
Abstract
Urethral bulking is an office procedure for treatment of stress urinary incontinence that has increased in popularity in recent years. Numerous types of urethral bulking agents have been used since its introduction in the 1930s. Typically, these agents are imaged using specialty 3D 360° field-of-view transducers; however, a sonographer, during a pelvic or renal examination, may inadvertently find and image an echogenic structure near the urethrovesical junction in patients with a history of urethral bulking. Familiarizing oneself with the sonographic appearance of urethral bulking agents and optimizing techniques to obtain improved images of these agents may eliminate the need for additional imaging for the patient. Urethral bulking can be readily imaged with transducers commonly found in most ultrasound departments. This review will focus on the sonographic characteristics of urethral bulking agents and knowing when and how to use appropriate transducers to image the urethra.
Keywords
Introduction
Stress urinary incontinence (SUI), the involuntary loss of urine, is a common condition that affects adult women.1,2 The etiology of SUI is still not completely known. 3 Although there are numerous procedures to treat SUI, urethral bulking is considered minimally invasive and has recently increased in popularity. 4 In an attempt to achieve urethral coaptation and alleviate SUI, a bulking material can be injected into the proximal tissue of the urethra (Figure 1). Sonography is the method of choice for imaging urethral bulking material. Collagen was the urethral bulking material used for years, but it lacked longevity and required reapplications. More recently, the materials used are polymers that display distinct echogenic characteristics by sonographic imaging. 1 Bulking agents can be seen sonographically near the urethrovesical junction, but to the untrained or inexperienced observer, an image of an echogenic structure at the urethrovesical junction on a pelvic or renal sonogram may warrant the need for additional imaging. If a sonographer were knowledgeable about urethral bulking and acquired additional enhanced images of the area, this would obviate the need for supplementary imaging such as computed tomography (CT) or magnetic resonance imaging (MRI), which cannot image the urethral bulking material as well as a skilled operator using sonography.
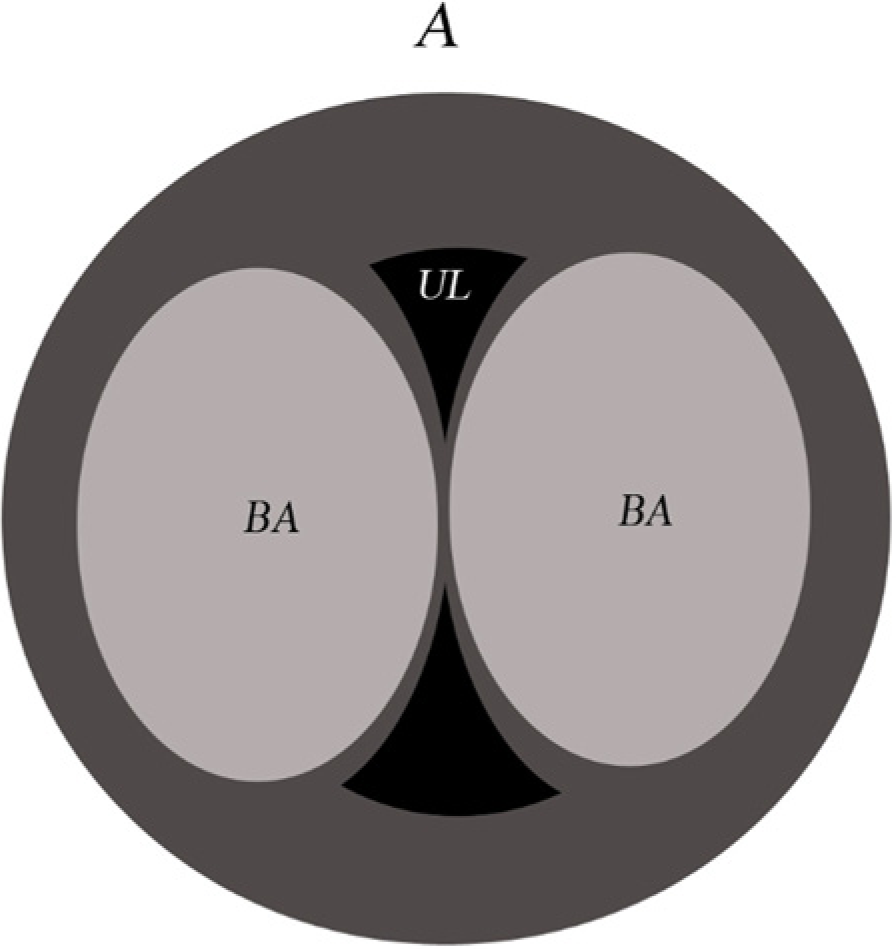
Schematic image of a transverse view of a urethra following a urethral bulking agent injection. A, anterior; UL, urethral lumen; BA, bulking agent.
