
Abstract
While the common organs assessed in chest pain are the heart, lungs, and inferior vena cava, one must also consider other diagnoses. Splenic rupture can be either traumatic or atraumatic, and splenomegaly can make this vulnerable organ even more susceptible to injury. A case is reported of a patient who presented to the emergency department with a complaint of left-sided chest pain; a focused assessment with sonography for trauma (FAST) examination showed significant intraperitoneal free fluid consistent with splenic injury. The role of bedside sonography in acquiring a rapid and accurate diagnosis is discussed.
Introduction
Chest pain is a significant cause of mortality and morbidity in the United States and is one of the leading causes of admission and inpatient costs. 1 Bedside ultrasonography has become more widespread due to its ease and accessibility in the emergency department. While the common organs assessed in chest pain are the heart, lungs, and inferior vena cava, one must also consider alternatives or other diagnoses. It is established that ultrasound of the chest can diagnose many cardiac and respiratory disorders that are otherwise missed during admission. 1 One finds that in the setting of blunt abdominal trauma, a positive focused assessment with sonography for trauma (FAST examination) leads a patient directly to the operating room for exploration and repair of injuries with a high degree of sensitivity.2,3
Case Presentation
A 39-year-old male with a history of hypertension presented to the emergency department (ED) with left-sided chest pain noted over the past two hours. The pain was described as sharp and radiating up and down through his entire left chest in a crescent shape. It was associated with nausea but no other symptoms. He reported symptoms of an upper respiratory tract infection (URI) three weeks prior but otherwise had been in his usual state of health. Three days prior to his presentation, a bicyclist collided with the right side of his backpack. The bicycle did not hit his body, and he did not fall. He did not seek medical attention after the collision or mention it to the emergency physician, as he felt it was minor and non-contributory. His physical examination was unremarkable. The electrocardiogram (EKG) showed slight ST-wave elevation in the precordial leads, thought to be reflective of junction point elevation. His chest radiograph, complete blood count, basic metabolic panel, and troponin levels were all within normal limits. He was admitted to the observation unit for 24 hours and received aspirin as well as subcutaneous heparin for deep venous thrombosis (DVT) prophylaxis. During his hospitalization, he had a second negative troponin level and a normal echocardiogram. At time of discharge, his physical examination remained unremarkable, and he was noted to be pain free.
The patient returned to the ED two days later complaining of recurrent pain that was now more prominent in his left shoulder and radiating to his left flank. He was well appearing, and his vital signs, physical examination, and repeat laboratory tests were all within normal limits. A FAST examination (Figure 1) was performed, which showed a large amount of intraperitoneal free fluid. An abdominal computerized tomography (CT) scan was then obtained (Figure 2), which showed approximately two liters of free fluid in the abdomen and confirmed a splenic laceration. He was admitted to the surgical intensive care unit and soon after developed hypotension. When a repeat hematocrit of 21% was obtained, the patient was taken emergently to the operating room for exploratory laparotomy. A grade 3 splenic laceration was found, and a splenectomy was performed. The patient remained hemodynamically stable, and he was discharged on postoperative day five.
