
Abstract
Diagnostic imaging has proven to be a beneficial tool in the screening, diagnosis, and prognosis of breast cancer. Most cancers are found early with breast screening methods, such as mammography. In some instances, breast cancer will go unidentified or untreated up to the point that the cancer becomes more advanced. This case study investigates a form of breast cancer that was diagnosed within a month after the patient’s first meeting with her physician. The breast cancer was examined with x-ray, computed tomography, and sonography. The role of sonography is discussed in detail with the aim of illustrating the usefulness of this technology in identifying cancerous breast tissue.
Inflammatory breast cancer (IBC) is an aggressive form of breast cancer accounting for 2.5% of all breast cancer cases.1,2 It is characterized by rapid progression, local and distant metastases, younger age of onset, and lower overall survival compared with other breast cancers. 2 Because of the rapid progression of IBC, accurate diagnosis is critically important. Magnetic resonance imaging (MRI), positron emission tomography (PET), computed tomography (CT), mammography, and sonography are diagnostic imaging examinations that can be used to evaluate the status of IBC. One study aimed to compare the previously mentioned imaging studies in their ability to examine IBC; it was found that sonography was able to identify an area of focal linear infiltration in the absence of a discrete mass and yielded a diagnosis of cancer. 3
This particular case study presents a patient with inflammatory breast cancer and the imaging tests that were used to evaluate her condition. CT and sonography played a prominent role in the evaluation of the cancer, whereas the role of sonography specifically was deemed clinically significant because of its posttreatment application.
Case Report
A woman in her early 60s was diagnosed with advanced stage inflammatory breast cancer in the left breast. The cancer was categorized as T4B, with “T4” referring to the large size of the tumor and the extent it had grown into the chest wall and/or skin and “B” referring to the ulcerative nature of the mass. 4 Initially, the patient had noticed what she thought was a spider bite on her left breast, and she left this untreated until the “spider bite” developed a significant ulceration. At her initial evaluation, the patient stated she had not had a mammogram in more than two years. Because of the nature of the lesion, a biopsy was performed almost immediately, and the results showed the breast to have ulcerated skin with poorly differentiated carcinoma.
The first imaging tests ordered to evaluate the cancer included an x-ray and a chest CT with contrast. The x-ray revealed a prevalent necrotic area in the left breast (Figure 1), whereas the CT documented several masses. The first mass, identified as the primary tumor in the left breast, measured 8.9 cm (Figure 2). The mass had a cavitary component against the skin’s surface and appeared to invade the surrounding area. On the surface, the cancer was associated with skin thickening and enhancement. The mass was described as having probable central ulceration, and the diagnosis of exclusion was necrotic erosive primary breast carcinoma.
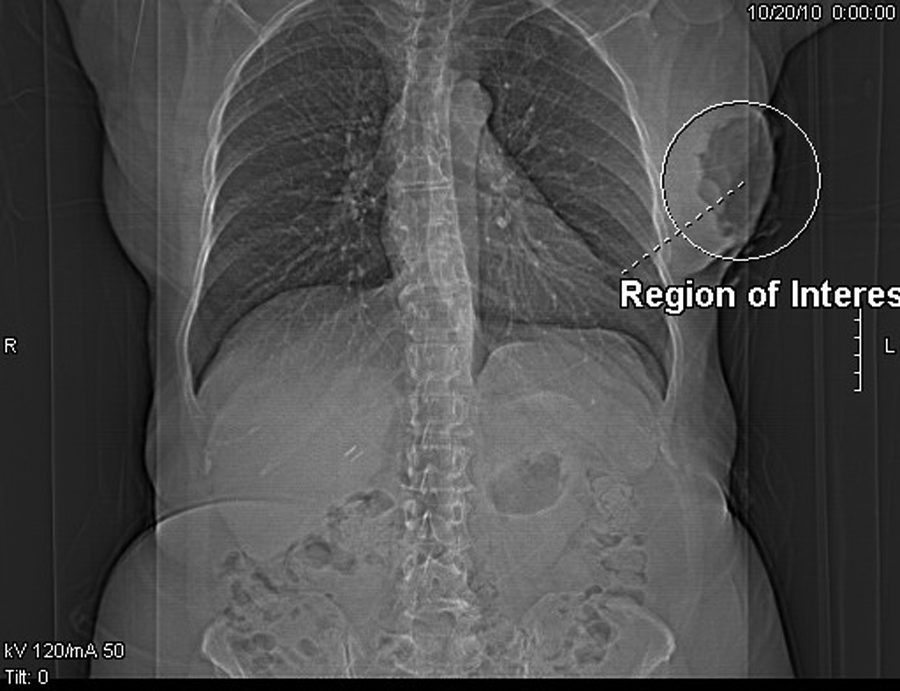
An x-ray of the primary location of the cancer in the left breast. The region of interest (right) notes the target area.