History
Sclerosing agents, sodium morrhuate, and paraffin were initially used when urethral bulking was introduced in the 1930s. These agents did not prove to have good long-term outcomes. Teflon, collagen, and autologous fat were later attempted, but similar to the previous agents, Teflon and autologous fat had unfavorable outcomes. Collagen was long considered the gold standard in urethral bulking. 3 As with injection of collagen elsewhere in the body, there was a concern for disintegration requiring additional injections. Today, there are several bulking agent options to choose from. Some of the more popular agents available are silicone, calcium, zirconium, polyacrylamide, or collagen based. 3 The decision to use one bulking agent over another is typically determined by physician preference and is often based on the availability, cost, and ease of use of the agent. 1 To date, the ideal bulking agent, one that would be biocompatible and durable over a significant time, has not been developed. 1
Urethral Bulking
There are two standard methods of urethral bulking: periurethral and transurethral. 4 Both can be performed in the office setting. 1 Reports of efficacy of one method compared to the other are conflicting. Some claim that the transurethral route produces improved efficacy and durability and lower postoperative urinary retention rates, 1 whereas others claim that the two procedures are equally efficacious. 4
Although not as efficacious as the surgical sling procedure for SUI, urethral bulking is appealing for multiple reasons. 1 As mentioned earlier, urethral bulking can be performed in the office setting, offering significant savings for patients in time and expense. After a surgical sling procedure for SUI, another sling procedure may not be advisable or even feasible. Elderly, medically frail patients make up a substantial percentage of SUI patients and they may benefit from a minimally invasive alternative. Women who are interested in child bearing or professional women who do not want to lose time from work might also find urethral bulking a good alternative. 3 The ease of use and low complication rate make urethral bulking an appealing alternative to surgery. 4
Imaging
The ultrasound signal produced by the bulking agents varies depending on the makeup of the agent. Collagen-based bulking agents vary between hypoechoic, isoechoic, and hyperechoic. 5 The signal from a calcium-based agent will produce a hyperechoic structure on the image near the urethra 6 (Figure 2). Bulking deposits vary in size and shape. A well-placed bulking agent should appear round or oval in shape, whereas a poorly distributed bulking agent may track along the urethra. An agent tracking along the urethra will have the same echotexture but will appear elongated (Figure 3).
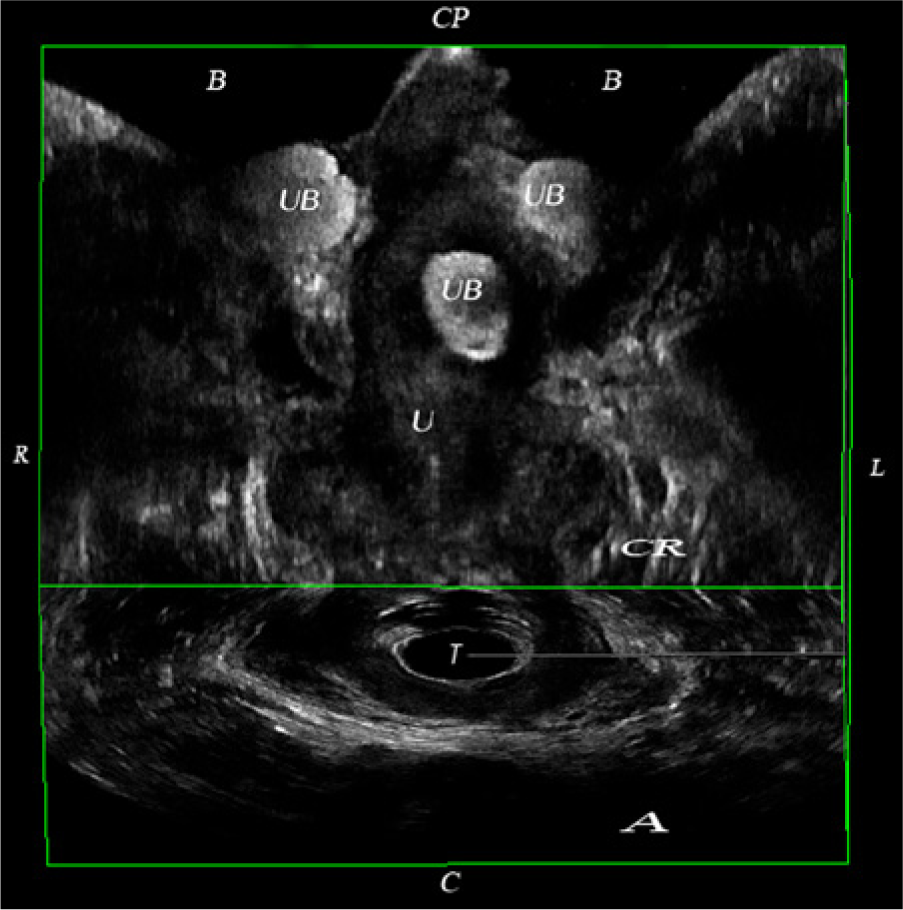
Coronal view obtained using an endovaginal transducer of a 3D volume demonstrating a urethral bulking agent. B, bladder; UB, urethral bulking agent; U, urethra; T, transducer; C, caudad; CP, cephalad; R, right; L, left; CR, coronal view; A, axial view.
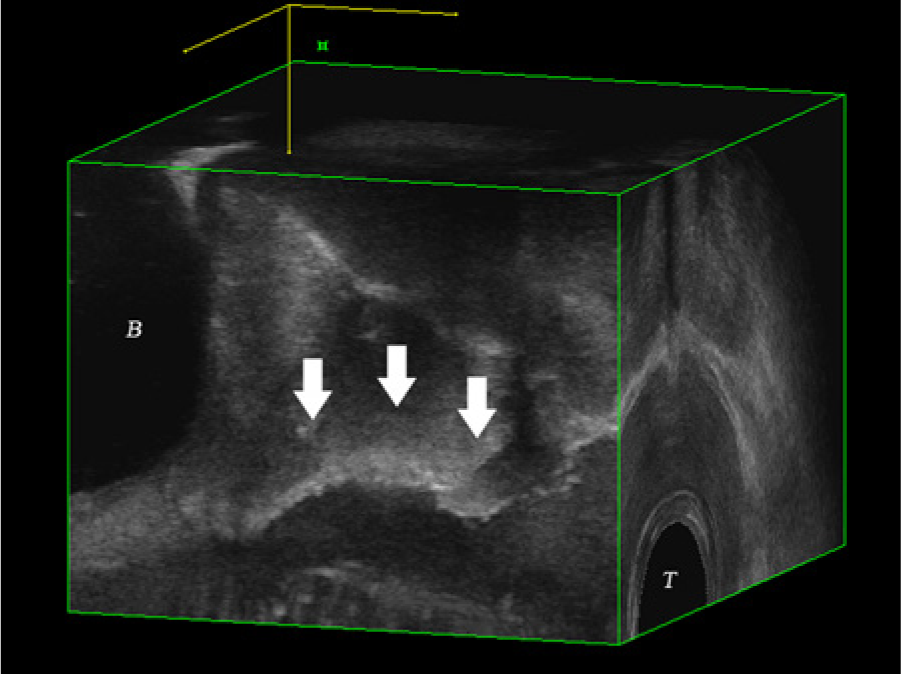
Right sagittal view of a 3D volume showing the urethral bulking agent tracking along the urethra (white arrows). B, bladder; T, transducer.