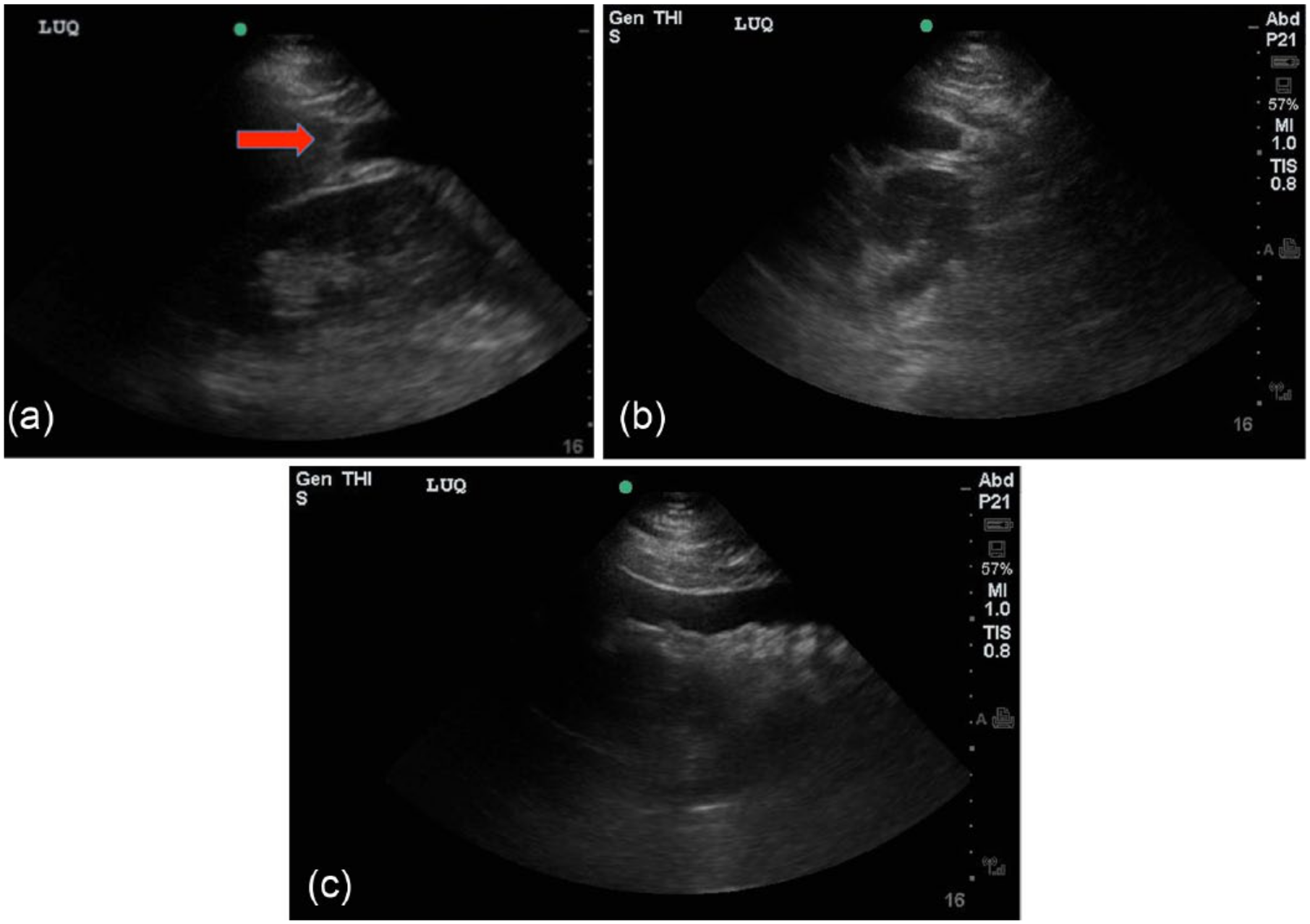
(a) Gray-scale image of the splenorenal interface in the longitudinal plane demonstrating intraperitoneal free fluid (arrow). (b) Gray-scale image of the splenorenal interface in the transverse plane. Free intraperitoneal fluid is again noted. (c) Grayscale image of the inferior pole of the left kidney demonstrating fluid tracking inferiorly into the left paracolic gutter.
