
Abstract
The pathophysiology of cording (visible bands of tissue that can form in the ipsilateral axilla and arm following breast cancer surgery) remains equivocal. Cording can be a painful and functionally limiting condition. Our aim was to assess the role of duplex ultrasonographic imaging as a diagnostic tool for assessment of this condition. We evaluated five women who had undergone surgery for unilateral breast cancer. Cording was identified by self-report and confirmed by physical examination. Duplex ultrasonography was performed within one week of the clinical diagnosis of cording. Duplex ultrasonography failed to identify the cording structures and does not appear to be a useful diagnostic tool for determining the pathophysiology of cording following treatment for breast cancer. Research focusing on intervention strategies to facilitate the clinical resolution of cording following breast cancer surgery is needed.
Introduction
The formation of visible, palpable bands of tissue in the axillary region following treatment for breast cancer was first described as axillary web syndrome by Moskovitz et al. in 2001 1 (Figure 1). These structures may extend from the axilla into the brachium, cross the antecubital fossa, and sometimes even extend into the volar aspect of the forearm and thumb.1,2 This clinical presentation is also often referred to as cording.2–4 The incidence of cording following breast cancer treatment has been cited to range from 20% to72%1,5,6 and has been reported to cause upper extremity pain as well as functional limitations.1,3–8 Axillary lymph node dissection is consistently cited as the most significant risk factor for the development of cording after breast cancer surgery.1,3–6

Photograph demonstrating axillary cording in the right axilla of a woman who had an axillary dissection for breast cancer.
Despite the relatively high incidence and functional limitations that accompany this condition, the pathophysiology of cording is not well understood. It has been referred to as a variation of Mondor’s disease, which is thrombophlebitis of subcutaneous veins caused by trauma, such as surgery.1,9 In Moskovitz’s report, axillary webs from four patients were biopsied to determine the pathophysiology of the cording tissue. The results revealed dilated, thrombosed lymphatics and/or thrombosed superficial veins, leading the authors to conclude that the etiology was of “lymphovenous” origin. 1 In 2009, Leduc et al. 2 reported on the clinical findings of 15 women who had been surgically treated for breast cancer. Measurements of the palpable cord were performed to determine size and location, with the authors reporting that the cords averaged 44% of the length of the limb. Given the anatomical course of the cords that was documented, the authors also concluded that cording was likely of lymphatic origin. 2 A report by Rashtack et al. 10 in 2012 showed that histologic examination of a “band” thought to be cording demonstrated a structure positive for lymphatic endothelium.
We have previously reported on a cohort of 308 breast cancer patients evaluated for cording, with a cumulative incidence of 36.2% at 24 months postsurgery. 6 The median time to first development of cording was 15.8 months (range, 4.2–38.9). Axillary lymph node dissection and younger age at the time of breast cancer diagnosis were significantly associated with the risk of developing cording. Other clinicopathological factors were evaluated and found not to be associated. These data emphasize that cording following breast cancer treatment is common and may occur after the early postoperative period. Our findings also demonstrated that cording has a significant impact on functional reaching activities. Given the invasive nature of surgical biopsy, we sought to evaluate the utility of duplex ultrasonographic imaging for assessing the pathophysiology of cording in a small cohort of patients treated for breast cancer.
Methods
Study Design and Patients
The cohort for this pilot study was recruited from our lymphedema screening program. In 2009, with Institutional Review Board (IRB) approval, we initiated a large, prospective lymphedema screening protocol. All women undergoing treatment for breast cancer at our institution were prospectively screened for changes in arm volume, function, symptoms, and quality of life (Clinicaltrials.gov identification number NCT01521741). Bilateral arm volume measurements were obtained preoperatively and every three to eight months postoperatively using the Perometer (Pero-System GmbH, Wuppertal, Germany), a valid and reliable instrument that uses infrared light to measure arm volume changes.11,12
To evaluate the efficacy of noninvasive ultrasonographic imaging in determining the pathophysiology of cording, an ancillary protocol received IRB approval in 2010. This ancillary study used the previously described longitudinal screening protocol to identify eligible participants for the imaging study (Clinicaltrials.gov identification number NCT01427166).
