
Abstract
This report describes an unanticipated finding in an asymptomatic volunteer scanned in a sonography education program that led to the diagnosis of a rare, benign tumor consistent with a ganglioneuroma. The importance of maintaining a proper protocol for addressing incidental pathological findings for volunteers in the educational setting is emphasized.
Introduction
Recruiting volunteers to be scanned in a medical sonography education program is the cornerstone of ultrasound training as it provides the essential psychomotor skills needed for the student to become a competent, entry-level sonographer. In addition to students practice scanning on each other, recruiting volunteers may improve the students’ overall skills, offering different body habitus, positioning of organs, and the unexpected pathology that will be seen in clinical, real-life scenarios.
The American Institute of Ultrasound in Medicine (AIUM) states that no hazard has been identified that would preclude the prudent and conservative use of diagnostic ultrasound in training and research with the ultrasound exposure kept as low as reasonably achievable (ALARA). 1 It is therefore appropriate that the volunteer be informed of this lack of a bioeffects hazard within the goals of the training. While finding volunteers to be scanned in medical sonography programs in and of itself may be a challenge, the additional policies and procedures for handling volunteers can also be complex but should be in place. In the event of uncovering pathologic findings in a volunteer, a protocol should be in place to manage these findings and should indemnify all parties participating in the laboratory scanning session. For example, a signed release form that includes contact information for a primary care physician who has an established relationship with the volunteer should be in place prior to the student scanning. This essential component provides a process to route any follow-up diagnosis and treatment from the sonographic findings. Additionally, it is suggested that appropriately credentialed laboratory faculty always scan the volunteers before they are released from the laboratory. If incidental findings are noted, the medical director of the sonography program will have the ability to provide written documentation of the abnormal findings. This report discusses an incident where the incidental findings protocol and contingency plan for reporting of pathological findings from a volunteer were both necessary and utilized.
Case Report
As a part of a sonography volunteer program, program applicants are offered (but not obligated to) the opportunity to volunteer as medical models. This volunteering opportunity allows the applicant a chance to talk to the students in the program and receive a firsthand view of the technical and physical skills needed to become a sonographer. In this case, a 23-year-old female volunteered as a medical model while she was applying to the sonography program. The model had no past medical history and was asymptomatic.
On the initial scan, the sonographic findings demonstrated a hypoechoic mass inferior to the left kidney consistent with a retroperitoneal mass (Figure 1A). The student presented the information to the faculty supervisor, who then rescanned the medical model to confirm the abnormality. The medical director was then notified of the finding. Upon review of the images by the medical director, a report noted the sonogram demonstrated a well-circumscribed 5 × 6 cm solid, lobulated mass located inferior to the left kidney (Figure 1B). In addition, minimal anterior displacement of the left kidney was noted (Figure 1C). The borders of the kidney were identified and did not appear to be contiguous with the mass. Color Doppler assessment did not demonstrate any flow into the mass (images not shown). This unofficial report of the incidental findings was sent by the medical director to the medical model’s primary care physician for further evaluation of the mass.