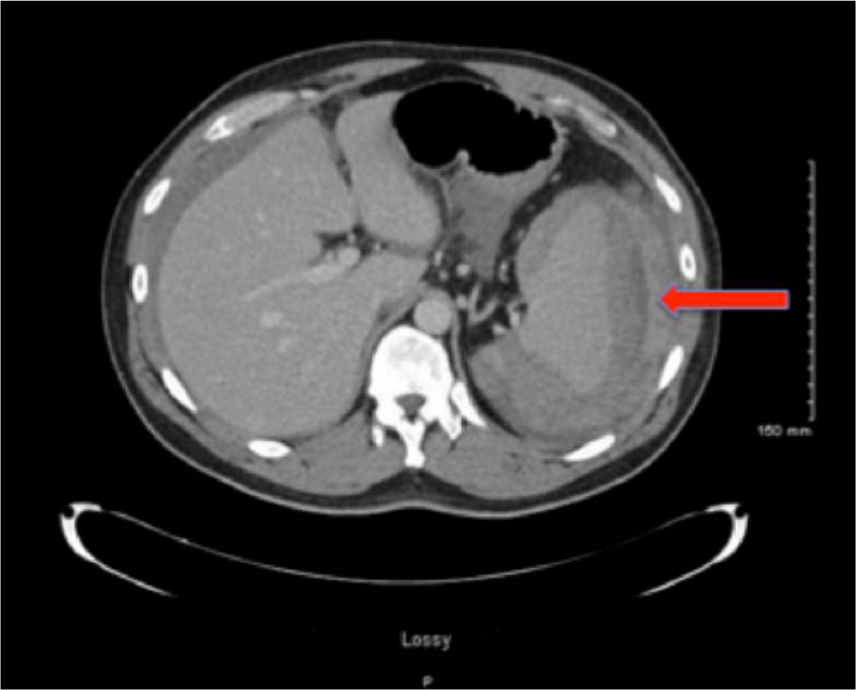
Contrast-enhanced cross-sectional computerized tomographic image of the upper abdomen showing significant fluid surrounding the spleen consistent with a splenic laceration/rupture.
Discussion
Splenic rupture can be either traumatic (most commonly due to blunt injury) or atraumatic (due to malignancy or infection). The spleen is the most commonly injured organ in blunt abdominal trauma. 4 Roughly 6% of blunt abdominal injuries are associated with splenic injury. 5 Injuries to ribs 9 to 11 are particularly concerning, as they are located just superficial to the spleen.
The mean splenic size is 150 g,6,7 with a mass above 250 g considered splenomegaly. Infection is the etiology of splenomegaly in up to 16% of cases. 8 Splenomegaly can make this vulnerable organ even more susceptible to injury.
In this case, routine echocardiography at the time of the first hospital visit was normal; as there was no attempt to evaluate the upper left quadrant, it did not demonstrate splenic pathology. At the second visit, the patient was initially well appearing and hemodynamically stable; however, after four hours, his hematocrit had dropped from 39% to 31%. The positive FAST exam showed prominent hypoechoic areas coursing down from the spleen, prompting an immediate surgical consult and CT scan. After CT showed a splenic laceration/rupture, the patient was admitted to the surgical intensive care unit 9 and soon after developed hypotension. When a repeat hematocrit of 21% was obtained, the patient was taken emergently to the operating room for exploratory laparotomy where a grade 3 splenic laceration 10 was found and a splenectomy was performed.
The resected spleen weighed 290 g (Figure 3), almost double the average splenic mass. 11 It was suspected that the splenomegaly was the result of a viral infection corresponding to the URI symptoms the patient had described, and that in this setting, his seemingly minor traumatic injury caused a splenic laceration. In addition, the anti-platelet agents and DVT prophylaxis he received during his initial evaluation for chest pain could have contributed to further bleeding and accumulation of subcapsular blood (Figure 4).
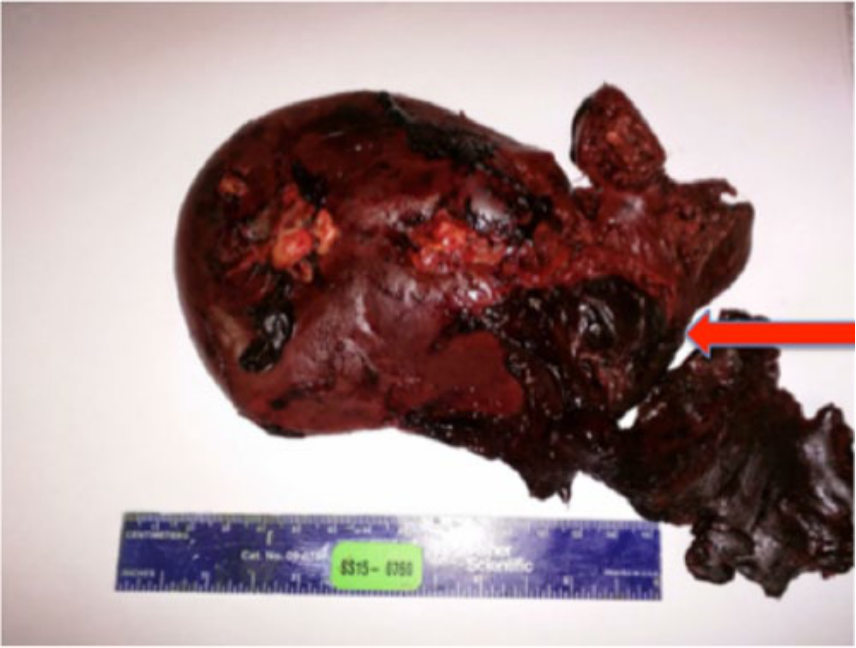
Photograph of the gross pathologic specimen of the enlarged spleen showing the laceration and some of the associated hematoma.
