
Abstract
This article focuses on the sonographic examination technique for evaluation of intracranial translucencies during the first trimester scan. Appropriate knowledge of the sonographic landmarks is the most important factor for evaluating normal as well as abnormal brain structure, and this examination may enable detection of open spina bifida at an early stage of fetal development.
Keywords
Introduction
Screening at 11 to 13 weeks’ gestation is now performed not only to measure nuchal translucency (NT) but also to detect severe malformations and identify pregnancies at high risk for adverse fetal and maternal outcome. 1 There is a growing body of evidence that with a thorough knowledge of normal and abnormal anatomic features and with appropriate sonographic technique, open spina bifida (OSB) may be detected early in pregnancy. 2 Chaoui et al3,4 were the first to report on the standardized view and feasibility of early detection of OSB by anomaly of the cranial posterior fossa at the time of NT screening.
Sonographic Technique
The examination should be performed with as high an image resolution ultrasound system as possible; for the figures shown in this article, a Voluson E6 (GE Medical Healthcare System, Milwaukee, WI) was used with a transabdominal multifrequency 4- to 8-MHz (R48D) probe. The following sonographic system settings were used: harmonic imaging, high; wide aperture scanning (cross-beam), 1; speckle reduction, 3; dynamic range, 6; contrast, 7; line density, normal; and gray map, 7.