Identification of Cording
Cording was determined by self-report on the Lymph-edema Evaluation Following Treatment for Breast Cancer (LEFT-BC) questionnaire during study visits for lymphedema screening. The LEFT-BC is a quality-of-life and symptom assessment questionnaire. The questionnaire stated, “As your body heals following treatment for breast cancer, sometimes bands of tissue can form in your armpit or down your arm that look like strings or thin ropes. This is called cording.” A photograph of cording was included on the questionnaire to assist patients in identifying the condition. Patients were asked to indicate if during the past month, they “saw or felt a thin cord or string in any of the following areas: in your armpit that extends into the inside of your upper arm, across the inside of your elbow, along your forearm and wrist, under your breast extending toward your abdomen or none of the above.” Patients were classified as having cording if they responded “yes” to any of the above locations.
Validation of Self-report for Cording Assessment
Trained research coordinators were notified electronically when a patient indicated “yes” to having cording in the LEFT-BC questionnaire. A designated nurse practitioner in the breast center then performed a clinical examination of the upper limb and axilla to confirm the presence of cording. If cording was confirmed by clinical examination, the patient was offered enrollment in the imaging trial. Once written consent was obtained, the patient was scheduled for an appointment in the Massachusetts General Hospital imaging laboratory within seven days following the clinical examination confirming the presence of cording.
Upper Extremity Exercises
Participants were provided a cording educational sheet that included instructions for applying warm compresses to the cord along with a detailed instructional guide to a series of upper extremity exercises. The intent was to help reduce symptoms of pain and stiffness associated with the presence of cording. Patients were asked to keep a study journal of interventions used to help improve their symptoms.
Duplex Ultrasonographic Imaging
Duplex ultrasonography was performed to identify characteristics specific for the presence of a cord. Study subjects were evaluated with either a GE LOGIQ-9 (GE Healthcare Ultrasound, Milwaukee, WI) or a Philips iU22 (Philips Ultrasound, Bothel, WA) using a 9-MHz multifrequency linear probe and the extremity venous examination instrument presets. 13 This probe was the highest frequency probe available in the imaging laboratory at the time of this investigation. (Our review of the literature did not disclose any other investigation that imaged the cord with higher frequency transducers.) All ultrasonographic examinations were performed following a standard imaging protocol, unique to this study, specifically designed to image for cording. Other advanced imaging features such as harmonic imaging or compound scanning were used as appropriate. For the examination, the patient was placed in a supine position with the upper extremity abducted to 90° and the elbow extended.
All the examinations were performed by the same registered diagnostic medical sonographer (RDMS)/registered vascular technologist (RVT) in an accredited peripheral vascular diagnostic laboratory (Intersocietal Accreditation Commission–Vascular Testing, Ellicott City, MD, www.iac.org). With the patient in the position as described above, the RDMS/RVT identified and confirmed the cord by visual inspection and palpable examination. The transducer was placed on the region of the cord that was visible and palpable, and the cord was evaluated over its entire extent from the axilla to antecubital fossa, with a focus on the palpable cord. 14 Using this target area, imaging was done in both cross-sectional and sagittal scanning planes. Because dense/firm structures are often more highly reflective on ultrasound and appear as brighter echoes than soft tissues in the same region, 15 imaging was concentrated on reflective areas superficial to muscle groups in the arm and in the region where the cord was palpated on physical examination. Optimizing ultrasound settings using high-pulse repetition frequency, focal zone placement in the region of the cord, and the shallowest depth of view possible, all visible structures that were in the region of the palpable cord were evaluated. A continuous, linear echogenic structure in an orienta-tion similar to that of the fascia in muscle groups was considered to represent the cord. Direct measurements of the presumed cord, including area and diameter, were obtained (Figure 2). For comparison and for quality assurance reasons, an ultrasonographic examination in the unaffected arm was done to determine whether the identified structure was the cord and not another normal, dense tissue found in this region. When a soft-tissue structure (not consistent with muscle, nerve sheath, tendon, or vein) was discernible in the region of the cord, the technologist confirmed that the course of that structure could be followed along the path of the palpable cord. Evaluation was then performed in transverse and longitudinal views to establish a set of descriptive terms and measurements to define this structure. The ultrasonographic examinations were independently reviewed by a second technologist for quality assurance, and all of the findings were interpreted by a physician on staff at our institution who is a vascular medicine specialist. Both upper extremities were imaged; the limb without the cord was studied to serve as the control.