A computed tomography image demonstrating the large mass in the left breast (A); the mass measured 8.9 cm (B). The ulcerative characteristic of this mass is noticed anteriorly.
A second mass shown on CT in the supraclavicular area measured 4.5 cm (Figure 3). This mass was suspicious for direct bony and muscular invasion and also displayed central necrosis and irregularity.
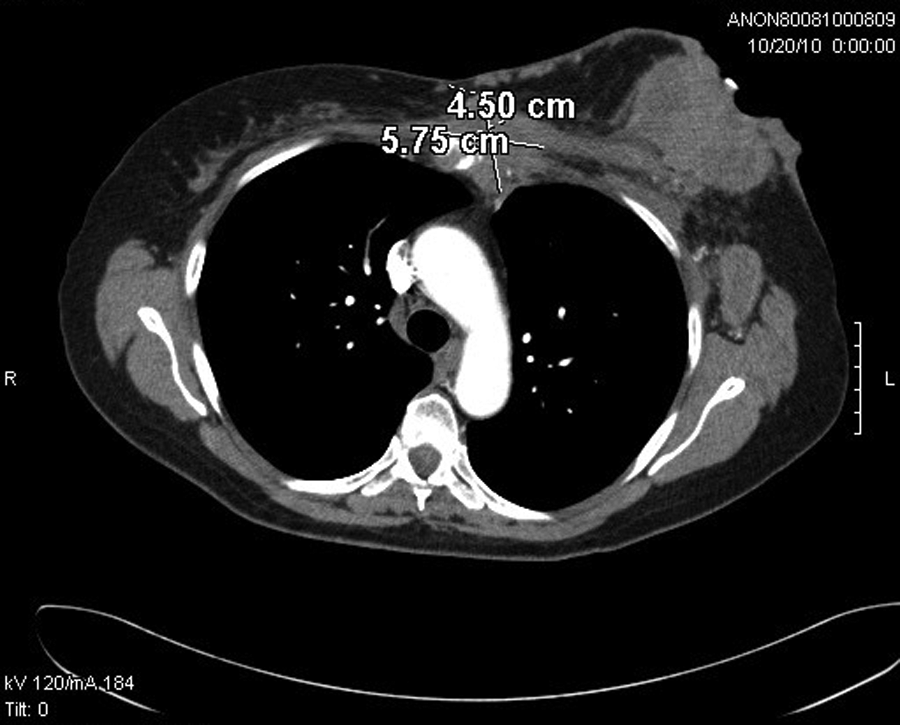
A computed tomography image demonstrating the 4.5-cm supraclavicular mass. Notice the invasion of this mass into the anterior chest wall and mediastinum.
The final masses were identified as massive left axillary adenopathies, the largest measuring 5.85 cm and another measuring 4.3 cm (Figure 4). All the findings from the CT suggested the cancer to be advanced with metastatic disease.