The fetus is scanned in the midsagittal section (Figures 1 and 2), the same plane as required to measure the NT according to the Fetal Medicine Foundation guidelines (www.fetalmedicine.com). The crown rump length (CRL) must be 45 to 84 mm and the image of the fetus should be magnified to occupy at least 75% of the entire image display. For correct NT measurements, the probe must be angled to avoid the zygomatic process, and the maximum “on-to-on” distance must be measured. The first caliper is placed at the level of the internal echogenic line representing the soft nuchal tissues, while the second caliper is placed at the level of the external echogenic line representing the fetal skin. In the midsagittal section, two echogenic lines of the nasal bone are visualized, and this additional sonographic marker can be included in the statistical model to calculate the corrected maternal risk for aneuploidies—namely trisomy 21, trisomy 18, and trisomy 13. The probe is then angled upward to allow evaluation of the occipital brain (Figure 3), while a tilting of the probe allows visualization of the choroid plexuses of the lateral ventricles (the “butterfly sign”).
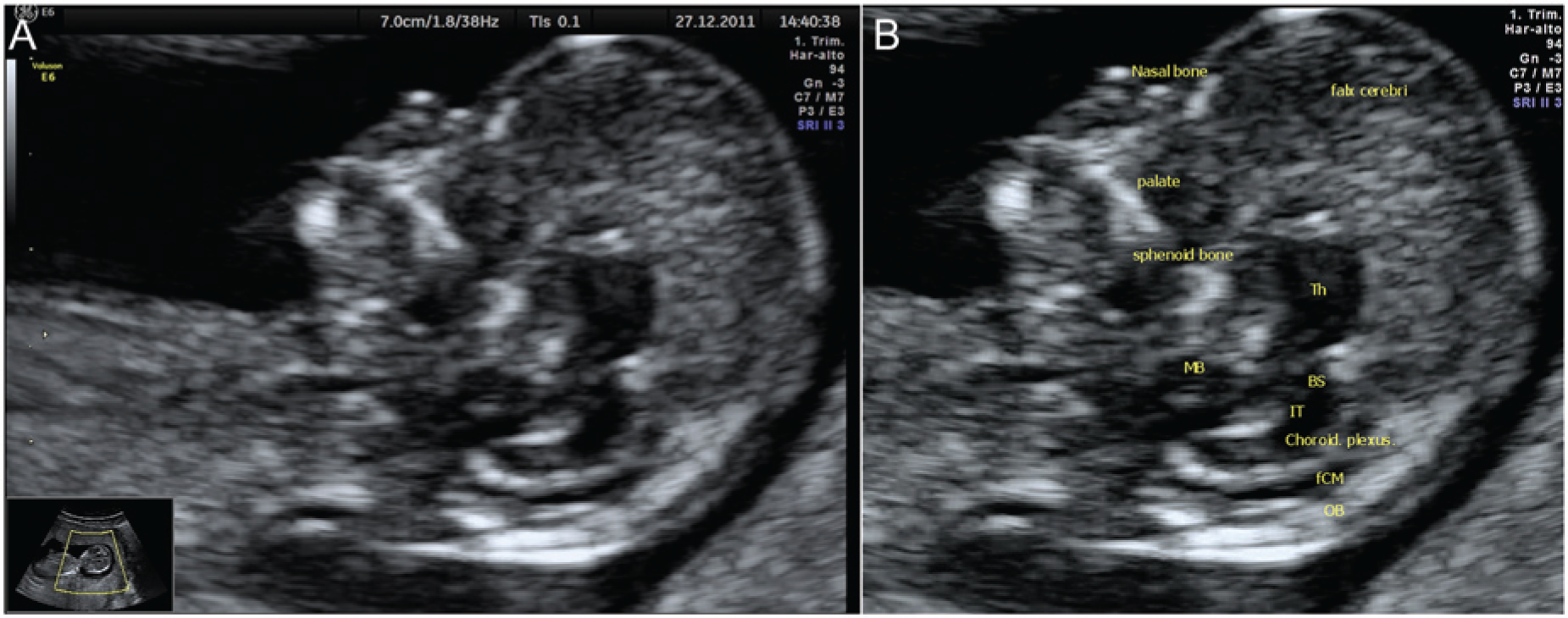
(A) Transabdominal scan performed at 12 weeks gestation in midsagittal plane showing the fetal profile and the intracranial translucencies. (B) Scan parameters as for part A with sonographic anatomic landmarks. BS, brain stem; MB, midbrain; fCM, future cisterna magna; IT, intracranial translucency; OB, occipital bone; Th, thalami.
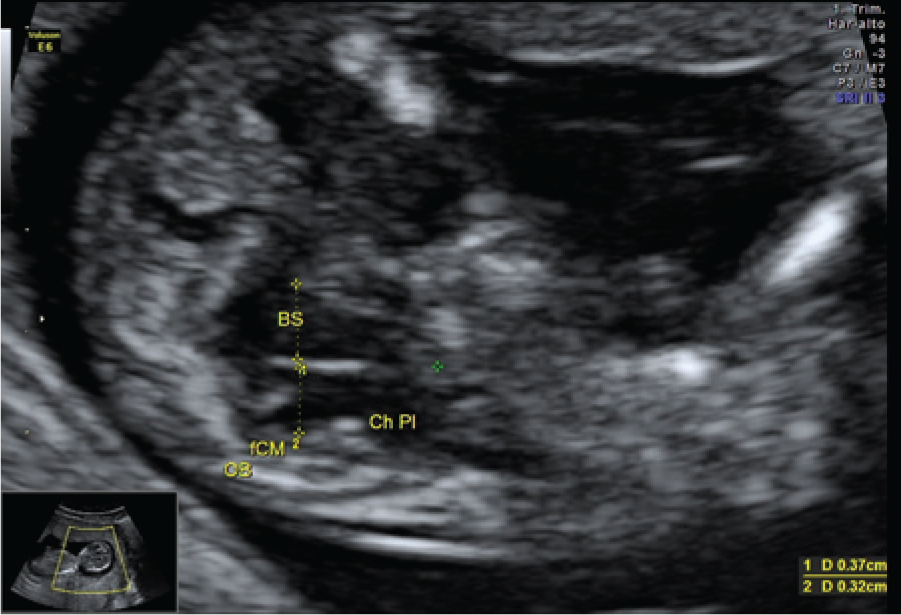
Demonstration of the measurement of the brain stem and the intracranial translucency as well as the brain stem to occipital bone diameter. BS, brain stem; Ch pl, choroid plexus of the fourth ventricle; fCM, future cisterna magna; OB, occipital bone.