Gray-scale image of a cord that was present in a 51-year-old woman who underwent a mastectomy with an axillary lymph node dissection. This imaging examination took place 16 months after her surgery date.
Clinicopathologic Characteristics
Patient demographics and information regarding their breast cancer treatment such as surgical procedure, adjuvant treatment, and tumor size were collected via medical record review (Table 1). Cording has been identified as an independent risk factor for arm volume changes of >5%, so arm volume was documented as well. 6
Clinical and Pathologic Characteristics for the Five Study Participants.
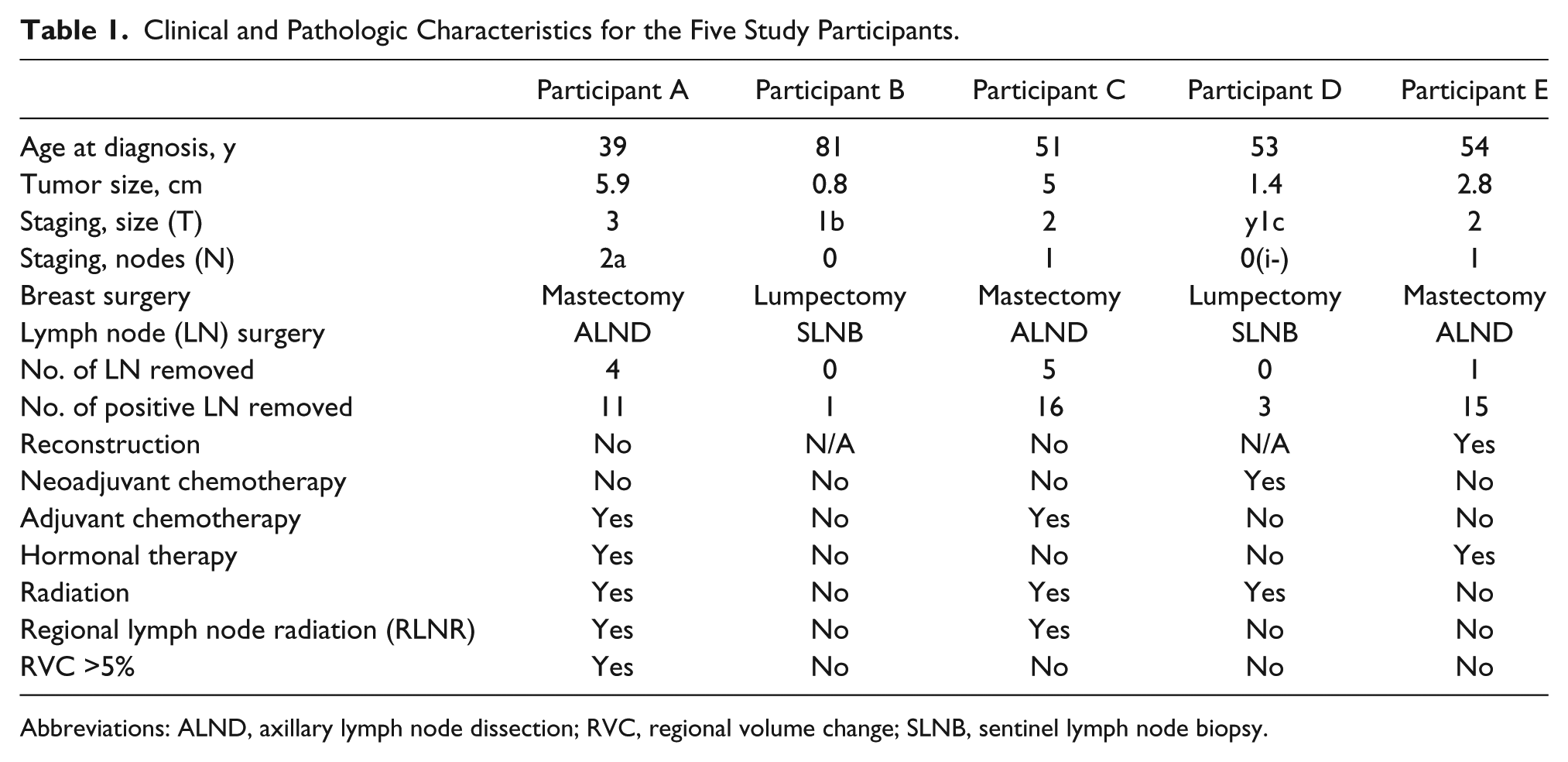
Abbreviations: ALND, axillary lymph node dissection; RVC, regional volume change; SLNB, sentinel lymph node biopsy.
