
Abstract
The objective was to assess the consensus among sonographers that the quality of abdominal ultrasound (US) images is related to the patient’s body mass index (BMI). Fourteen sonographers completed a 12-item questionnaire to evaluate their experience with abdominal US imaging with respect to image quality in correlation with the patient’s adipose tissue. Of the sonographers sampled, 85.7% agreed that there is an association between the amount of adipose tissue on a patient’s abdomen and the quality of US image obtained; 85.7% also agreed that a normal BMI of 18.5 to 24.9 provides the best US image. However, only 28.6% agreed that normal amounts of adipose tissue produce poor image quality. There appears to be agreement among sonographers that BMI is a factor in obtaining good quality abdominal US images. The general consensus was that the best abdominal US images were obtained in patients with normal BMI, whereas images obtained from patients with BMI 30.0 to 34.9 and to a lesser extent BMI 25.0 to 29.9 were limited in quality.
Abdominal ultrasound (US) examinations are increasingly being used as a noninvasive and inexpensive imaging modality. 1 Additionally, point-of-care US has been used by nonradiologists of various specialties including emergency medicine, critical care medicine, and surgeons at the bedside.1-8 However, the body habitus of patients who may be the best candidates for this examination and the limitations of abdominal US imaging in the nonpregnant patient have not been well defined. Other imaging modalities have been extensively researched in this regard. For example, difficulties in obtaining diagnostic-quality images in obese patients have been documented for mammography, 9 chest computed tomography (CT) for evaluation of pulmonary embolism, 10 and combined positron emission tomography–CT. 11
A retrospective study evaluating radiology report qualifications attributable to patient body habitus in abdominal US demonstrated a positive correlation between the increased number of habitus-limited reports and the increased prevalence of obese individuals in Massachusetts between 1991 and 2001. 12 However, in an associated project by our team, physicians trained in sonography were asked to evaluate transmitted extended-Focused Assessment with Sonography for Trauma (e-FAST) images. It was hypothesized that a linear relationship between patient BMI and US image quality would occur. The physicians consistently rated the US images of overweight (BMI 25.0-29.9) patients as having the best quality and the images of obese patients (BMI ≥ 30) as having the worst quality; the images of patients with normal body weight were considered to fall in the middle in terms of quality. This unexpected result led to a literature search that found a paucity of research in US image quality and patient body habitus. To further investigate this result, a short survey was developed for sonographers to determine their opinions on the relationship of body habitus and US image quality. We report the results of that survey here.
Methods
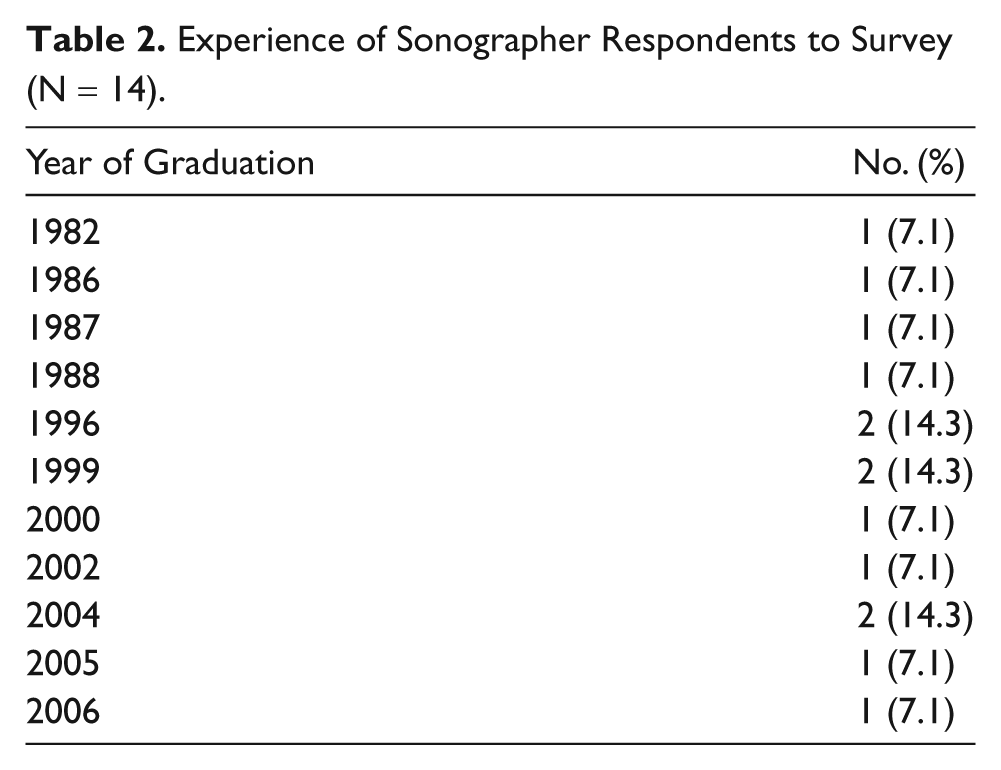
