
Abstract
Objective:
Accumulating evidence suggests that abnormal ductus venosus (DV) flow is associated with fetal anomalies. This study aimed to investigate the relationship between quantitative DV Doppler parameters and nuchal translucency (NT).
Materials and Methods:
A total of 76 singleton pregnancies with an NT ≥3 mm were enrolled in the experimental group, and 156 singleton pregnancies with an NT <3 mm were recruited in the control group. Ductus venosus Doppler parameters were collected for both groups. The relationship of the DV Doppler parameters between the two groups and the correlation within the experimental group were analyzed. A receiver-operating characteristic curve was used to determine the best diagnostic cut-off point of DV pulsatility index (DVPI) to indicate a measured NT ≥3 mm.
Results:
There was a significantly higher values for DVPI, DV resistance index (DVRI), and systolic velocity/maximum velocity during atrial wave ratio in fetuses with an NT ≥3 mm compared with those in the control group (P < .00). Fetuses with increased NT, DVPI, and DVRI showed significant positive correlations with NT (P < .00; r = 0.44 and P < .00; r = 0.37, respectively). The best diagnostic cut-off point of DVPI for indicating a measured NT ≥3 mm was 1.15, indicating acceptable performance for the area under the curve of 0.83 (95% confidence interval: 0.770–0.892).
Conclusion:
In this study, in fetuses with an NT ≥3, the DVPI was higher than that in those with an NT <3. In addition, a positive correlation between DVPI and an NT ≥3 was observed.
The nuchal translucency (NT) measurement is now an integral diagnostic element in most first-trimester obstetric screening tests. 1 An enlarged NT is considered to be ≥3 mm and is mainly used as an important indicator, given that aneuploidy is a considerable risk at this threshold. Several studies have been conducted to increase the sensitivity and specificity of imaging-based screening tests. 2 Based on this assumption, adding the diagnostic assessment of the ductus venosus (DV) to NT evaluation has been explored to increase the detection rate of fetal anomalies, such as chromosomal abnormalities and cardiac defects. 3
The DV is the most frequent vein considered for Doppler evaluation during the first trimester of pregnancy. 4 Accumulating evidence indicates that the DV flow profile is the main cardiovascular imaging marker influencing prenatal risk stratification in terms of adverse pregnancy outcomes that would include chromosomal abnormalities and cardiac anomalies.5,6 The DV connects the umbilical vein to the inferior vena cava, providing highly oxygenated blood for fetal circulation. 7 A Doppler examination of the DV is typically performed quantitatively for assessing parameters, such as the DV pulsatility index (DVPI; the most frequent measure), DV resistive index (DVRI), time-averaged maximum velocity (TAMAX), and the ventricular systole/atrial contraction ratio (S/A ratio), or qualitatively focusing on the a-wave. 8
Considering DV Doppler assessment as a relatively inexpensive, accessible method, as well as adding the evaluation of the DV with NT measurement, could improve first-trimester screening for chromosomal abnormalities and congenital heart disease, which could reduce the diagnostic false-positive rate.9,10 Notably, previous research has demonstrated the relationship between DV-derived Doppler and increased NT measurements. 11 Sometimes, NT evaluation can be difficult due to fetal position or maternal body habitus. 12 This diagnostic challenge could yield special attention when making a DV assessment to supplement an increased NT measurement as a first-trimester risk calculation. Given that there is variation in the reference values for NT and DV Doppler indices in different ethnic populations,13 –15 it is plausible to achieve specific ethnicity-related relationships regarding DV Doppler characteristics and NT measurements.
This study aimed to evaluate the association between quantitative DV Doppler parameters, particularly DVPI and NT, in fetuses. This was conducted by recruiting both a control group and an experimental group of fetuses with increased NT measurement, regardless of race and ethnicity.
Materials and Methods
Study Population
This study used a matched case-control research design that enrolled pregnant Caucasian women who attended a tertiary center for a first-trimester sonography screening program between January 2021 and August 2022. The study protocol was approved by the tertiary center’s ethics committee (IRB# IR.MUI.MED.REC.1399.798). The study protocol and minimal risks of the procedures were explained to all participants, and informed consent was obtained. A total of 76 women with singleton pregnancies with an NT ≥3 mm and a crown-rump length (CRL) ranging from 45 to 84 mm (11–13 weeks + 6 days) were included in the experimental group. A control group comprising 156 women with singleton pregnancies with an NT <3 mm and in the same CRL range were recruited. Data on maternal age, CRL, NT, DVPI, DVRI, TAMAX, and S/A ratio were collected for all participants. All participants in the experimental group were advised to undergo amniocentesis and fetal echocardiography. A normal pregnancy outcome was confirmed for all patients in the control group after delivery, based on a detailed report by a neonatal pediatrician.