Results
This pilot study permitted enrollment of 15 subjects. Because of the investigational nature of the use of sonographic imaging in this trial, it was determined that after the first initial patients were enrolled, the study team would meet to review the images and determine the efficacy of the imaging studies in meeting the study aims. This preliminary review of the imaging examination findings was part of the original IRB approved protocol for this study. The research team agreed that the target enrollment of 15 patients would be pursued only if early findings yielded useful data at determining the pathophysiology of cording. The research team met after the first five participants had been imaged and the images had been reviewed by the radiologist. The team was in agreement that no more subjects should be enrolled as the results of the first five patients did not provide useful data to determine the pathophysiology of cording.
All five participants were female, with a mean age of 56.2 years (range, 40–81; median, 53.01). They are referred to as participants A, B, C, D, and E (Table 1). The mean time from surgery to onset of cording was 8.15 months (range, 0.87–19.9; median, 3.1). Two participants had undergone lumpectomy and three underwent mastectomy. One of the three mastectomy patients underwent reconstruction, which consisted of a tissue expander. Three of the five women underwent axillary lymph node dissection, and two had sentinel lymph node biopsy. Three of the five women had adjuvant radiation.
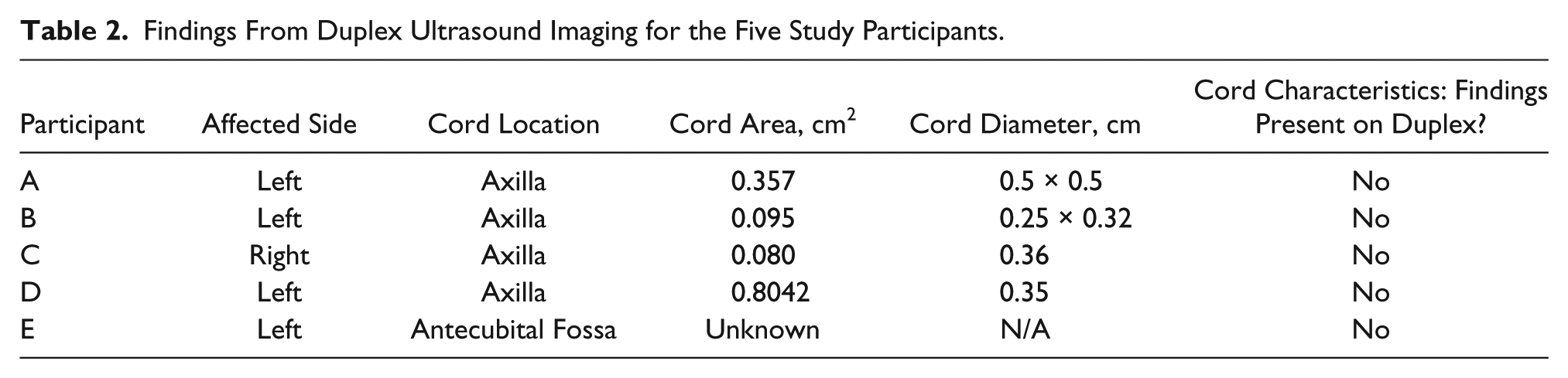
The findings of the duplex imaging examinations are summarized in Table 2. Four subjects demonstrated what was thought to be a cord on duplex imaging. The identified structures were linear and continuous, and they extended into the biceps muscle. The presumed cord had a “honeycombed” appearance in transverse view and a striated/linear appearance in longitudinal view (Figures 2 and 3). Despite other imaging techniques such as computed tomography, honeycomb-like structures have not been previously described as findings in duplex ultrasonographic studies. 16 The presence of fluid in the interstitial spaces on ultrasonographic evaluation is typically a marker for evidence of lymphedema. 17 Even though participant C had only one visible and palpable cord on clinical examination, ultrasonographic imaging showed honeycombed-type structures (unrelated to tendons, nerve sheaths, muscle groups, fascia, or veins) in both arms in the same regions of the bicep. On clinical examination, participant E had a visible and palpable cord on the ipsilateral side of her surgery yet had no discernible ultrasonographic findings on the affected or the unaffected arm.