To examine the level of correlation between BMI/amount of adipose tissue and the quality of US images obtained, we conducted a survey of sonographers. Internal review board approval was obtained before sonographers were enrolled in the survey. A questionnaire was developed consisting of 12 items. Items were designed to assess for consistency between participants’ responses. Most of the items were scaled from 1 to 9 (disagree to agree) and pertained to the technologists’ personal experience. The survey items were related only to adult abdominal US examinations using an Acuson Sequoia 512 model with a 4V1 vector probe performed at this institution. Each of items 3 through 11 was rated on a 9-point Likert scale based on four definitions of BMI provided (Table 1). The terms defined in each category were used interchangeably to look for consistency. A score of 1 was the lowest agreement in each category and 9 was the highest agreement. The responses were collapsed into three groups: disagree (1, 2, 3, 4), neutral (5), and agree (6, 7, 8, 9). Fourteen sonographers of varying experience at our institution, an adult hospital, were surveyed. All the participating sonographers had more than 5 years of clinical experience, having graduated within the previous 7 to 30 years (Table 2). There was 100% participation and response rate to all items. The participants were not compensated; however, the approximately 5 to 10 minutes spent on the survey occurred during their normal working hours. The surveys were administered in a standardized and consistent manner by one of the investigators.
Definitions of Body Habitus

Experience of Sonographer Respondents to Survey (N = 14)
Statistical Analysis
All categorical data were presented as frequencies (percentages). The consensus of participants was demonstrated by their consistency in answering the contrapositive items; the level of agreement was examined with weighted kappa coefficient (κw) and a corresponding 95% confidence interval (CI). Agreement was examined using the following standards (Landis and Koch) for strength of agreement for the kappa coefficient: 0 = poor, 0.01 to 0.20 = slight, 0.21 to 0.40 = fair, 0.41 to 0.60 = moderate, 0.61 to 0.80 = substantial, and 0.81 to 1 = almost perfect. The items were grouped for evaluation of agreement based on the following groupings. Responses on items 4, 8, and 10 were assessed for agreement on normal BMI (small amounts of fat). Responses on items 5, 7, and 11 were assessed for agreement on overweight BMI (moderate fat). Responses on items 3, 6, and 9 were assessed for agreement on obese BMI (large amounts of fat). All data analysis performed in this study was conducted using SAS 9.2 (SAS Institute Inc, Cary, North Carolina).
Results
A summary of the responses from the 14 sonographers who participated in the survey is given in Table 3. There was agreement among 85.7% of responders that there is an association between the amount of adipose tissue on a patient’s abdomen and the quality of US images obtained. When participants were asked to specify which BMI provides the best image quality, 85.7% agreed that a normal BMI of 18.5 to 24.9 provides the best US image quality. However, 28.6% also agreed that normal amounts of adipose tissue produce poor image quality.