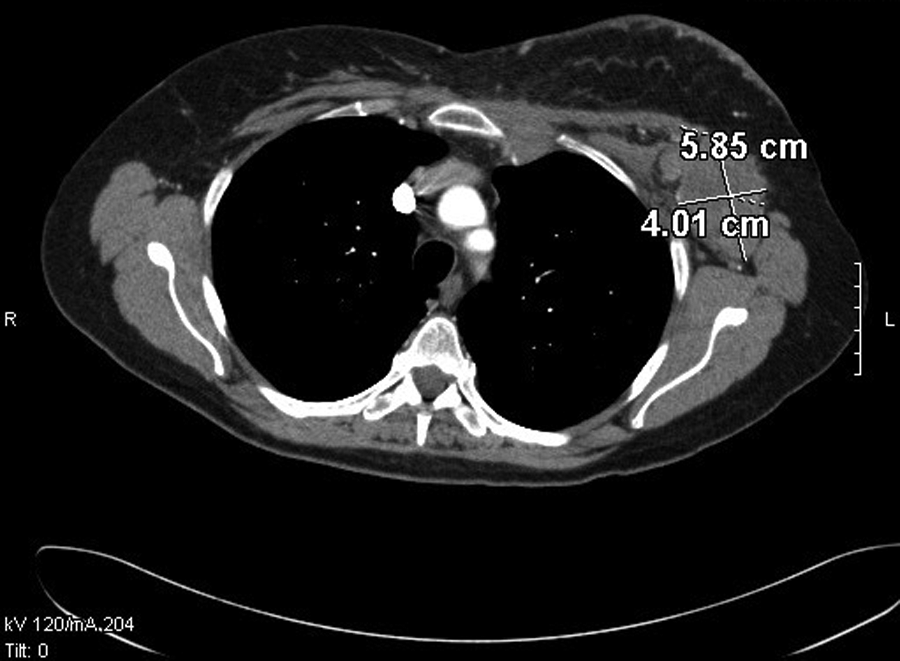
A computed tomography image of the 5.85-cm mass in the axilla region.
Because of the advanced nature of the patient’s cancer, chemotherapy (in the form of Taxotere) was begun almost immediately following her initial examination. A chest and abdomen CT with contrast and an x-ray were performed after a few rounds of chemotherapy had taken place. These scans demonstrated no metastases to the lungs, liver, abdomen, or bone. The patient seemed to be responding well to the chemotherapy.
Additional imaging performed after the patient underwent more chemotherapy treatment included CT of the chest and abdomen, intended for restaging the cancer, and a sonogram of the left breast to determine residuals of the tumor and serve as a baseline examination for future studies. The chest CT revealed bilateral pleural effusions (Figure 5), which were felt most likely to be secondary to the Taxotere chemotherapy versus metastatic disease. Sonography was done using a GE Logiq E9 (GE Healthcare, Waukesha, Wisconsin) with a linear matrix array probe (ML6-15). On the sonogram, the left breast mass could not be visualized adequately due to the ulceration of the breast. A large, heterogeneous mass was identified in the left upper outer region and measured about 5 cm (Figure 6). A second large mass was identified in the lower inner and outer portions of the left breast and appeared to be too large to fully display on the sonogram (Figure 7). A 3-cm hypoechoic region was identified in the axilla (Figure 8). During the breast sonogram, color Doppler imaging showed significant blood flow to the area of interest (Figure 9). The results of the sonogram were classified as BI-RADS category 6—known cancer.
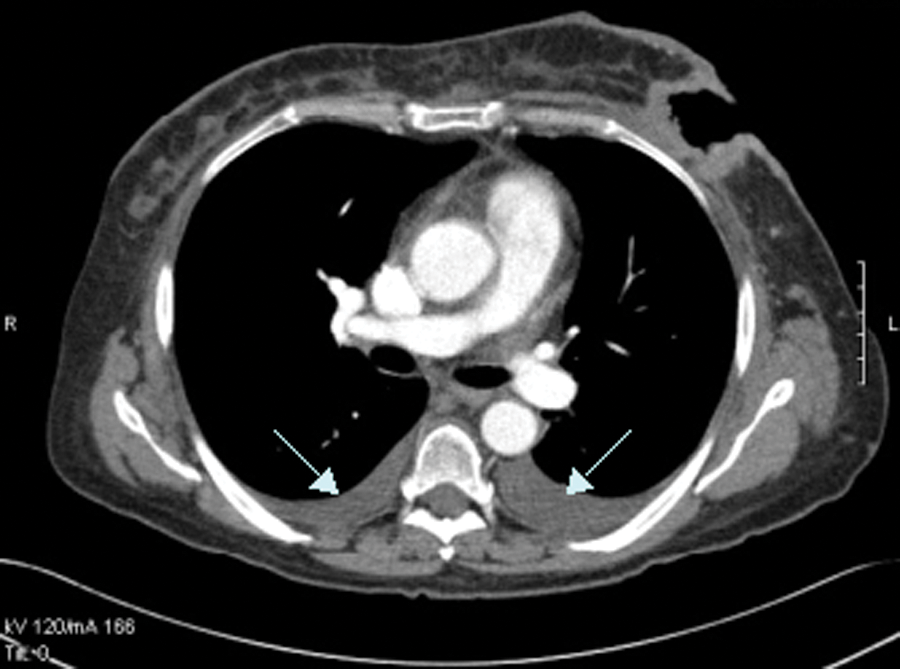
A computed tomography image showing the bilateral pleural effusions (arrows).