Findings From Duplex Ultrasound Imaging for the Five Study Participants.
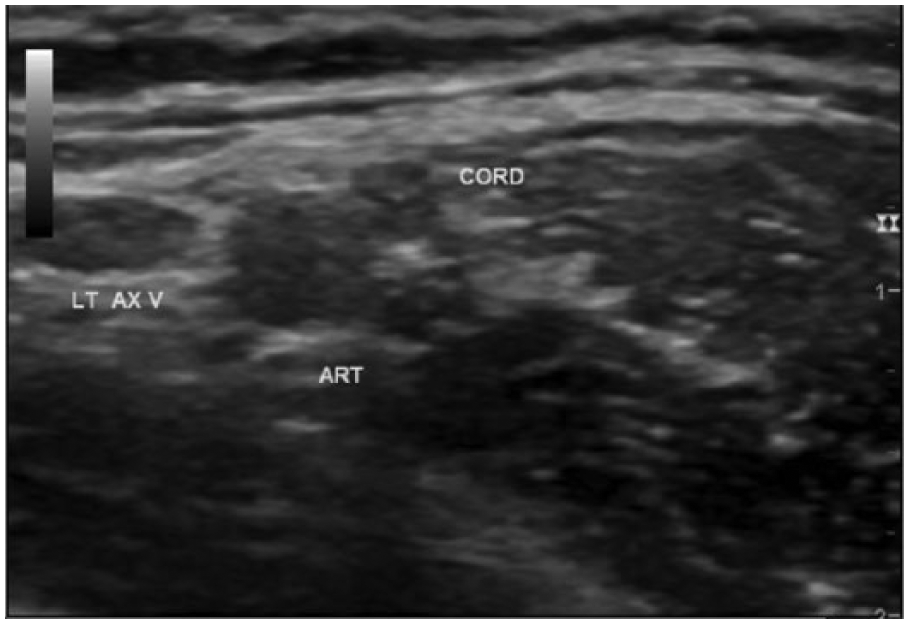
Gray-scale image of a cord that was present in a 53-year-old woman who underwent a lumpectomy with a sentinel lymph node biopsy. This imaging examination took place 1 month after her surgery date. LT AX V, left axillary vein; ART, artery.