Summary of Responses to Sonographer Surveys
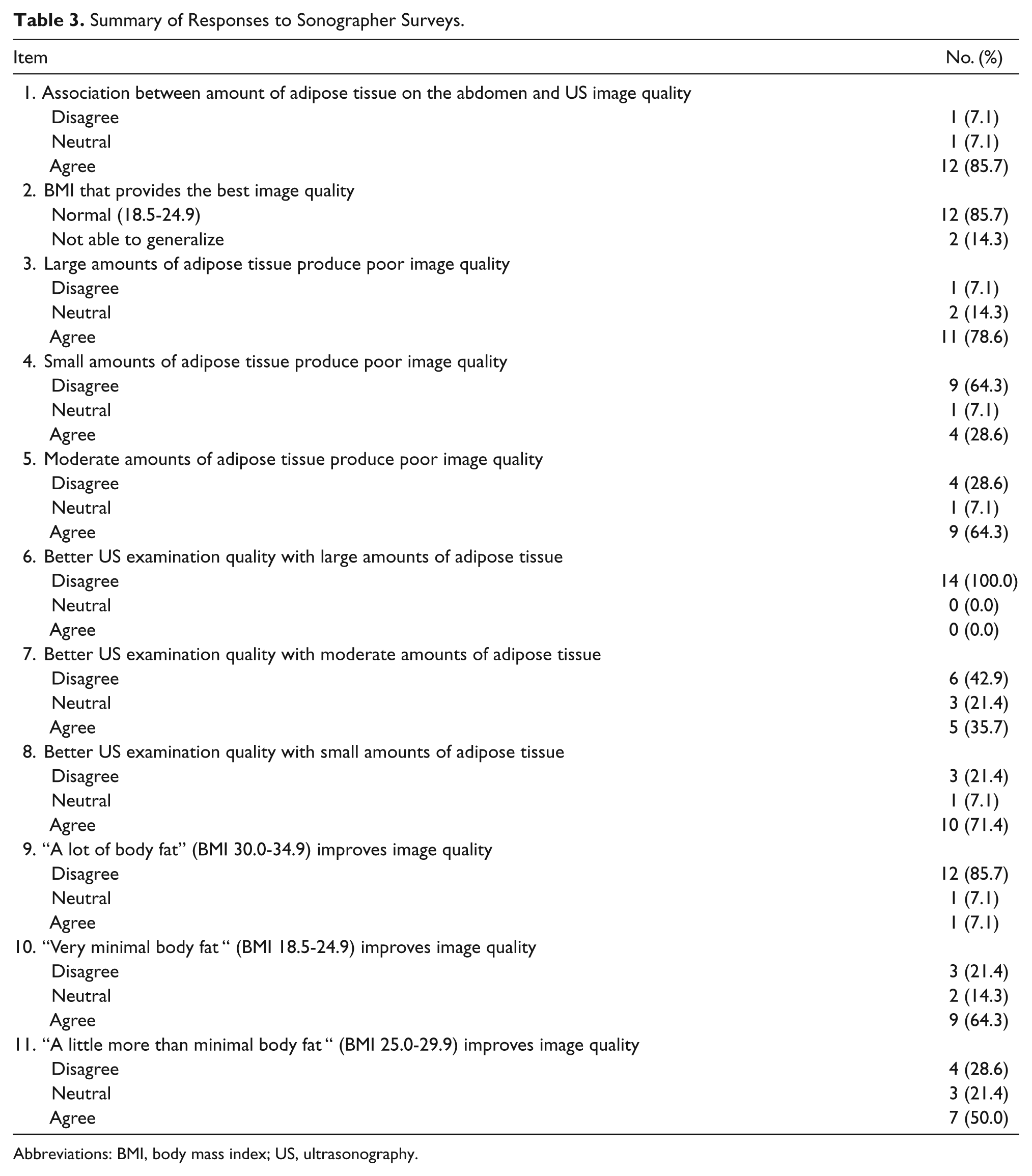
Abbreviations: BMI, body mass index; US, ultrasonography.