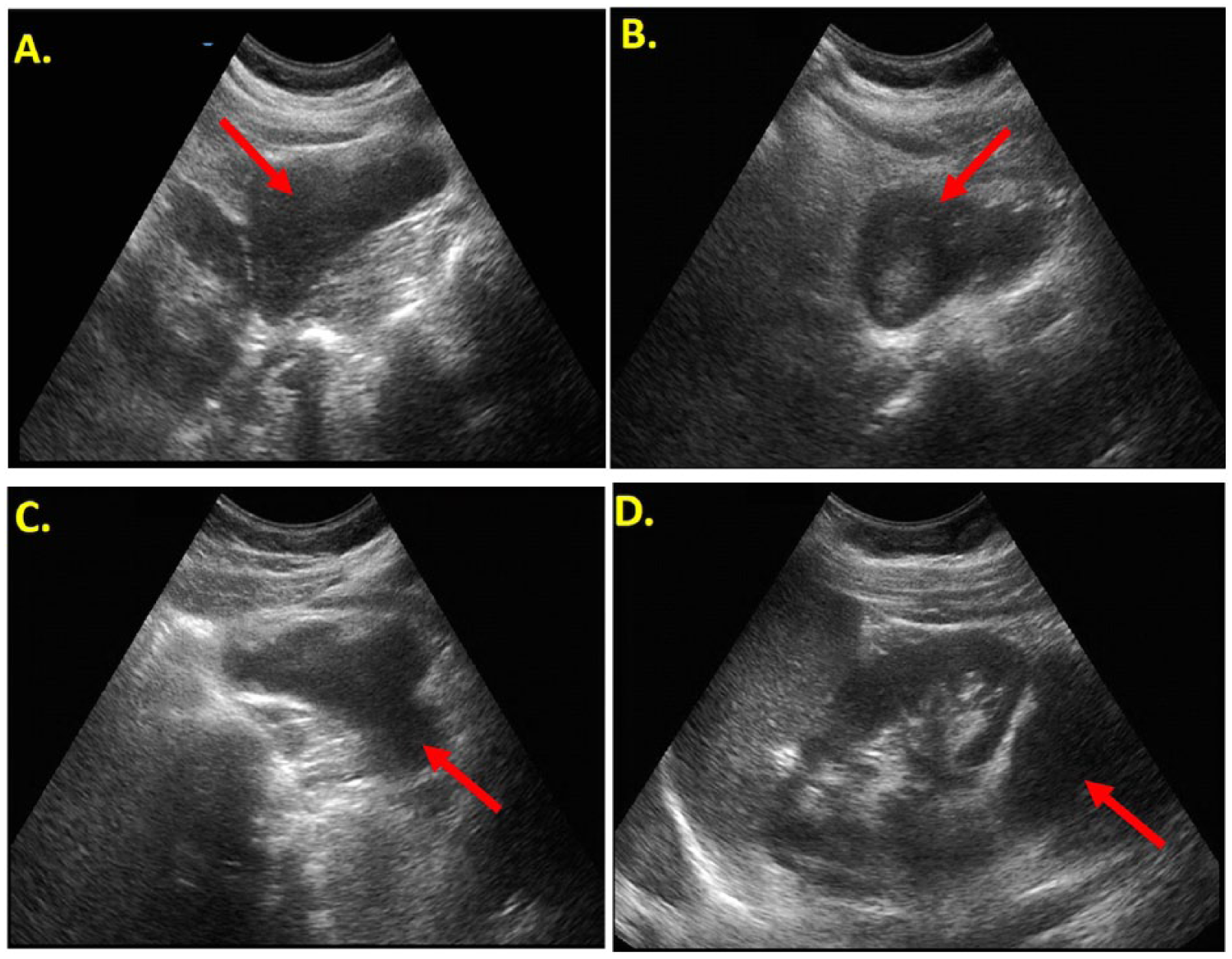
Gray-scale images of the left kidney and surrounding area. (A) Initial sagittal image showing an infrarenal mass (arrow). (B) Follow-up sagittal image showing the solid retroperitoneal mass (arrow). (C) Transverse image showing the mass and its lobulations (arrow). (D) Coronal image through the spleen and left kidney showing superior displacement of the kidney (arrow).
A computed tomographic (CT) scan was ordered 2 weeks later, which showed a lobulated, well-circumscribed mass that measured approximately 8.2 × 3.9 × 10.1 cm. (Figure 2A). The mass was predominantly hypodense, with only partial enhancement (Figure 2B), and abutted the left psoas muscle without clear signs of invasion. In addition, as noted in the sonogram, the mass caused slight superior displacement of the left kidney and posterior displacement of the left ureter (Figures 2C, 2D). No mesenteric or retroperitoneal adenopathy or ascites were noted.