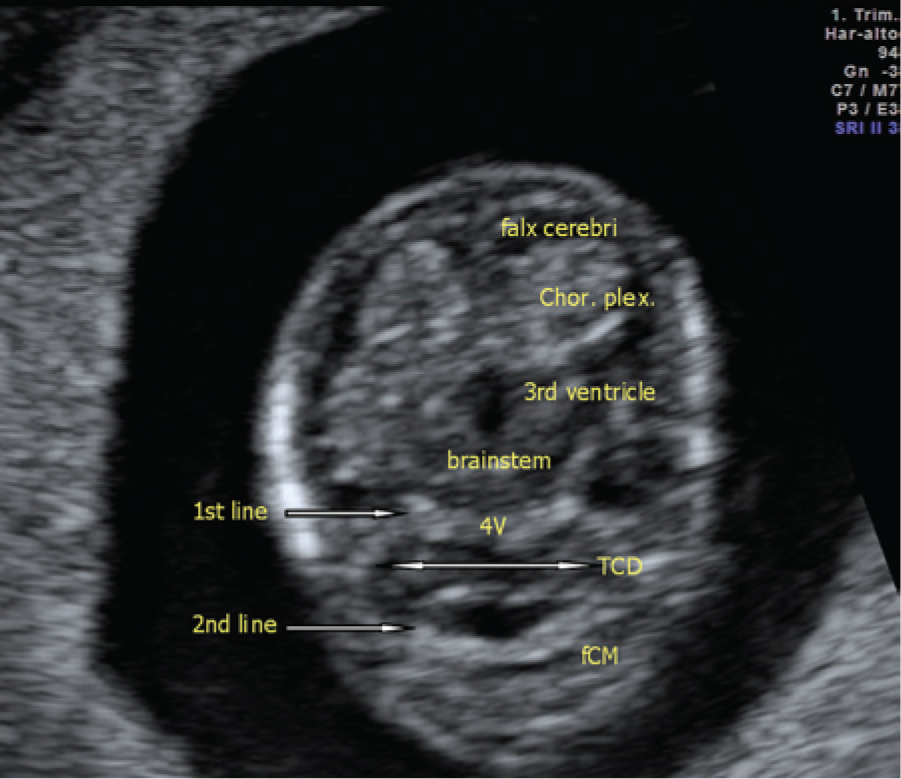
The same fetus as shown in Figure 1 in the transabdominal axial plane. Note the 2 echogenic lines represented by the intracranial translucency (4V, fourth ventricle, first line) cranially and by the future cisterna magna (fCM, second line) caudally. TCD, transcerebellar diameter.
In the midsagittal section in normal fetuses, the future cisterna magna (CM) extends along the entire length of the fourth ventricle and is separated from it by a thin membrane, which in the tilted axial view appeared as a transverse echogenic line. At 11 to 13 weeks, the fourth ventricle appears as a fluid-filled translucent region with 2 echogenic horizontal borders, representing the posterior border of the brain stem (anteriorly) and the echogenic thin choroid plexus of the fourth ventricle (posteriorly). The fluid of the future CM is readily identified between the choroid plexus and the occipital bone. Fetuses with OSB have a posterior and caudal displacement of the fourth ventricle and partial or complete obliteration of the CM. 5
Discussion
Chaoui et al 3 initially examined fetuses at 11 to 13 weeks in the midsagittal view and reported that in 200 normal fetuses the fourth ventricle was always visible, with a mean anteroposterior diameter of 2.0 mm, whereas in 4 fetuses with OSB the fourth ventricle was obliterated through compression by the caudally displaced hindbrain. In a later paper, Chaoui et al 4 described a case series of 6 fetuses with OSB, of whom 2 were detected with trisomy 18 at the routine 11- to 13-week sonographic examination (Figure 4). The intracranial translucency (IT) was obliterated in 2 cases, and in all cases the typical landmarks of a normal posterior brain and normal IT were absent. In all cases, the ratio of brain stem diameter to brain stem–occipital bone (BSOB) distance was increased to ≥1, independent of CRL. Those authors have further demonstrated the feasibility of using the standard midsagittal plane commonly used for NT measurement to assess the IT and the posterior brain and to determine the presence of OSB during NT screening, 6 and they concluded that the midsagittal plane of the fetal face is the standard view and should be used also to visualize the posterior brain region.