Results of the analysis of agreement between items on related characteristics are presented in Table 4. It is seen that for small amounts amount of fat, there was poor agreement (a consistent result) between items 4 and 8 (κw = −0.0957) and items 4 and 10 (κw = −0.1875). Items 8 and 10 reported moderate agreement (a consistent result) (κw = 0.5395). There was poor agreement (a consistent result) between the items regarding moderate fat, items 5 and 7 (κw = −0.2727), items 5 and 11 (κw = −0.2584), and items 7 and 11 (κw = −0.0316). With regard to large amounts of fat, agreement was poor (a consistent result) for the item. All sonographers reported disagreement with item 6 (large amounts of fat giving better image quality), with 9 of the 14 participants supporting (item 3) the perception that the quality of images was poor with large amounts of fat; items 3 and 9 reported a poor agreement (a consistent result) (κw =0.0329). Items 6 and 9 had strong agreement/consistency since 12 of the 14 technologists reported “disagree” on both items. The lack of agreement proves that the participants understood the items that were proposed in the survey. The results of this reliability study of the tool for assessing consensus between US technologists indicated that there was consensus on amount of adipose tissue and quality of image.
Analysis of Agreement Between Survey Items a
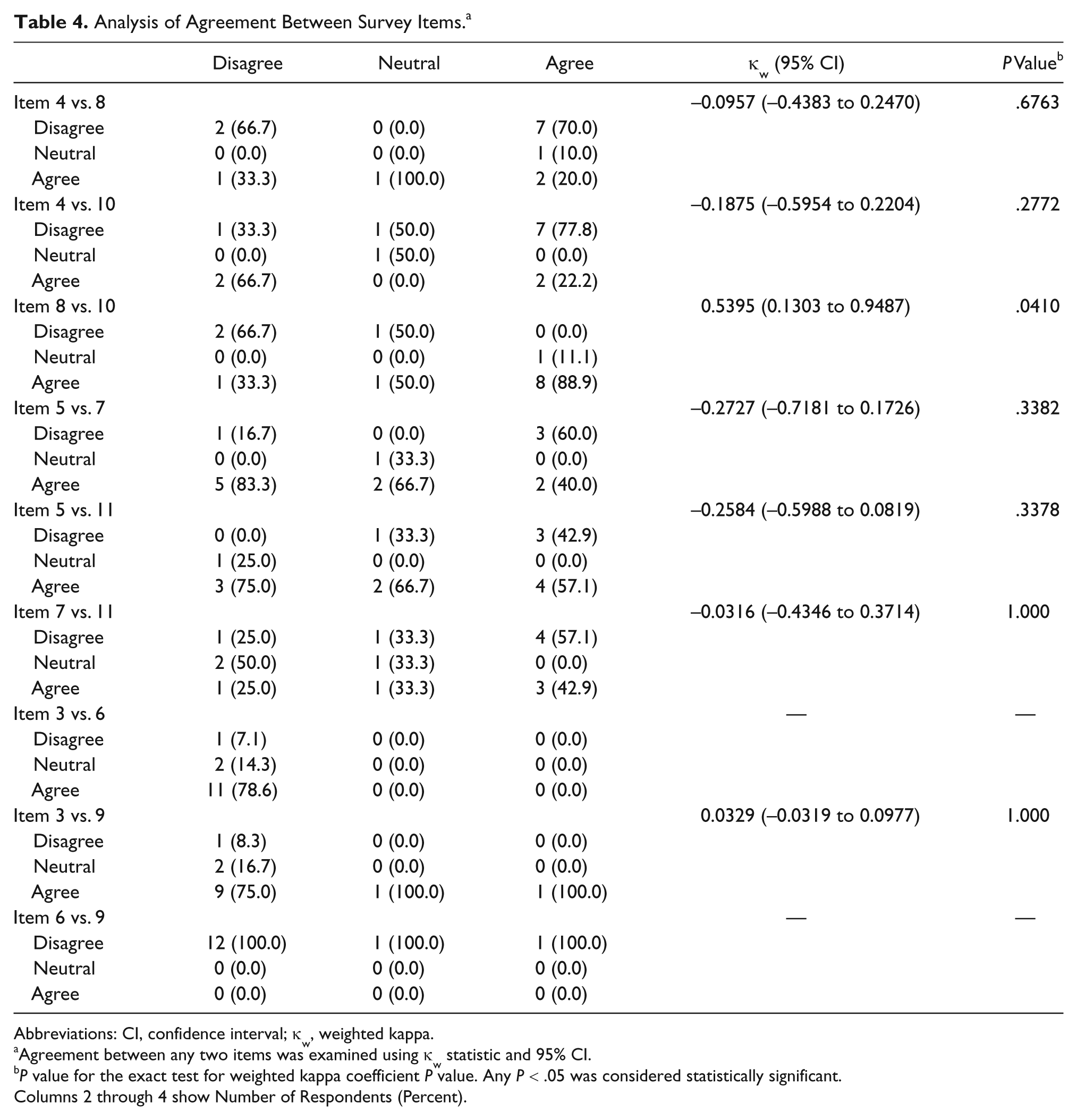
Abbreviations: CI, confidence interval; κw, weighted kappa.