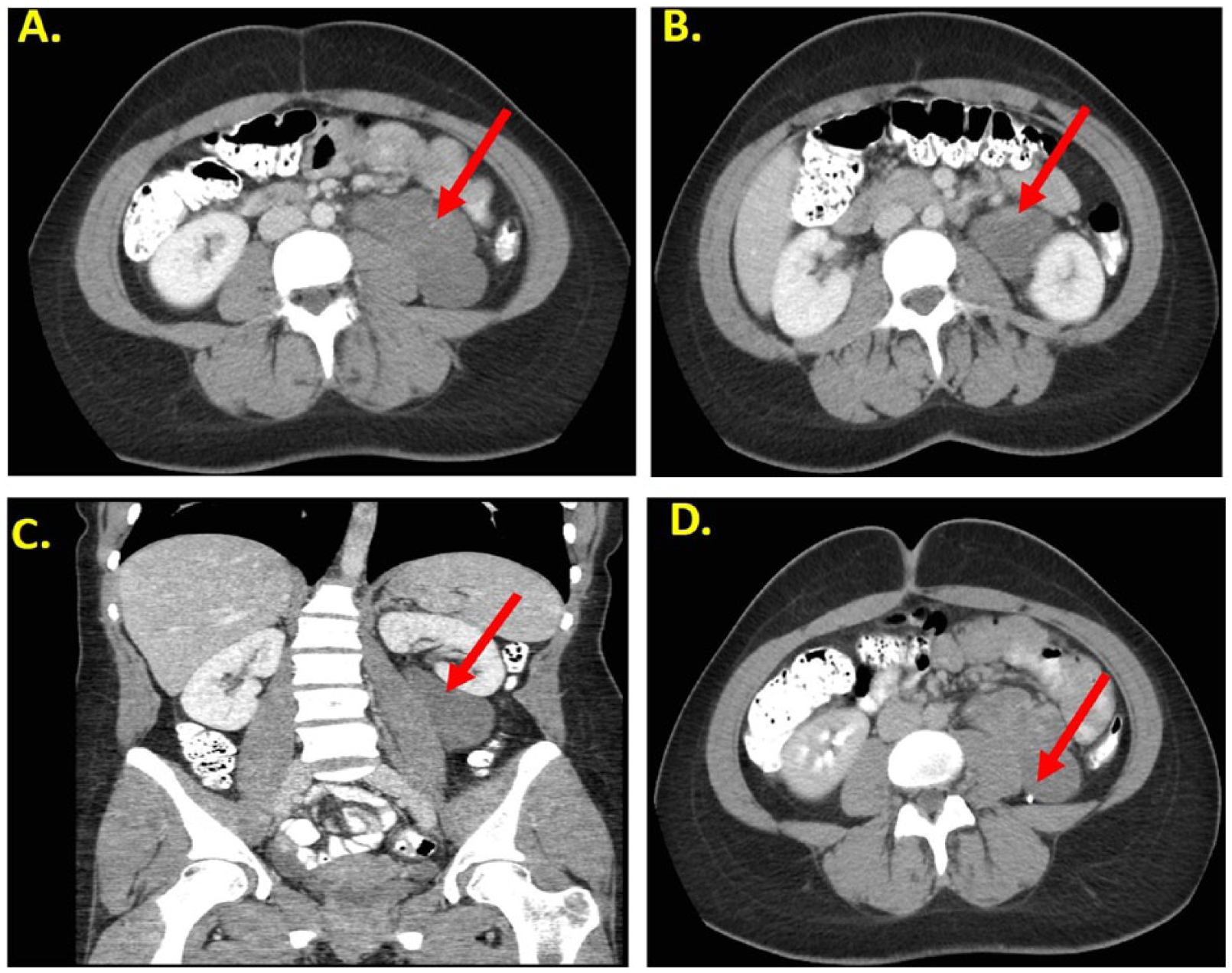
Computed tomographic (CT) images of the infrarenal retroperitoneal mass. (A) Axial cross-sectional image showing the lobulated, well-circumcribed mass (arrow) measuring 8.2 × 3.9 × 10.1 cm. (B) Enhanced axial CT image showing the predominantly hypodense mass with only partial enhancement (arrow). The mass can be seen to abut the left psoas muscle without clear signs of invasion. (C) Enhanced coronal CT image showing superior displacement of the left kidney by the mass (arrow). (D) Delayed enhanced axial CT image showing posterior displacement of the left ureter (arrow).
A CT-guided biopsy was done 9 days later that showed uniform morphology of predominantly neuromatous stromas with myxoid change and scattered mature ganglion cells. No evidence of malignancy, such as immaturity, significant cytologic atypia, mitoses, or tumor cell necrosis, were identified. Laboratory results did not show any abnormalities or reason to believe that the mass secreted catecholamines or steroid hormones. These findings were consistent with a diagnosis of a nonmalignant retroperitoneal ganglioneuroma.