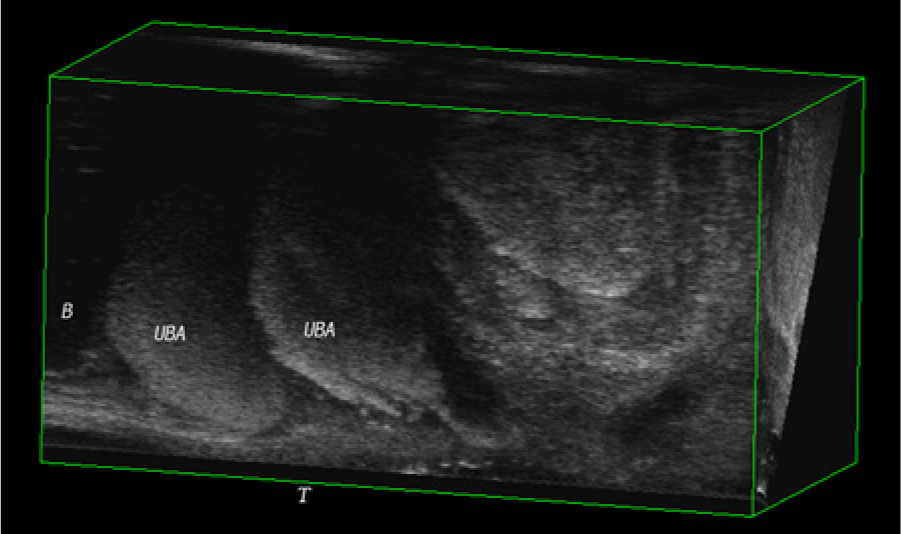
Because of the irregular and varying shape that bulking agents take after injection, 3D sonography is ideal for imaging as opposed to a purely cross-sectional modality. 5 Offices specializing in pelvic floor disorders may have specialty 360° field-of-view 3D endovaginal transducers not widely available in more general imaging departments. The only companies currently manufacturing such transducers are BK Medical (Peabody, Massachusetts) and Hitachi-Aloka (Tokyo, Japan). These are high frequency transducers to provide good image resolution. Some are biplane probes obtaining images with both linear and perpendicular arrays, whereas others are 360° field-of-view probes that obtain the images axially; urethral bulking agents can be seen clearly with both (Figures 4 and 5). Whereas superior images can be obtained with specialty transducers, urethral bulking agents also can be imaged well with transducers commonly found in most ultrasound departments.
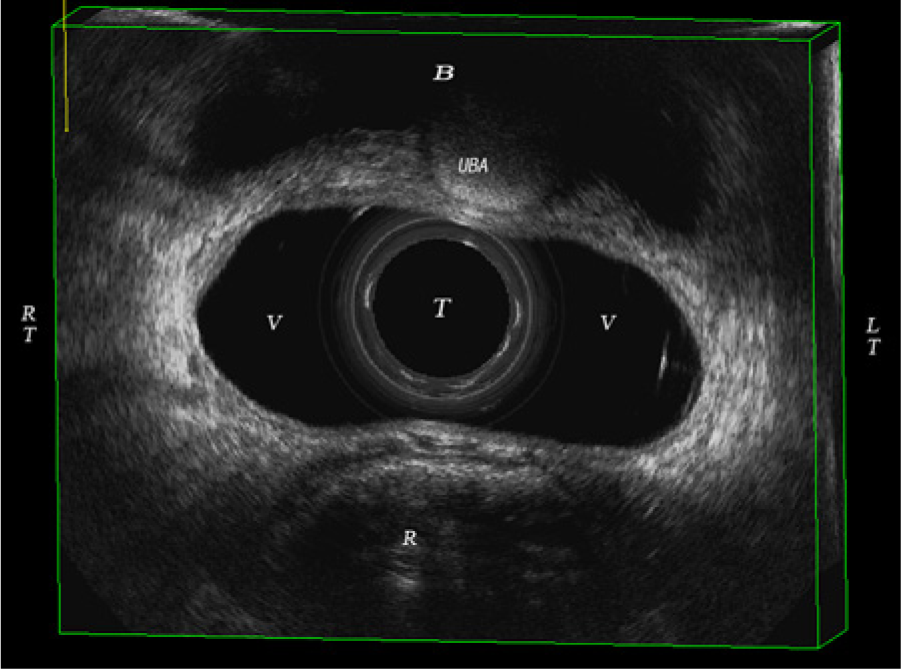
Axial view of a 3D volume obtained using an endovaginal transducer placed above the level of the urethrovesical junction showing a urethral bulking agent. B, bladder; UBA, urethral bulking agent; T, transducer; V, vagina; R, rectum; RT, right; LT, left.