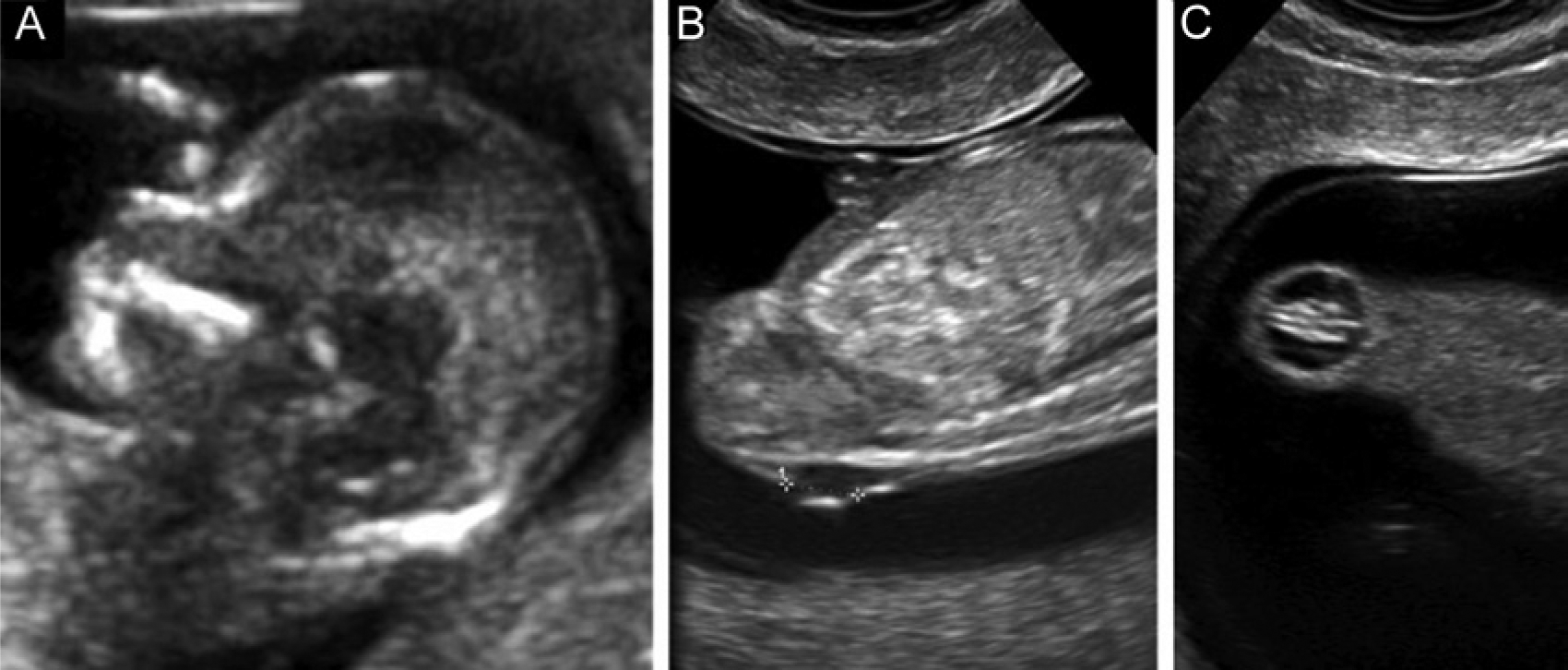
(A) Transabdominal songraphic image of the fetal face showing a mid-sagittal view, with no typical clear intracranial translucency borders identifiable. The brainstem is thickened and the distance from the posterior border of the brainstem to the occipital bone is shorter than the brainstem diameter. (B) Subsequent transvaginal sonographic image of the spine showed a small lumbosacral spina bifida 5 mm in diameter (calipers) and, once the fetus had turned (C), the small myelomeningocele could be visualized in a coronal tangential plane. (Reproduced with permission from Chaoui et al 4 and ISUOG.)
