
Abstract
Normal physiologic herniation of the fetal bowel is often seen on first trimester sonogram. An omphalocele is an abdominal wall defect that occurs as a result of herniation into the umbilical cord and is often associated with chromosomal anomalies. This case report presents an omphalocele seen in the first trimester and discusses how to differentiate this finding from normal physiologic bowel herniation.
Normal physiologic herniation of the fetal bowel occurs between 8 and 12 weeks gestational age and is a finding often seen on first trimester sonogram.1–3 An omphalocele is an abdominal wall defect containing bowel and/or liver and occurs as a result of herniation into the umbilical cord. This embryologic defect is often associated with chromosomal anomalies.4–9 With careful scanning, the sonographer may be able to differentiate normal physiologic gut herniation from early identification of an omphalocele.1,10 This case report describes a first trimester omphalocele and discusses how to differentiate an omphalocele from normal physiologic gut herniation.
Case Report
A 31-year-old female presented to the ultrasound department for a routine first trimester sonogram. The patient denied any pertinent medical history. Transabdominal sonography, followed by transvaginal sonography, showed a single living intrauterine pregnancy with a gestational age of 10 weeks 3 days. Sonography also showed increased nuchal translucency (4.0 mm), a small volume of ascites, and what appeared to be an omphalocele containing a portion of the liver and measuring approximately 9 mm in size. (Figures 1 and 2) The remainder of the examination was unremarkable. As a result of the sonographic findings the patient terminated the pregnancy, and no follow-up was able to be obtained. It is unknown whether the patient had the products of conception tested for aneuploidy.
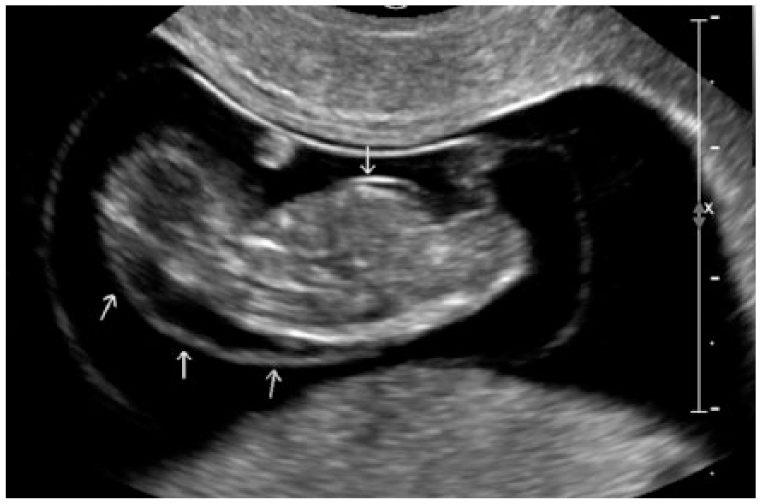
Sagittal gray-scale image of 10-week fetus showing herniation (arrow) and associated increased nuchal lucency (arrows).

Gray-scale image of fetus with measurement of herniation; 9 mm size suggests omphalocele.
Discussion
Normal embryologic maturation of the abdominal wall and bowel occurs during the fourth week of gestational age. This process involves three folds: foregut, midgut, and hindgut. The foregut makes up the esophagus, stomach, duodenum, liver, pancreas, biliary tract, pharynx, and lower respiratory tract. The midgut structures include the small intestine, cecum, appendix, ascending colon, and the proximal portion of the transverse colon. The hindgut includes the distal portions of the alimentary tract and parts of the genitourinary tract. In the early stages the small bowel tends to grow quickly and outpace the capacity of the abdominal cavity, thus protruding into the base of the umbilicus (Figure 3). Abnormalities are frequently seen during this midgut fold formation.1–3 In this stage, the intestines will herniate into the umbilicus, twist 90°, and conclude with a 180° counterclockwise twist before descending back into the abdominal cavity. In some instances, there is incomplete rotation of the bowel, which leads to an omphalocele.

Gray-scale image example of a first trimester fetus showing protrusion of the midgut into the base of the umbilicus.
An omphalocele is an encapsulated abdominal wall defect containing bowel and/or liver and occurs as a result of incomplete rotation of bowel returning into the abdominal cavity (Figure 4). An omphalocele is not typically an isolated finding.7–9 Concomitant with an omphalocele are a plethora of potential abnormalities including congenital heart defects (47%), genitourinary defects (40%), and neural tube defects (39%).6,11 Intrauterine growth restriction has also been found to be associated with an omphalocele. 12 The main chromosomal defects that would be found with an omphalocele are trisomy 13 (Patau syndrome) and trisomy 18 (Edward syndrome). 4 Due to the coexistence of multiple anomalies, a fetus found to have an omphalocele has a high mortality rate.1,2