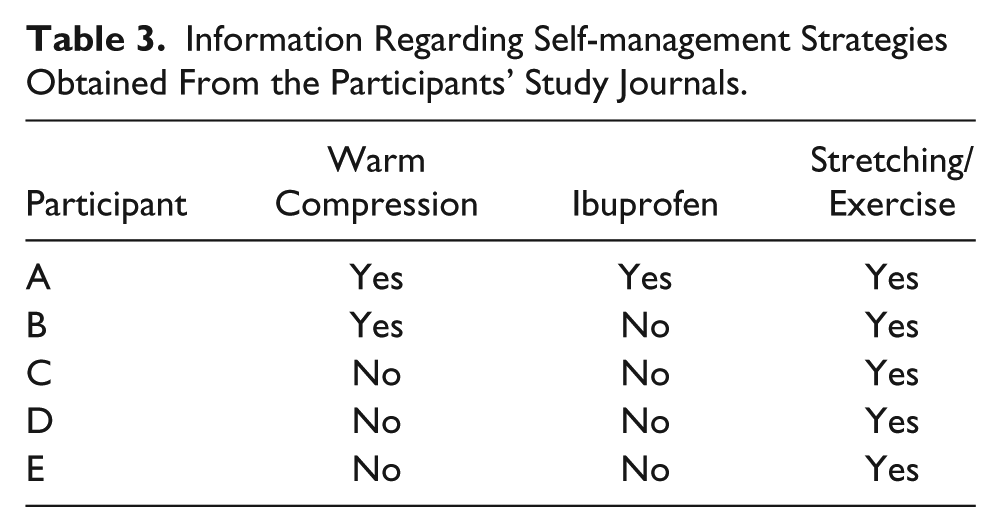
A review of study journals completed by participants in the study showed that all five participants performed stretching exercises provided to them per protocol in an attempt to improve the use of their arm for functional activities requiring the ability to reach laterally or overhead. Some used warm compresses or took ibuprofen to help resolve the cord and associated symptoms, as has been recommended in the literature 18 (Table 3).
Information Regarding Self-management Strategies Obtained From the Participants’ Study Journals.
Discussion
Ultrasonographic imaging is commonly used for evaluation of soft-tissue structures such as lymph nodes, tendons, fascia, and muscles as well as in the identification of seromas, abscesses, and fluid collections. 19 However, to date, no validation is available in the literature to support the utility of duplex ultrasonography for the purpose of identifying lymphatic channels. The results of this pilot trial are consistent with that diagnostic limitation when evaluating cording. Although the patient and technologist could visualize and palpate a cord and placed the transducer directly over that site, the technologist and vascular physician who interpreted the findings found no consistent or reliable indicator to determine the absolute presence or absence of a cord on the ultrasonographic images. One possibility for this may be a limitation of the sensitivity of the 9-MHz transducer used in this study; for such superficial structures, a much higher frequency transducer, for example 12 to 15 MHz, might provide more definitive results.
The rationale for investigating the pathophysiology of cording is twofold. One, it would enhance patient education, as providers could give patients a clear explanation of this painful and functionally limiting problem. Second, understanding pathophysiology could clarify whether all cording structures are of similar etiology and would provide data that could be important in determining strategies for intervention. Given the results of this pilot trial, it appears that biopsy seems to be the only definitive procedure to determine the pathophysiology of cording.1,5,10 However, given the invasive nature of this procedure, it is not a diagnostic tool that we endorse for patients with cording.
The question of how to clinically manage axillary web syndrome/cording remains unresolved. Several reports in the literature suggest that axillary web/cording is a self-limiting problem that occurs in the first three months following surgery and typically resolves spontaneously during that time period.1,2,4,5 Our data demonstrate that cording can continue to be present for the first time many months after surgery, with new cases developing as late as 24 months postoperatively. 6 Other reports in the literature suggest that there are effective interventions that facilitate the resolution of cording; however, these are mainly case studies and a single retrospective review.18,20–23 Randomized, controlled clinical trials are needed to determine if there are effective intervention strategies that are appropriate for this condition.
Conclusion
In conclusion, the noninvasive duplex ultrasonographic imaging used in this pilot study was not able to distinguish characteristics unique from other soft-tissue structures for palpable, visible cords. In addition, use of ultrasonographic imaging did not provide useful information on the pathophysiology of cording. The results of this pilot study demonstrate that other methods of imaging should be investigated to determine a reliable diagnostic tool to differentiate lymphatic channel inflammation from a cord in patients with palpable cords on clinical examination. Given that biopsy is an invasive method of determining pathophysiology, we suggest that in addition to noninvasive imaging, future research should be directed toward generating level 1 evidence to determine if all cording is self-limiting or if there are clinical presentations of axillary web syndrome/cording in which intervention with physical or occupational therapy may facilitate resolution. The standard of care for managing cording has yet to be well supported by evidence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by award R01-CA139118 (NIH) and award P50-CA089393 (AVON/Spore PFP Award) from the National Cancer Institute and the Adele McKinnon Research Fund for Breast Cancer-Related Lymphedema. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health.