Sagittal view of a 3D volume obtained using an endovaginal transducer showing a urethral bulking agent. B, bladder; UBA, urethral bulking agent; T, transducer.
Because of the increasing frequency of urethral bulking procedures, it is reasonable to expect that at some time a sonographer may unknowingly scan a patient posturethral bulking during a pelvic or renal sonogram. Although the bladder is seen on both transabdominal pelvic and renal sonograms, the urethra is not routinely imaged on either study. Urethral bulking agents can mimic a bladder stone when imaged transabdominally with a convex transducer (Figure 6). If a questionable echogenic structure is seen transabdominally, additional imaging such as CT or MRI may be ordered. Given that sonography is the method of choice for imaging urethral bulking agents, a few questions about the patient’s past medical history and a few additional sonographic images may spare the patient the expense, inconvenience, and anxiety of additional imaging with another modality.
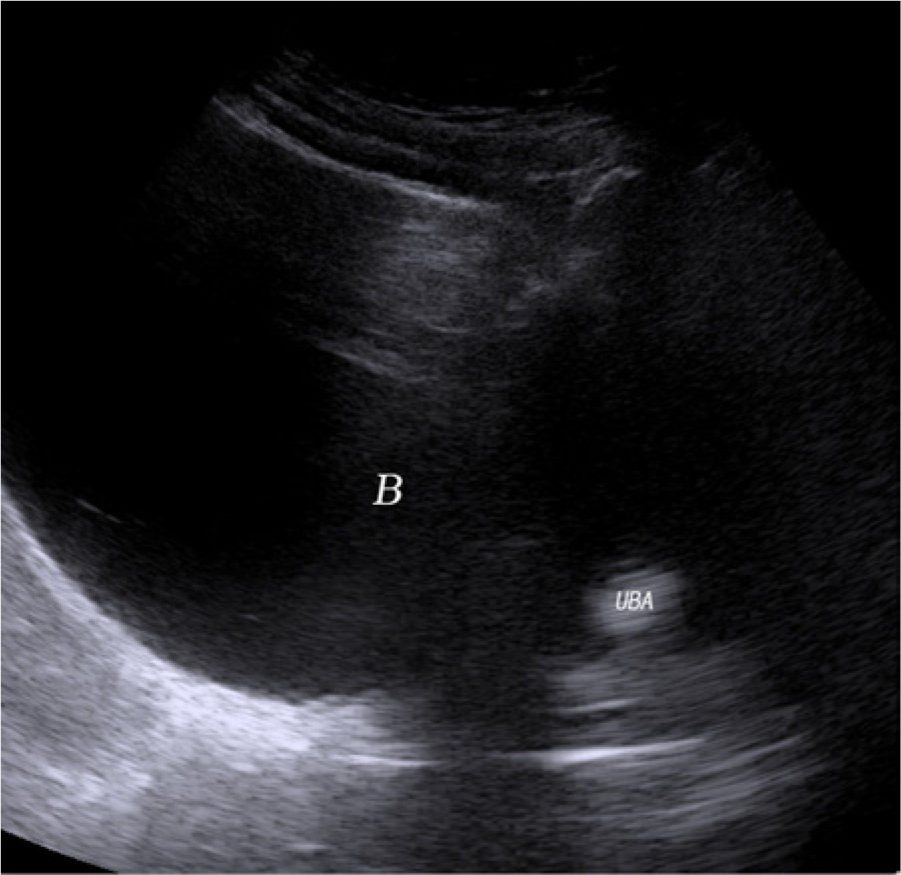
Sagittal transabdominal image of an echogenic urethral bulking agent. B, bladder; UBA, urethral bulking agent.