Diagram showing herniation of the small bowel, with a portion of the liver, into the base of the umbilicus with incomplete rotation of the bowel back into the abdominal cavity, characteristic of an omphalocele.
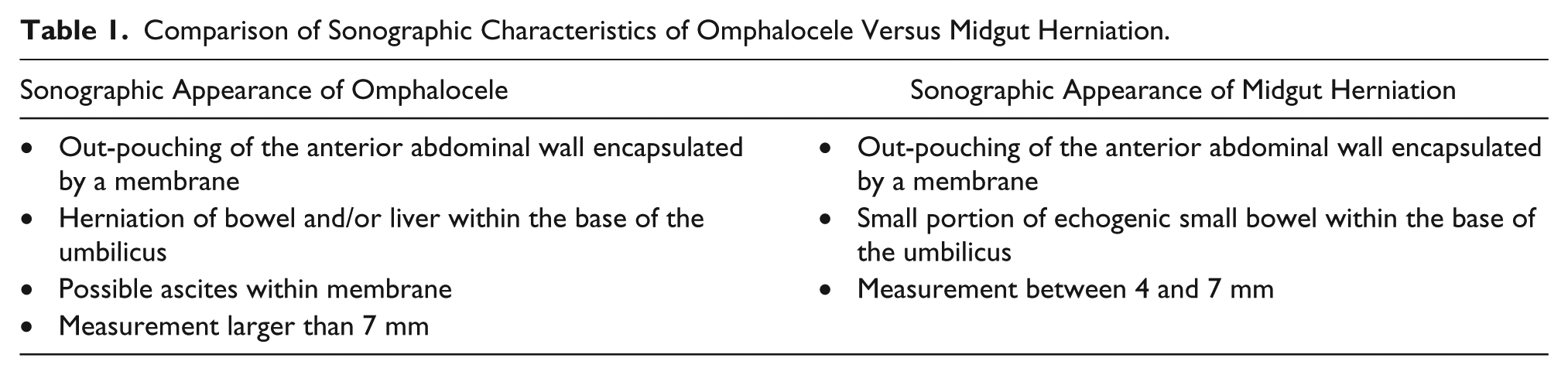
A number of significant features differentiate physiologic midgut herniation from an omphalocele (Table 1): (a) Midgut herniation descends back into the abdominal cavity by 12 weeks gestational age. (b) Midgut herniation will have a heterogeneous appearance within the encapsulated umbilicus, while an omphalocele will tend to have a more homogeneous appearance. (c) Midgut herniation will present as a small spherical shape, while an omphalocele will present with a large circular shape anterior to the abdominal wall. (A physiologic midgut herniation measures between 4 and 7 mm [Figure 5], and an omphalocele measures greater than 7 mm. 10 ) (d) The “tip of the iceberg” sign for an omphalocele is the definite appearance of the liver along with small bowel within the herniation.
Comparison of Sonographic Characteristics of Omphalocele Versus Midgut Herniation.

Gray-scale image example of a first trimester fetus showing the measurement of a normal physiologic midgut herniation.
Sonography can play a significant role in discerning midgut herniation from an omphalocele. Careful first trimester scanning of the anterior abdominal wall is crucial. It is important to determine the gestational age of the fetus being scanned and determine whether a physiologic midgut herniation should be present. The sonographer must examine the echogenicity of the herniation at the base of the umbilicus and make a determination as to heterogeneity or homogeneity. If the sonographer concludes that the herniation is too large to be considered a physiologic midgut herniation, measurements must be taken at the base of the umbilical herniation. Since an omphalocele is not usually an isolated finding, a survey appropriate to gestational age should be used to further locate other potential abnormalities, with a follow-up anatomical survey when more anatomy can be identified. An omphalocele is often found with an increased nuchal translucency (>3 mm) on the back of the fetal neck (Figure 1). Another common finding is fetal intrauterine growth restriction (fetal weight <10th percentile). 12
Upon diagnosis of an omphalocele via sonography, it is usually recommended that the mother receive a chromosomal screening analysis. The chromosomal analysis can be accomplished by either a blood test, such as cell-free DNA, or an amniocentesis.1,5 Amniocentesis will provide a definitive diagnosis of a wide variety of congenital conditions, including trisomy 13 and trisomy 18.
The prognosis of a fetus with an omphalocele is not always lethal. More often than not it ends in a fetal demise because of the associated chromosomal abnormalities.4,13 However, there are occurrences where a fetus progresses to full-term birth and is delivered. Upon delivery, surgery is performed on the fetus’s abdominal wall to correct the omphalocele and place the intestines back into the abdominal cavity.3,14 Studies have been performed to determine whether postbirth repair is an option. Montero et al 15 suggested using the omphalocele diameter in comparison to the abdominal circumference, femur length, and head circumference to evaluate whether the omphalocele is compatible for repair. With a ratio of 0.21 or greater, it is considered a “giant” omphalocele, which results in a poor outcome.
Conclusion
Midgut herniation is a normal physiologic occurrence during fetal development. However, complications can arise during this phase of fetal development, including an omphalocele. An omphalocele is an abdominal wall defect containing bowel and/or liver as a result of herniation into the umbilical cord. This abnormality is often associated with chromosomal anomalies, most commonly trisomy 13 and trisomy 18. With attentive and thorough scanning, an omphalocele can be detected and differentiated from normal physiologic herniation, which has a significant effect on the outcome in clinical decision making.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.