
Abstract
Placental mesenchymal dysplasia (PMD) has commonly been identified on second trimester ultrasound in association with Beckwith-Wiedemann syndrome (BWS). In this report, a case of PMD later confirmed as Beckwith-Wiedemann is presented, which was identified by sonography in the first trimester. When faced with a first trimester finding of an enlarged cystic placenta, it is suggested that BWS be considered as a possible diagnosis and accordingly, genetic testing with methylation studies offered to the parents.
Introduction
Placental mesenchymal dysplasia (PMD), known also as mesenchymal stem villous hyperplasia, is a rare placental vascular abnormality of unknown etiology with a reported incidence of 2 in 1000 cases.1,2 Due to its relatively new recognition, there is paucity of data with respect to outcome of affected pregnancies. Nevertheless, recent reports, including a systematic review by Nayeri and colleagues, 3 have implicated an association with Beckwith-Wiedemann syndrome (BWS) and adverse perinatal outcomes including intrauterine growth restriction (IUGR) and intrauterine fetal demise (IUFD). The sonographic presentation may demonstrate an enlarged, hydropic, and multicystic placenta. The cysts are typically well defined and may be separated by placental tissue, as opposed to a placental mass primarily comprised of cysts, as may be seen with gestational trophoblastic disease. The fetal anatomy will likely be unremarkable except in cases of associated Beckwith-Wiedemann syndrome. 2 Long-term outcomes are favorable so long as the fetus survives any complications stemming from IUGR and related pathology.
Beckwith-Wiedemann syndrome, which can be due to uniparental disomy of 11p15, is associated with the sonographic findings of macroglossia, macrosomia, organomegaly, abdominal wall defects, and placentomegaly. 4 Fetuses diagnosed with BWS may have favorable outcomes if they survive the neonatal period, although they may have difficulty with feeding or breathing due to macroglossia. Mental status may be normal or slightly reduced. Other possible long-term complications include development of seizures, hypoglycemia, and embryonal tumors such as neuroblastoma and hepatoblastoma. 4 Although recently linked with PMD, the reports have predominantly included second/third trimester or postpartum diagnoses. In the following we present a first trimester case of PMD associated with BWS.
Case Presentation
A 32-year-old gravida 2, para 0 Asian woman was referred to the clinic for a routine first trimester risk assessment and nuchal translucency measurement at 13 weeks and 3 days gestation, based on her last menstrual period. A sonographic examination was performed using a Voluson E8 machine (GE Healthcare, Fairfield, Connecticut, USA). Sonography showed that the fetus demonstrated a normal early anatomic survey and nuchal translucency measurement. However, the placenta appeared enlarged, hydropic, and contained numerous small cystic appearing areas (Figure 1), consistent with PMD. Prenatal diagnostic testing of chorionic villous sampling (CVS) was offered to the patient, which she accepted. The genetic evaluation demonstrated normal 46,XY karyotype and microarray; however, the methylation assay for Beckwith-Wiedemann syndrome proved positive. On follow-up examination (at 16 weeks) to discuss the results of the genetic testing, an isolated small omphalocele was also noted (Figure 2). After genetic counseling and consideration of their options, the couple elected to terminate the pregnancy. Post-delivery gross examination confirmed the presence of an omphalocele along with macroglossia.