Outside of specialists for pelvic floor disorders, few sonographers have significant experience with urethral bulking agents or procedures. If sonographers are knowledgeable about urethral bulking agents and the images they produce, they typically will be able to acquire the additional images necessary to avoid the expense and CT radiation exposure of follow-up imaging. The same curved transducer used for transabdominal pelvic and renal sonograms can be used transperineally to image the urethra. The patient should be scanned in the lithotomy position as when scanning transvaginally. The transducer should be prepped in a similar fashion to a traditional endovaginal transducer. An ample amount of gel should be placed on the transducer and then covered with a transducer cover or glove; it is important to ensure that there are no air pockets between the cover and the transducer. After applying gel on top of the cover, the transducer should be placed on the perineum. Although tissue contact is required, care should be taken to avoid applying too much pressure. 2 The pubic symphysis, urethra, vagina, and rectum can all be seen clearly. The abdominal probes used for transperineal pelvic floor imaging display the image on the screen as designed for an abdominal probe (Figure 7), which is not the anatomically correct orientation for pelvic floor imaging. Most experts in pelvic floor imaging prefer that the transperineal image be displayed in a nontraditional orientation. 2 The image is inverted and reversed (Figure 8), as if the patient is standing, and obtained from the left sagittal plane. This orientation represents the female pelvis in the functional standing position (Figure 9). This is considered standard orientation in pelvic floor ultrasound imaging.
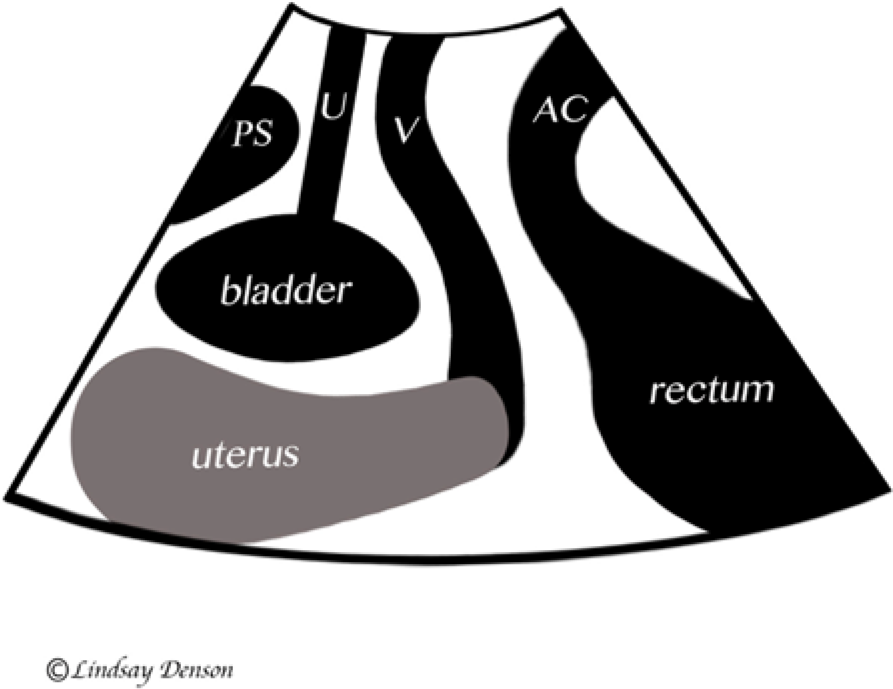
Schematic drawing showing the traditional transperineal sonographic orientation. PS, pubic symphysis; U, urethra; V, vagina; AC, anal canal.

Transperineal sonogram using the standard pelvic floor orientation showing an echogenic urethral bulking agent. AC, anal canal; UB, urethral bulking agent; PS, pubic symphysis.