Complete surgical resection of the mass occurred 13 weeks following the initial diagnosis. During the procedure, the ureters were found to be deep to the mass; however, the gonadal vessels went directly into the tumor itself. The mass was resected, and the procedure was well tolerated with no complications. An examination of the mass removed during surgery was done by 2 institutions, both confirming the previous diagnosis of a ganglioneuroma.
Discussion
Ganglioneuromas are rare, benign neurogenic tumors that arise from sympathetic ganglia. The tumors are composed of mature Schwann cells, ganglion cells, and nerve fiber. Ganglioneuromas may arise anywhere along the paravertebral sympathetic plexus and occasionally from the adrenal medulla. 2 Rare ganglioneuromas may undergo malignant transformation, including both de novo and those derived from maturation of a neuroblastoma. 3
The sympathetic nervous system, derived from neural crest, can lead to three types of tumors: neuroblastomas (most malignant), ganglioneuroblastomas, and ganglioneuromas (most benign). In accordance with normal anatomy, these tumors can arise anywhere the sympathetic nervous system populates, including but not limited to the neck, posterior mediastinum, adrenal glands, retroperitoneum, and pelvis. As ganglioneuromas are the most benign/mature of these tumors, they also appear the latest in life, typically from ages 10 to 40. They are identified on histology as a composition of ganglion and bundles of Schwann cells, 4 with >50% of the mass defined as Schwannian stroma-rich, a benign tissue. 5 Ganglioneuromas occasionally secrete hormones such as catecholamines, vasoactive intestinal peptides, or androgenic hormones. 6 The lack of significant primary research reflects the rarity of such tumors as only case reports were found upon a literature search.
Although there have been infrequent reports of ganglioneuromas in the central nervous system and mandible, the most common locations are the retroperitoneum (32%–52% of cases), posterior mediastinum (39%–43%), and cervical region (8%–9%).2,5,7 Within the retroperitoneum, the tumor is commonly seen along the paravertebral sympathetic ganglia (59% of cases) or, less commonly, in the adrenal medulla. 8 In the rare occurrence that these tumors present as gastric mucosa masses, further workup is warranted secondary to their association with multiple endocrine neoplasia (MEN) 2b syndrome.9,10 MEN2b syndrome describes a constellation of findings that can include pheochromocytoma, marfanoid-like findings, medullary carcinoma of the thyroid, and neoplasms of the eyes, mouth, and submucosa.
Due to their location and lack of early significant symptoms, retroperitoneal ganglioneuromas are often not discovered until they are more developed, with an average size at diagnosis of 8.0 cm (range, 2–25 cm). 11 They most frequently present with abdominal pain or palpation on physical examination. These large masses appear on CT or magnetic resonance imaging (MRI) as well circumscribed, oval, crescent, or lobulated masses. They can be extra-adrenal (59%) or intra-adrenal (41%) and will often surround major blood vessels but will have little or no compromise of the vessel lumen.2,12
Radiographic findings of ganglioneuromas have been described as well-circumscribed lobulated hypo-attenuating masses. Contrast enhancement is variable, while necrosis and hemorrhage is rare. 8 Ganglioneuromas can have discrete punctate calcifications in 20% to 30% of cases. 13 Sonographic appearance is usually nonspecific, demonstrating a heterogenous solid structure. 14 These masses are usually a concern because of their mass effect as well as the rare concern that they can transform into one of the more malignant tumors, a neuroblastoma or ganglioneuroblastoma. Treatment is surgical, and prognosis is considered good following resection. 11
Educational sonography programs not only provide an opportunity for students to gain hands-on experience with medical models but have the potential to identify pathology in asymptomatic volunteers. As such, sonography education programs should have the necessary protocols and procedures in place to respond to abnormal findings. These policies and procedures will provide for appropriate follow-up and management of incidental findings and provide the proper support for the medical model.
Conclusion
This report described a pathologic finding in an asymptomatic volunteer in an educational setting. The benefit of having policies and procedures in place for managing such findings was demonstrated. As a result, this infrastructure led to a diagnosis and treatment of a retroperitoneal ganglioneuroma.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.