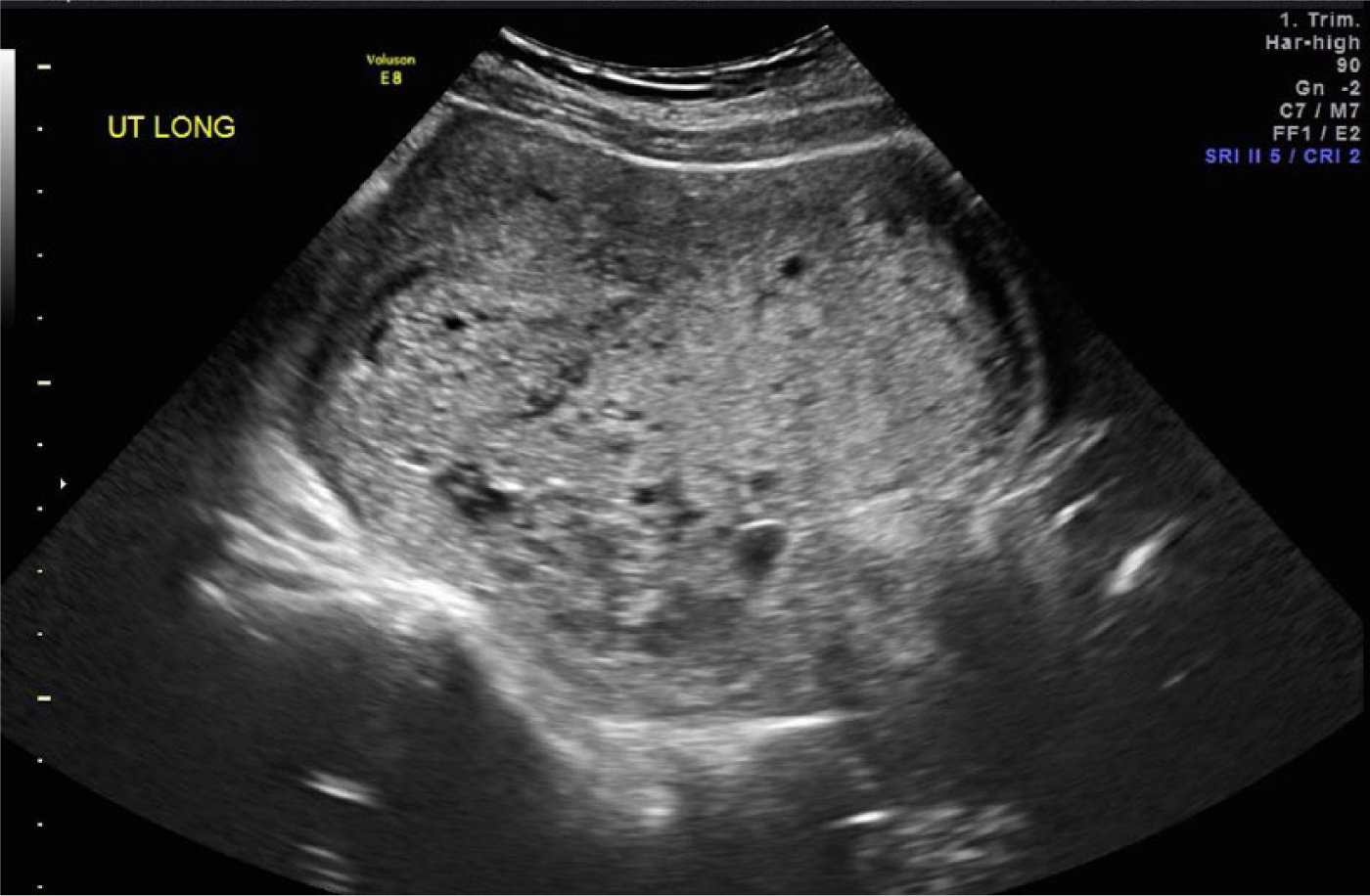
First trimester sonographic image of an enlarged thickened placenta with multiple small cystic appearing areas, consistent with placental mesenchymal dysplasia.
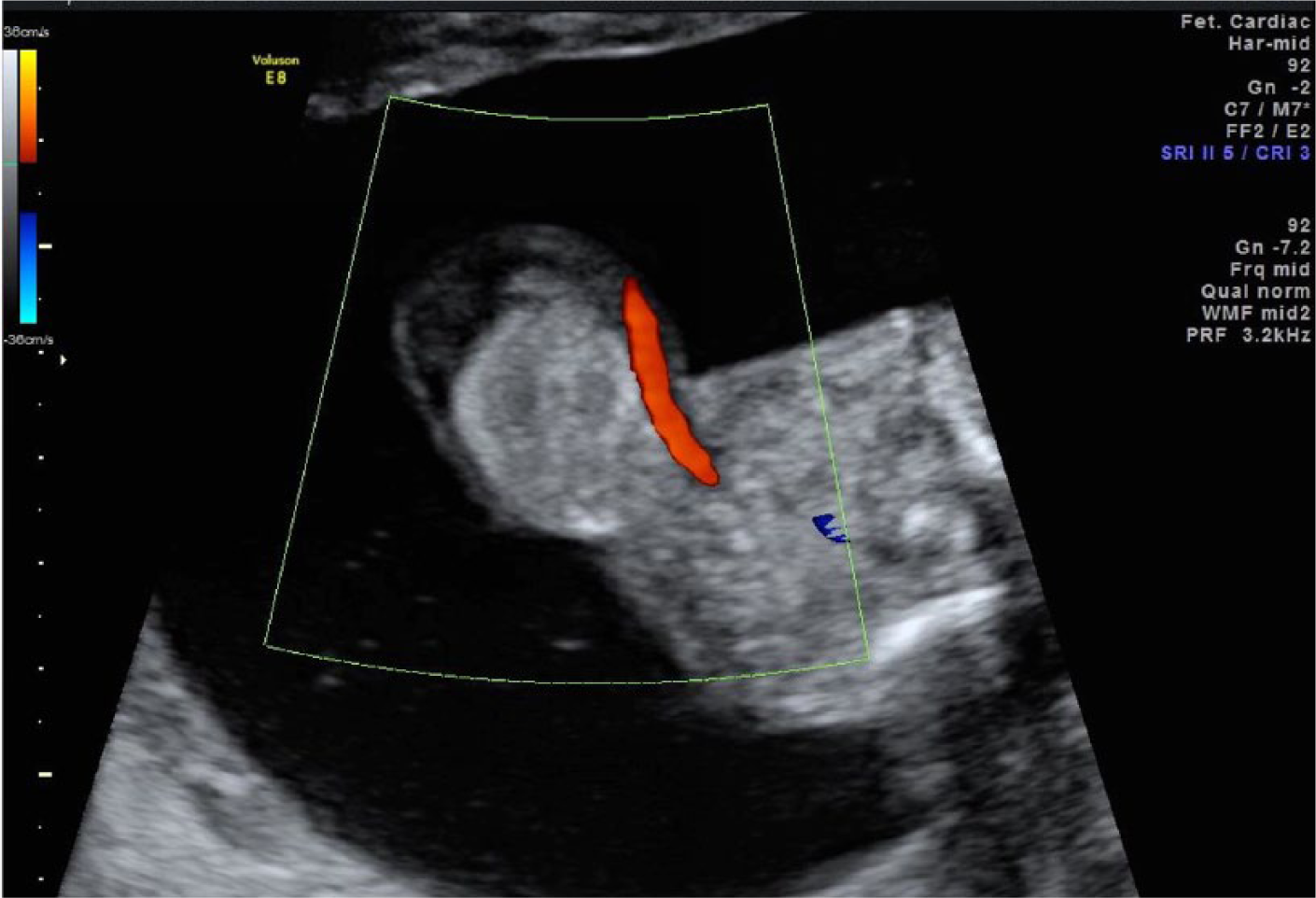
Color Doppler image taken at 16 weeks gestation showing the omphalocele.
Discussion
Prenatal sonographic findings of placental mesenchy-mal dysplasia and an omphalocele in association with Beckwith-Wiedemann syndrome are well documented in the current literature. However, these findings are predominantly described in the second or third trimesters of pregnancy.3–6 Although placental mesenchymal dysplasia has been reported in the first trimester, a literature search showed no reports of first trimester cases in association with BWS, and this is the first reported case.
PMD is underdiagnosed and underreported by many providers, including sonologists, as it is a relatively new entity first described in 1991 by Moscoso et al., 7 and many remain unfamiliar with its presentation.3,7 PMD is often mistaken for gestational trophoblastic disease due to the similarities between the two entities with respect to the placental findings. 3 The well-described first trimester sonographic findings associated with PMD include enlarged placenta, numerous cysts with placental tissue visible between them, and dilated chorionic vessels (Figures 3 and 4). The fetus may be normal but should undergo targeted sonography for signs of IUGR and BWS. Sonographically, the appearance of a cystic placenta may be similar to that of gestational trophoblastic disease. 