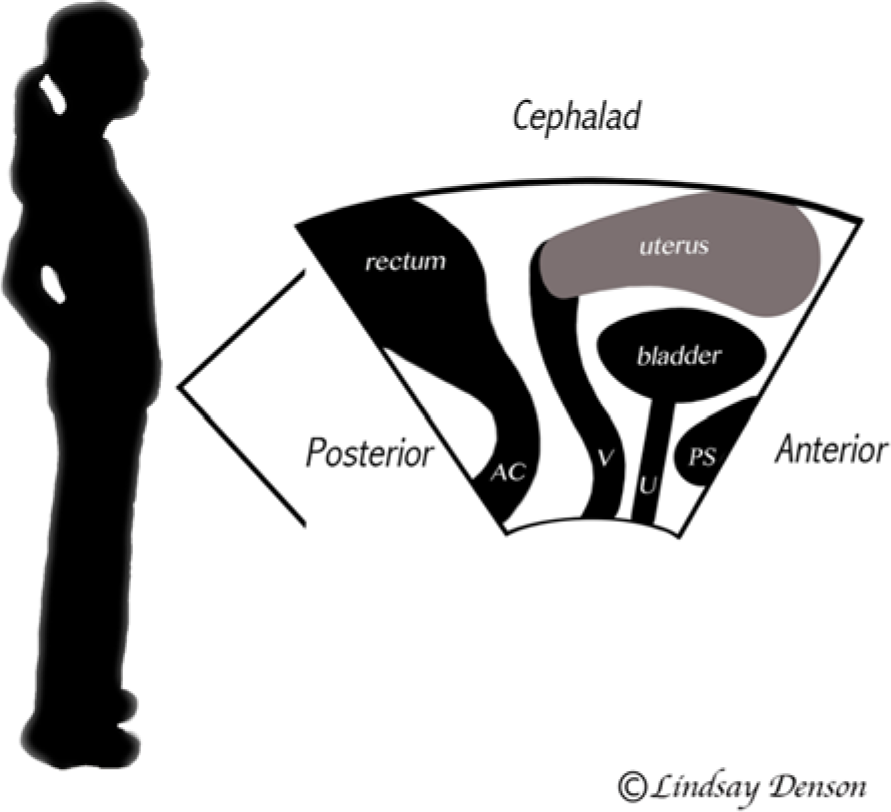
Schematic drawing of the standard orientation for transperineal imaging, demonstrating why experts in pelvic floor imaging prefer the traditional image inverted and reversed. AC, anal canal; V, vagina; U, urethra; PS, pubic symphysis.
End-firing vaginal probes typically used to image the uterus and ovaries can also be used to image the urethra and the bladder neck. Unfortunately, the urethra is typically bypassed completely as the pelvic organs are imaged. The transducer and patient should be prepped as usual for a traditional endovaginal sonogram. On insert, the transducer should be angled anteriorly, where the urethra and bulking agent can be clearly imaged (Figure 10).
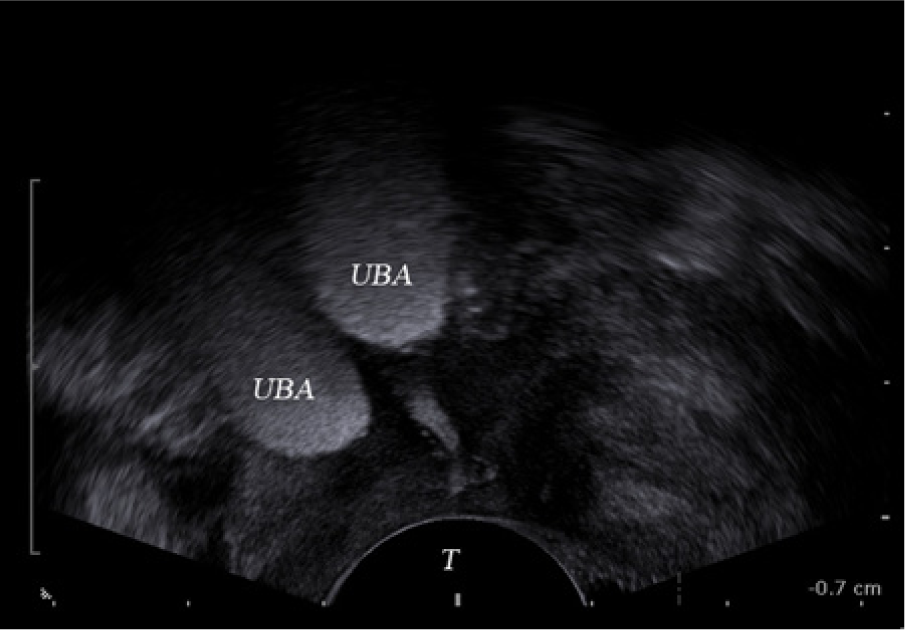
Sonographic image of a urethral bulking agent obtained with an end-fire transvaginal transducer. UBA, urethral bulking agent; T, transducer.
Conclusion
Urethral bulking is an appealing alternative to the surgical sling procedure for SUI. Popularity of this procedure is likely to continue to grow as improved bulking agents become available, and sonographers may start to see suspicious echogenic structures at the base of the bladder more frequently when scanning transabdominally. With proper imaging, urethral bulking agents produce a distinct signal. Enhanced images and a history of urethral bulking may spare the patient additional expense and exposure to other modalities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.