Sonographic study of the posterior brain region can also be achieved using the tilted-axial view. 7 In this plane, the posterior transverse echogenic lines disappear, resulting in the “single-line” sign in cases of OSB. 5 At 11 to 12 weeks, the cerebellum is tiny and is located above and dorsal to the fourth ventricle. 8 The fourth ventricle is delineated by a thin membrane, which can be demonstrated in a tilted axial fronto-occipital plane. Later, union of the cerebellar hemispheres takes place and the upper part of the vermis develops. 9 Lachman et al 10 examined the brain stem diameter and the BSOB distance (the vertical distance between the brain stem anteriorly and the occipital bone posteriorly) using stored images of the midsagittal view of the fetal face at 11.0 to 13.6 weeks from 30 fetuses with OSB and 1000 normal controls. The authors showed that in fetuses with OSB the brain stem diameter was above the 95th percentile of the control group in 29 cases (96.7%), while the BSOB diameter was below the 5th percentile in 26 cases (86.7%) and the brain stem to BSOB ratio was above the 95th percentile in all cases.
Sonographic assessment of IT is a feasible and reliable technique and may be performed at the first-trimester screening scan. The posterior brain area can be visualized with the same standardized midsagittal plane as is used for aneuploidies screening. In cases of suspected abnormality, an axial plane obtained by a transvaginal, anterior transfontanelle approach can be performed together with a targeted examination of the fetal spine. Reference ranges for IT (fourth ventricle), brain stem and BSOB diameters, and the anteroposterior diameter of the future CM and transcerebellar diameter have been constructed according to CRL. Intracranial translucency can be measured manually or by means of semiautomated calculation systems available in most state-of-the-art ultrasound systems. The manual and the semiautomated calculation of IT have been shown to be equally accurate and reproducible.
When the tilted axial plane is used, the anteroposterior diameters of the future CM and fourth ventricle are measured essentially along the suboccipitobregmatic plane just above the level of the sphenoid bone. In this plane, the falx cerebri, the choroid plexus of the lateral ventricle, the brain stem, the fourth ventricle, the cerebellum, and the future CM are all visualized. The fourth ventricle is measured from the posterior border of the brain stem to the posterior border of the fourth ventricle, whereas the future CM is the distance between the posterior border of the fourth ventricle and the anterior border of the occipital bone. The calipers must be placed on the above-described lines (“on-to-on”) in a manner similar to that for measurement of NT. In all cases of OSB, a thickening of the brain stem, a shortening of the distance between brain stem and occipital bone, and an increase in the ratio of brain stem diameter to BSOB distance to greater than 1 are observed. When the tilted axial plane is used and the “single line” sign is observed, this represents the sonographic cluster of early first trimester diagnosis of OSB.
The knowledge of these anatomical landmarks is of significant importance to sonographers in order to enable early detection of OSB. This will allow early clinical prenatal counseling to parents and appropriate management strategy. Further large population prospective studies on both low- and high-risk obstetrical patients are needed to confirm the promising and pioneering observations by Chaoui et al. 3
Footnotes
Acknowledgements
The author thanks Professor Rabih Chaoui and ISUOG for their courtesy and kind permission to reproduce published materials.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.