Agreement between any two items was examined using κw statistic and 95% CI.
P value for the exact test for weighted kappa coefficient P value. Any P < .05 was considered statistically significant.
Columns 2 through 4 show Number of Respondents (Percent).
Discussion
A surprising finding was the discordance regarding normal BMI. Intuitively it may seem that absence of adipose tissue would provide the highest quality image, as this is typically the case in radiographic imaging. The poor agreement between items 7 and 11 was unexpected. These items were included to check for consistency and were expected to demonstrate agreement. This may be the result of misunderstood or unequal terminology. The descriptions of moderate amounts of adipose tissue and “a little more than minimal body fat” (BMI 25.0-29.9) may not have been considered equal in the opinions of the surveyed.
At the other extreme, most imaging specialists would expect to find imaging quality to be limited by obesity. However, we found the perception that small or normal amounts of adipose tissue rather than no body fat may result in better images. Several possibilities exist that would explain our results, including patient factors, definitions, techniques used, and examination factors. BMI considers the patient’s total body weight in relation to height. However, the location and concentration of adipose tissue vary from person to person. For example, women have an increased proportion of adipose tissue below the waist, whereas men tend to have more fat around the midline and intra-abdominally. 13 Ethnic differences also exist in adipose tissue distribution. 14 When imaging the abdomen with US, the location of the adipose tissue becomes an issue, especially if it is thickest over the area of interest, because fat may attenuate the US beam and diminish the image quality. 15 Another caveat involved with the distribution of body fat is that when a patient is supine, fat tends to spread out. Therefore, in the patient with moderate amounts of fat, the distribution of the fat may result in less fat over the abdominal organs of interest, providing better image quality in these patients.
In a patient with too little body fat, an entirely different problem arises. Adipose tissue is important in providing tissue interfaces to allow good differentiation between organs. 15 In a patient with very little body fat, the differentiation between tissues or organs of similar density becomes difficult. This is best exemplified in the US imaging of children, in whom the lack of body fat is a common issue. 16
Technical factors may play an important role in explaining why patients with moderate amounts of fat seem to produce better quality images. A certain amount of body fat may provide better images because the US transducer hardware and mathematical algorithms are designed to optimize images of the general population, as was demonstrated by Scabia et al. 17 Given that all equipment does not use the same algorithms and hardware, image optimization depends on the specific equipment, software, and hardware. For example, a statistically significant difference exists between images obtained with a common portable US machine and those obtained with a more expensive, larger US machine when typical views used by emergency physicians are compared. 18
Ultrasound hardware has been adapted for differences in body density and mass. The higher the frequency transducer, the more attenuation will take place and the less penetration. 15 Therefore, when an obese patient is imaged, a lower frequency transducer may be necessary to reduce the attenuation and allow deeper penetration of the US beam. The software will adjust the images as well, boosting those signals that take longer to return in order to provide a brighter image of those areas, taking into account physiologic factors such as variations in tissue density. For example, in a study by Pinton et al., 19 a numerical algorithm was developed to simulate a diagnostic US pulse propagating through a histologically measured representation of human abdominal wall with spatial variation in the speed of sound, attenuation, nonlinearity, and density. 19
Sonographers may be better able to manually adjust the US technology to best accommodate normal patient body type (BMI 18.5-24.9) with skill and experience. Research has indicated that superior technical abilities are needed to obtain high-quality images. In a study by Jang et al., 20 it appeared that physicians acquire the ability to interpret Focused Assessment with Sonography for Trauma (FAST) images earlier than they acquire the technical skills required to perform the examination. By extrapolation, the skills acquired by experienced sonographers to perform and obtain high-quality images may allow them to adapt their scanning technique to a patient’s BMI and quantity of adipose tissue. 21 The use of varying angles, pressures, and transducer types is learned with experience and may allow sonographers to obtain high-quality US images in such a way that the patient’s body type becomes less relevant.