A sonogram showing longitudinal (A) and transverse (B) views of the primary breast mass in the upper outer portion of the left breast.

A sonogram showing longitudinal (A) and transverse (B) views of the mass located in the lower inner-outer portion of the left breast.
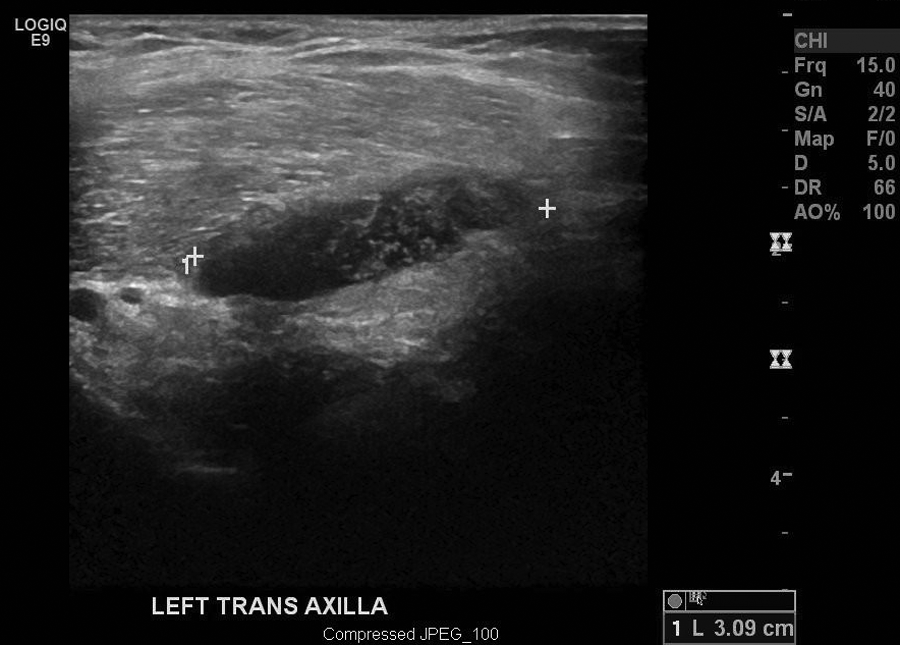
A sonogram showing a transverse image of the 3-cm mass found in the left axillary region.
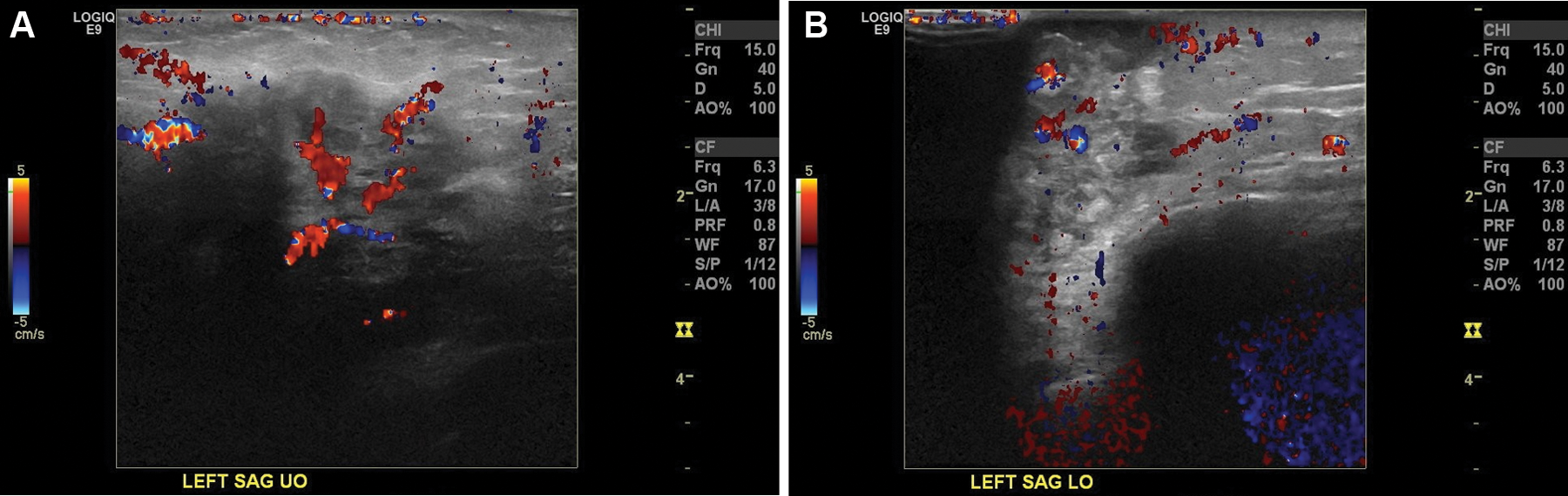
The use of color Doppler on sonographic examination of the masses located in the upper outer region (A) and lower inner-outer portion (B) of the left breast. Both views were obtained longitudinally.
Discussion
Few aspects of the diagnosis of breast disease are managed by symptoms or hematological data; instead, images tell the story. 5 This is why diagnostic imaging is important. If a patient initially presents with a more advanced form of breast cancer, diagnostic imaging will still play a large role in the diagnosis and treatment of the disease. Mammography, sonography, MRI, CT, and PET are all used to examine the severity and extent of breast cancer.
When evaluating all the imaging procedures used on this breast cancer patient, it may seem odd that a mammogram was never performed on her upon the realization that she had breast cancer. In this case, the use of mammography would not have been beneficial for three reasons: (1) the cancer was already so advanced that mammography would not have diagnosed the condition any more effectively, (2) any image obtained from a mammogram would likely be unclear and nondiagnostic due to the ulcerative characteristics of the breast tissue, and (3) the patient would have experienced severe pain during the test given the physical presentation of her breast.
It is widely understood that the use of sonography in evaluating breast cancer can provide valuable information about the nature and extent of a solid mass or lesion within the breast tissue. 5 Although sonography is not generally an effective method for diagnosis of breast cancer when used independently of other diagnostic examinations, certain characteristics present in malignant masses are apparent on sonograms. In this case, the patient’s sonogram showed that the large breast masses measured taller than wide, appeared very hypoechoic, and demonstrated posterior shadowing, all characteristic of malignancy.