8 However, in gestational trophoblastic disease the placental mass is often described as hypervascular by color Doppler sonography. In addition, the cystic components may not be well circumscribed and can be so numerous they essentially replace all placental tissue. With molar pregnancy there may not be a fetus at all (complete mole), or if a fetus is identified there may be signs of triploidy (IUGR, hydrocephalus, syndactyly, oligohydramnios) as opposed to the aforementioned signs of a fetus with BWS. It can be difficult to discern a twin pregnancy with a complete mole and a coexistent normal twin. In this case, it is important to identify the placenta of the normal twin to help distinguish from PMD.3,5 Although BWS is associated with presence of an omphalocele (Figure 5), this often may not be diagnosed in the first trimester as there may be physiologic fetal gut herniation. Furthermore, macroglossia and organomegaly are also features, which present later in gestation, all of which underscore the importance of using PMD as a clue for BWS investigation. When faced with the aforementioned sonographic findings, the sonologist should evaluate the preg-nancy for the following differential diagnoses: molar pregnancy (often accompanied by markedly elevated human chorionic gonadotropin levels), chorangioma (often well circumscribed and vascular), subchorionic hematoma (often localized to base of placenta and not the parenchyma), and hydropic placentation (often related to an underlying infection or fetal isoimmunization).6–8 Karyotype should be offered to rule out molar gestation and methylation studies done to assess for BWS. An infectious disease panel should also be carried out.
