastoma cases that present with calcifications, sonography has an 80% accuracy rate. 5 Sonography provides a detailed view of the eye and can determine which structures are involved. Orbit sonograms show the ocular anatomy with great clarity. Figure 3 demonstrates the normal sonographic appearance of an orbit. The anterior chamber is the first anechoic structure seen in the anterior aspect of the image (blue arrow), while the lens can be visualized just posterior to the anterior chamber. The posterior chamber is the largest anechoic region visualized posterior to the lens. The posterior border appears smooth with no disruption, indicative of a normal, attached retina.
In cases of unilateral retinoblastoma, sonography can be used to compare the affected eye with the unaffected eye, and serial examinations can be compared to evaluate for resolution or progression of the disease. Retinoblastoma appears as an echogenic mass along the posterior portion of the posterior chamber. It is not uncommon for there to be echogenic calcifications scattered throughout. In cases of retinal detachment, there will be a thin echogenic line that floats above the mass, and when tracked, it can usually be traced to an attachment point at an area unaffected by the mass. 5 Occasionally, complete detachment will be seen, where no point of attachment can be located.
When patients present with leukocoria and abnormal eye movement, retinoblastoma is often suspected until proven otherwise; however, several other conditions can present with leukocoria and should thus be considered as differential diagnoses. These include persistent fetal vasculature, Coats disease, and congenital cataracts. 1
Persistent fetal vasculature is a benign condition wherein the vascularity feeding the fetal eye fails to resorb, becomes hypertrophic, and remains patent. 5 The vascularity extends from the lens to the back of the eye. 5 Persistent fetal vasculature can be clearly differentiated from retinoblastoma through sonographic imaging by showing a vascular channel running from the optic nerve to the lens, an intact retina, and a posterior chamber free from mass. MRI can also be used to correlate. 6 MRI findings frequently show microphthalmos in the affected eye, but that does not occur in all cases. 7 The definitive MRI finding is the enhancing triangular tissue, or Cloquet canal, that is demonstrated in the affected eye. 7
Coats disease is a congenital vascular anomaly of the retina. It is the result of a faulty blood-brain barrier that results in leaky retinal vessels that produce exudate. 5 The exudate oozes into the posterior chamber and produces debris. The increased pressure from the additional fluid and the debris that accumulates results in similar symptoms as retinoblastoma. Advanced Coats disease and retinoblastoma appear very similar on sonographic examination. Therefore, sonography is not recommended as the best modality to definitively diagnose Coats disease. 8 On MRI, Coats disease can be diagnosed by showing a posterior chamber free from mass but with the retina detached. There is frequently enhancement around the detached retina, indicating abnormal vasculature. Lipoproteinaceous subretinal exudation appears hyperintense in both T1- and T2-weighted MRI imaging. 1
Sonography can be used to accurately assess for cataracts prenatally as well as postnatally. Cataracts are localized to the lens, which can help to clearly distinguish them from retinoblastoma, as the rest of the eye will appear otherwise normal. The lens can appear uniformly echogenic or have a noticeably thicker rim than that seen in normal orbits. 5
Patients do not have to be sedated or put to sleep to evaluate the orbits, which is another tremendous benefit of using sonography for an orbital examination. Since orbits are superficial, a hockey stick–shaped probe with a frequency ≥10 MHz should be used. 5 The orbits are scanned through the patient’s eyelid (i.e., with the eye closed) via a light touch. As with all sonograms, it is necessary to take ALARA into account (i.e., “as low as reasonably achievable”) and to keep the acoustic output as low as diagnostically possible for the examination, especially since the eyes are sensitive structures and do not attenuate as much as soft tissue. Therefore, care needs to be taken to prevent any possible bioeffects. This case report shows a well-demarcated mass in the right posterior eye that appears to be localized to that area. Based on the correlation of sonographic and MRI findings, the patient’s diagnosis was retinoblastoma, and a proper treatment protocol was initiated. Future treatments could include radiation, focal laser therapy, and surgery.
On MRI T1-weighted imaging, retinoblastoma appears slightly hyperintense to the surrounding vitreous fluid. On T2-weighted imaging, retinoblastoma appears darker when compared with the surrounding vitreous fluid. 7 Since MRI is predominately used to stage retinoblastoma, the accuracy rates vary with the degree of infiltration. When postlaminar optic nerve infiltration is being detected, MRI has an overall accuracy of 93%. 7 With choroidal invasion, the accuracy rate is also 93%. For detection of scleral invasion and peribulbar fat invasion, MRI is reported to have a 100% detection rate. 7
In a similar case reported by Goel et al., 9 a 6-month-old female presented with leukocoria. The patient underwent imaging that included sonography, CT, and MRI. The findings correlated with unilateral retinoblastoma in the left eye. The patient was treated by enucleating the affected eye. Histologic analysis confirmed the mass to be retinoblastoma. The patient recovered well, and she was fitted with a prosthetic eye. This patient had only one affected eye and did not have a family history of retinoblastoma, which is consistent with nonhereditary occurrence of retinoblastoma.
A case of trilateral retinoblastoma that differed considerably from the case discussed here was reported by Presley and Flannigan. 10 This patient was a 30-month-old Haitian boy who had swelling and drainage from the right eye, as well as noticeable changes in visual acuity. The patient underwent a bilateral orbital sonogram, which showed large echogenic masses in both eyes. CT was also performed, which showed a suprasellar tumor in the brain. This, coupled with the bilateral retinoblastoma, led to a diagnosis of trilateral retinoblastoma. At the time of publication, no follow-up was known, but because of the advanced stage of the disease, the prognosis was poor.
The case presented here provides an excellent example of classic unilateral nonhereditary retinoblastoma with common clinical symptoms. This case and the images provided can be used as a comparison source in future cases of suspected retinoblastoma to assist in confirming the diagnosis.
Conclusion
Sonography was used to evaluate and characterize a case of suspected retinoblastoma. Sonographic imaging showed a single unilateral echogenic mass that was consistent with the appearance of retinoblastoma, and the correlation of sonographic and MRI findings confirmed the diagnosis of unilateral retinoblastoma. This case study effectively demonstrates the use of sonography to examine and accurately diagnose abnormalities of the orbits—specifically, retinoblastoma. While the benefits of sonographic evaluation include being noninvasive and not involving radiation exposure, it can also serve as a baseline to which future and serial examinations can be compared in an effort to evaluate the effectiveness of treatment.
Footnotes
Acknowledgements
I thank Patricia Honnoll, RDMS, RVT, for her assistance in obtaining images and information for this case study.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.