Furthermore, BMI is commonly used to measure obesity; however, it is quantified in ranges with arbitrary cutoffs. Is a BMI of 24.9 actually different than a BMI of 25.0 when only a couple of pounds can move a person from one category to the next? This should be considered when categorizing patients based on BMI. The definitions used to assess adipose tissue quantity in relation to other soft tissues may be flawed. 22
The following limitations of this pilot study are recognized. A relatively small sample size was used, though the setting was a 775-bed adult hospital with 100% sonographer participation. Including sonographers from several hospitals would have increased our sample size and eliminated any biases created by using just a single institution. We did not specifically evaluate the question of “too thin” in our survey, although some survey participants commented that good abdominal US images are never obtained for excessively thin people and that the best images are obtained for people of normal weight or those with small amounts of fat. Additionally, standard definitions, such as good versus poor image quality, were not provided as a baseline and may have affected those surveyed based on their preconceived opinions. To the same effect, the classification and descriptions of BMI were not specifically provided other than as worded in the questionnaire (see Table 1). The survey also did not specify what type of US imaging was in question, so opinions may have been biased toward the modality most commonly used by the particular sonographer. For example, tissue harmonic US imaging produces higher quality images than conventional sonography. 23 If the respondent’s perception was attributable to lack of definitions, further research with attention to consistency and well-specified definitions may be useful to correct this conflict. Finally, more qualitative inquiries of the sonographers would have yielded additional responses on the reasons why the sonographers disagreed, thus yielding some avenue for additional work. Unfortunately, we did not collect such data in this study.
Of note, the results from this pilot survey suggest a likely consensus that normal amounts of body fat (BMI 18.5-24.9) are best to obtain high-quality abdominal US images, a finding that is in conflict to some extent with the finding of the e-FAST study, in which physician raters determined that a BMI of 25.0 to 29.9 (overweight) was best. This variation in results makes evident the need for further investigation of BMI and its correlation to high-quality abdominal US imaging with careful attention to precise definitions.
Conclusion
There appears to be agreement among sonographers that BMI is a factor in obtaining good quality abdominal US images. There was a general consensus that a small amount of body fat (normal BMI) was best whereas a large amount of body fat (BMI 30.0-34.9) and to a lesser extent a moderate amount of body fat (BMI 25.0-29.9) were detrimental in obtaining good quality abdominal US images. Of the small number of sonographers surveyed, 71% believed that small amounts of adipose tissue are better whereas 79% agreed that large amounts of adipose tissue produce poor quality abdominal US images. In verbal interviews with the sonographers taking the survey, the majority mentioned that images of a patient who is too thin are poorer than images of a patient with normal body weight.
Further research is needed to evaluate how best to use US imaging in patients of varying body types and amounts of adipose tissue. It is possible that US is not the best choice of imaging in certain patients. There may also be better technology, such as more innovative transducers or software, to obtain and produce high-quality abdominal US images in patients with varying amounts of adipose tissue. A larger study evaluating patient BMI, specifically relating to location and amount of abdominal adipose tissue in correlation with abdominal US image quality, may allow better options for imaging the abdomen in the increasing population of obese patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding received Department of Defense Contract Funds, Grant HDRTA1-09-C-0059 Under the Defense Threat Reduction Agency (DTRA) of the Department of Defense (PI: Joseph Feldman, MD).