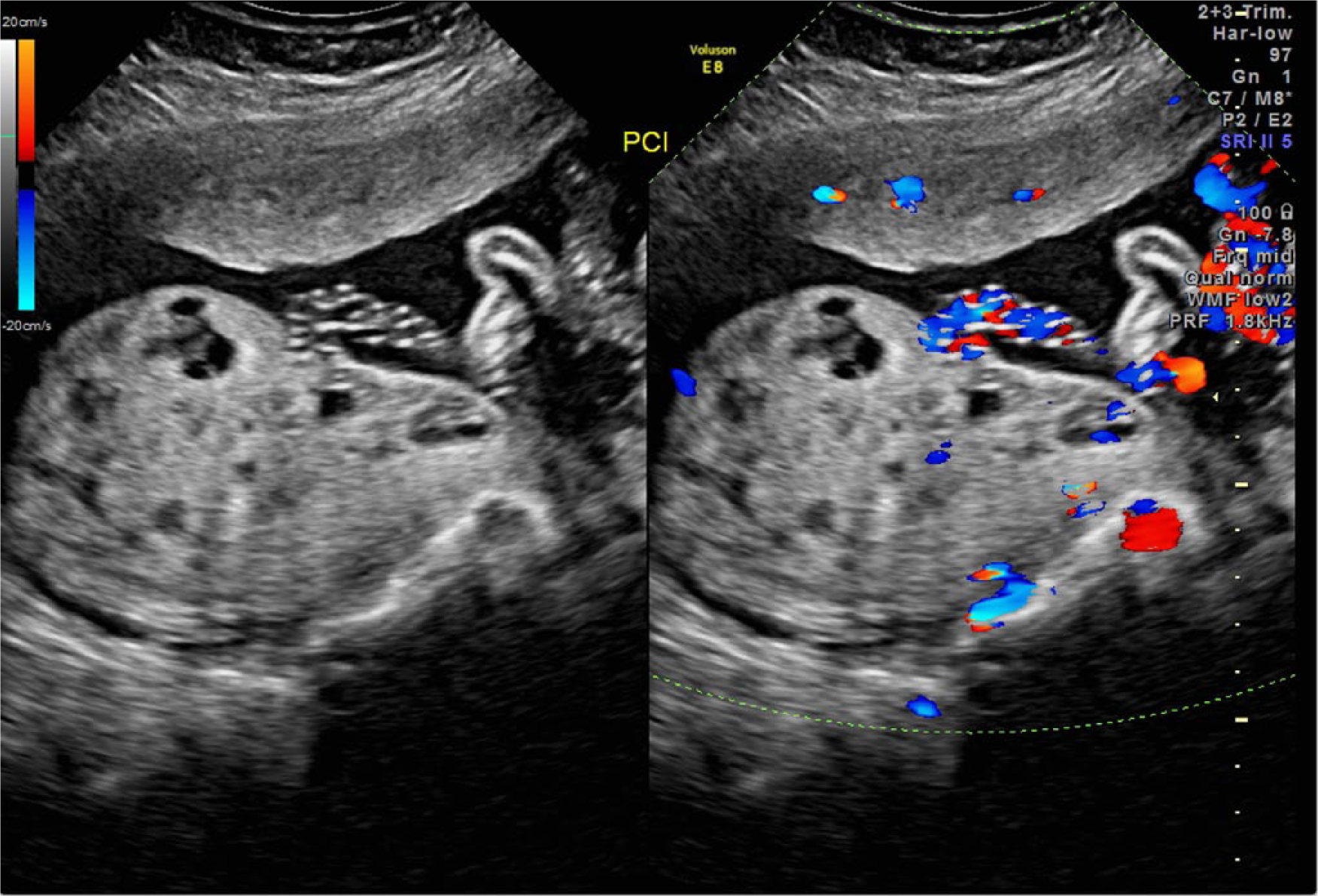
An example of placental mesenchymal dysplasia at 20 weeks gestation showing an enlarged placenta with numerous small cysts and dilated chorionic vessels.