It would have been educational to sonographically document the cancer throughout the different stages of treatment (which was done with CT) for comparative purposes. But in this case, sonography was used later on to assess the response of the cancer to chemotherapy treatments. A recent article has noted that sonography is extremely useful in evaluating the response to induction chemotherapy of axillary nodes, with possible impact on timing of local therapy. 2
In this particular instance of IBC, it seemed the most valuable diagnostic imaging test was CT. The cancer and metastatic disease appeared distinctly on the chest CT images throughout the course of the patient’s treatment. Staging, follow-up, and monitoring morphological changes of the tumor in response to treatment can all be evaluated by CT. 6 The patient received CT examinations before and after chemotherapy, and the difference in the size was quite clear.
Conclusion
Multiple imaging studies are needed to fully understand an advanced stage of inflammatory breast cancer; typically, no single study can stand on its own. In specifically addressing the use of sonography in evaluating advanced breast disease, the technology is gaining recognition and respect in its diagnostic application. Sonography is able to characterize some biological aspects of the cancer because the imaging depends on not only morphology and structure but also vascularization and perilesional reaction. 6 The assessment of advanced breast cancer by use of sonography and other imaging studies has proven to be beneficial in the diagnosis, staging, and prognosis of the disease.
Footnotes
Acknowledgements
The author thanks Darla McQuitty, Emily Melville, Breanna Wells, Andrea Frazier, and Shawnda Conner for their assistance in preparing and presenting this case study.
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author received no financial support for the research, authorship, and/or publication of this article.