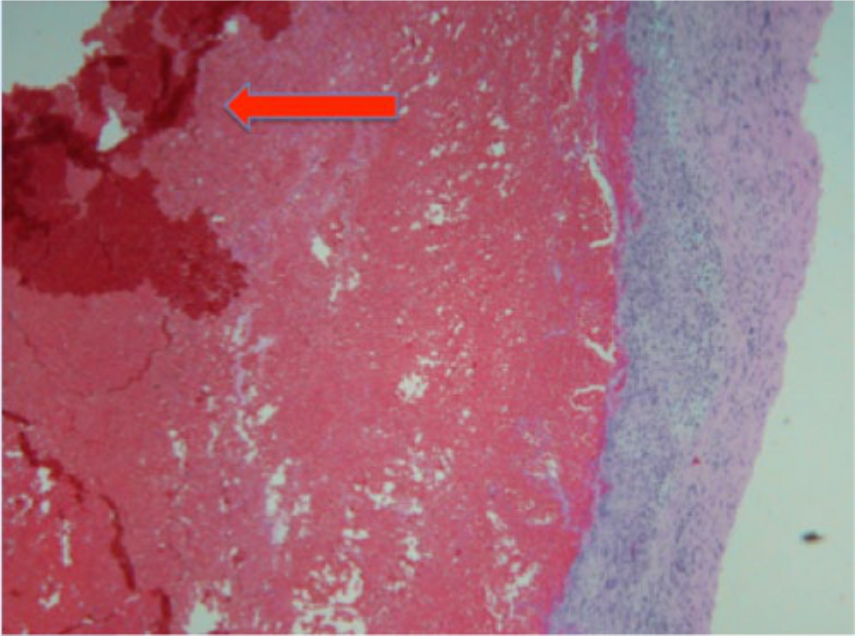
Microscopic histologic specimen (hematoxylin and eosin stain, ×100) from the resected spleen showing the capsule of the spleen with a large subcapsular hemorrhage (arrow).
This case illustrates several learning points. The first is to maintain a broad differential when evaluating patients with chest pain. It is natural to focus on pathology related to the heart and lungs, but any abdominal process that causes diaphragmatic irritation may also present with isolated chest or shoulder discomfort. The second is to avoid “anchoring bias,” a cognitive error in which a sonographer or physician “anchors” on a certain organ system or diagnosis and may fail to readjust in the face of evidence supporting an alternate explanation. Once the patient in this case report was labeled a “chest pain patient,” it may have become more difficult for clinicians to look beyond a cardiopulmonary etiology. In this case, the treatment that the patient received during his initial observation, which was appropriate for the management of chest pain potentially due to acute coronary syndrome, actually could have adversely affected his true pathology. This also applies to return visits to the ED. It is important to start fresh when evaluating “bouncebacks,” avoid anchoring on the previous diagnosis, and consider casting a wider net diagnostically. Ultimately, some cases are difficult to diagnose and may be missed on the first or even the second visit, but by avoiding these common errors, we may minimize risk to the patient and make the correct diagnosis even in a highly atypical presentation.
Conclusion
A case is reported of a patient who presented to the emergency department with a complaint of chest pain. The initial workup ruled out cardiopulmonary pathology. Other possible causes were not investigated until after the patient presented a second time with increasing symptoms. A FAST examination was able to rapidly demonstrate intraperitoneal free fluid, leading to the diagnosis of a splenic injury and appropriate surgical management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.