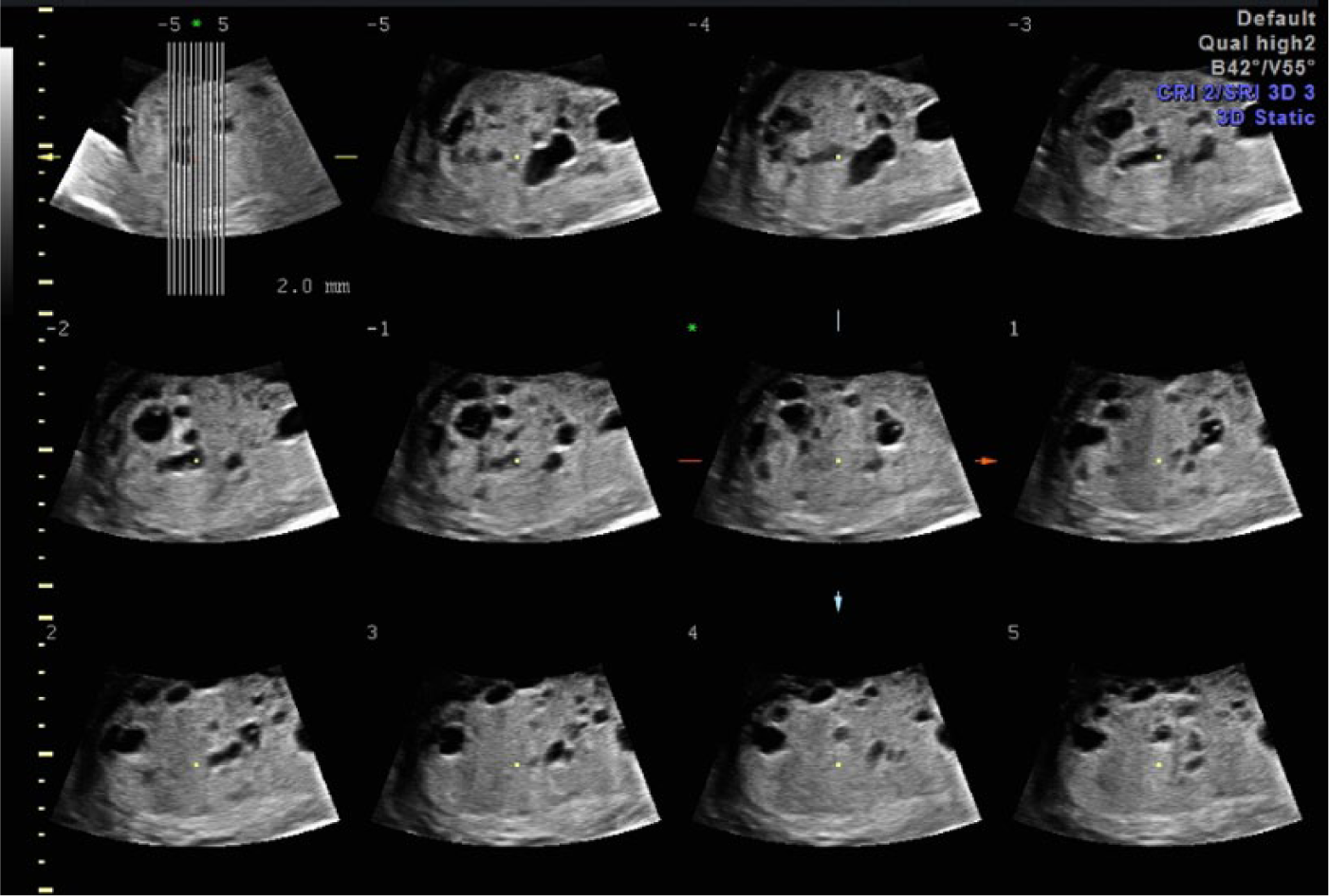
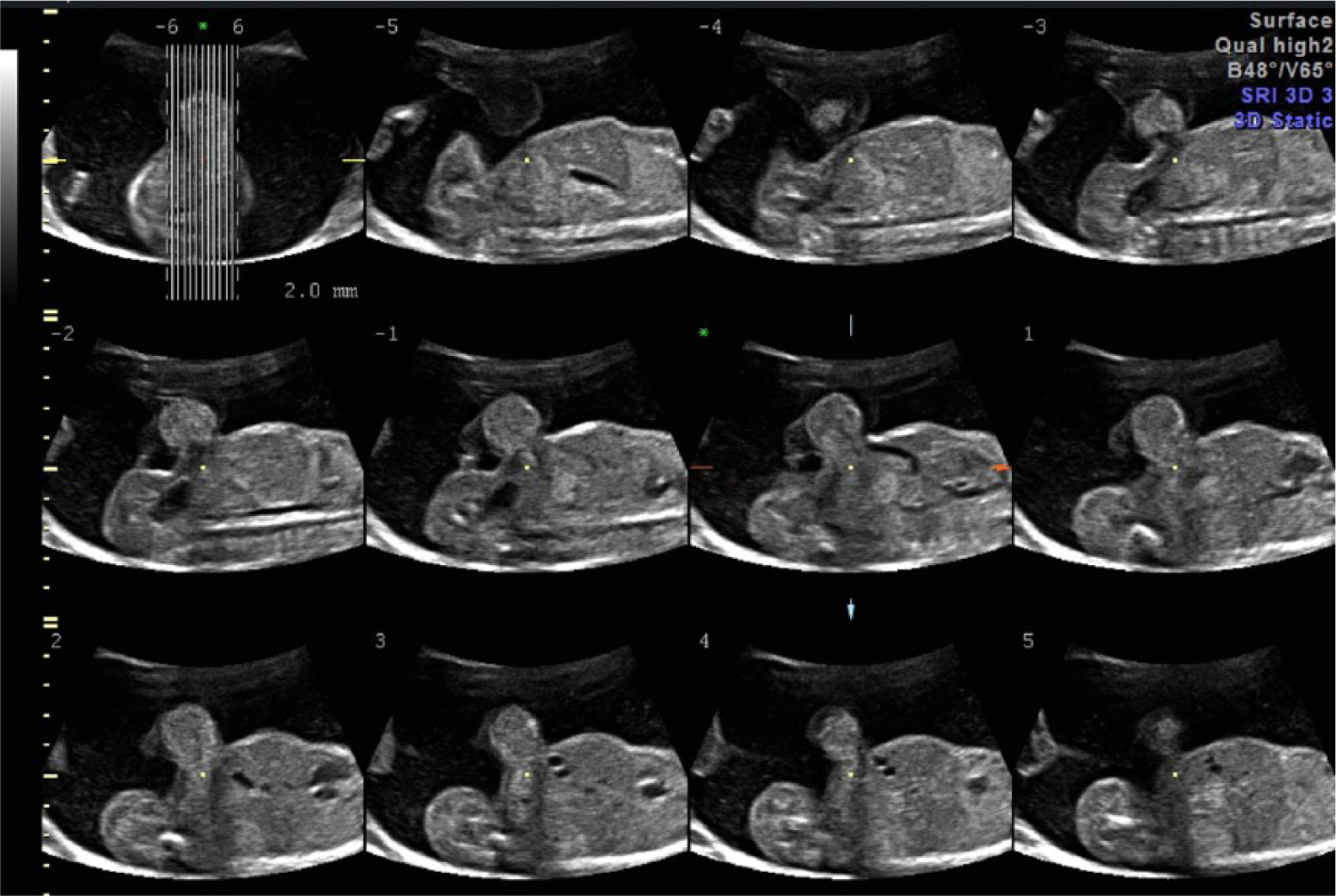
Panel of tomographic ultrasonographic images (TUI) showing an example of placental mesenchymal dysplasia at 20 weeks gestation demonstrating the enlarged thickened placenta with multiple small cystic areas.
Panel of tomographic ultrasonographic images (TUI) showing an example of an omphalocele at 20 weeks gestation.
Conclusion
The first known report of a first trimester case of placental mesenchymal dysplasia in association with Beckwith-Wiedemann syndrome is presented. When faced with a first trimester finding of an enlarged cystic placenta, it is suggested that BWS be considered as a possible diagnosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.