Sonographic Assessment
The sonographic examination included NT and CRL measurements and quantitative DV Doppler assessments performed by an obstetrics-focused radiologist with more than 10 years of experience (S.H.). All studies were performed using the Voluson E8 ultrasound equipment system (GE Healthcare, Milwaukee, Wisconsin) and the transabdominal scanning method. For good-quality NT measurement, the following criteria were considered: the image should be magnified to occupy 75% of the screen and show only the fetal head, neck, and upper thorax. The fetus must be located in the midsagittal plane. The fetal neck must be in the neutral position and should not be hyperextended or hyperflexed. Three echogenic lines indicating the inner and outer borders of the fetal skin and amnion must be visualized. Electronic calipers must be placed with a horizontal cross on the inner borders of the echolucent space, vertical to the fetal axis. The NT measurement must be performed at the widest space. 16
Several technical conditions were considered during DV Doppler assessments: measurements were performed when the fetus was in a state of inactivity, DV was examined using color Doppler imaging in a right ventral midsagittal plane, the distal portion of the umbilical sinus was the target on which the pulsed Doppler gate was placed, a Doppler gate of 0.5 to 1 mm in width was placed over the yellowish aliasing region closely above the umbilical sinus, the waveform was obtained with the smallest possible angle of insonation (≤30°) with at least three typical consecutive waveforms, a low-frequency filter between 50 and 70 Hz was selected, and the sweep speed was set to 2 to 3 cm/s to widely spread the waveforms. Moreover, adherence to the “as low as a reasonably achievable principle” was considered during all the sonographic examinations. 17 After obtaining high-quality spectral Doppler waveforms, manual tracing was performed, and DVPI, DVRI, TAMAX, and S/A ratio were calculated based on the software loaded on the ultrasound equipment system. To improve the reproducibility of the examination, the DV waveform was evaluated three times per patient, and the mean of the Doppler indices was retained for data analysis (Figure 1).
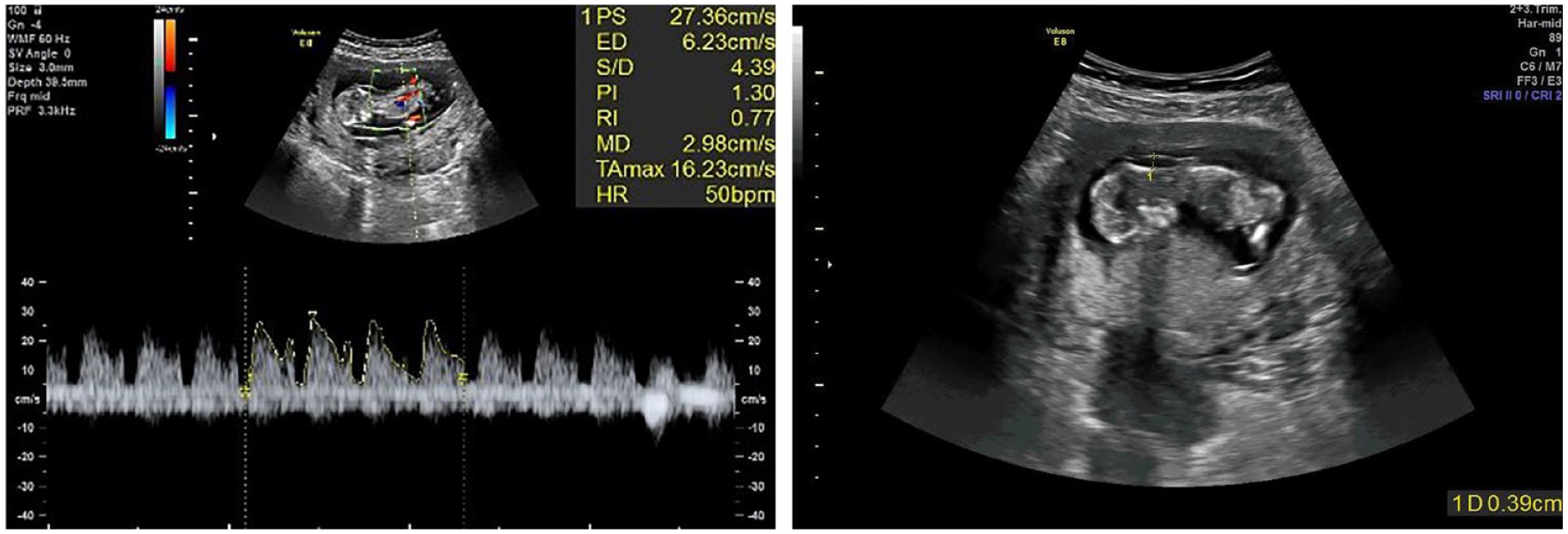
Sample images of the color and spectral Doppler investigation of the ductus venosus (DV) (right). Three typical DV waveforms were manually traced, and DV Doppler indices were extracted. The nuchal translucency (NT) measurement of the same fetus is demonstrated (left).
Statistical Analysis
The data were analyzed using SPSS version 18.0 computer software (Statistical Package for Social Sciences, Chicago, Illinois). An independent t test was used to compare DV Doppler parameters and other continuous characteristics between the experimental and control groups. The correlation between DV Doppler indices and increased NT in the experimental group was calculated using Pearson’s correlation coefficient. To determine the optimal cut-off value of DVPI for predictive performance in terms of increased NT (≥3 mm), a receiver-operating characteristic (ROC) curve analysis was performed. Statistical significance was set at P < .05, a priori.
Results
A total of 232 pregnant women (76 in the experimental group and 156 in the control group) were enrolled in this study. The general characteristics of the two study groups are presented in Table 1. Of all the participants with increased NT, 56 consented to further evaluation by a perinatologist. Among these, 41 women underwent amniocentesis; 33 had normal karyotypes and eight had abnormal karyotypes. Therapeutic termination was performed in all pregnancies with abnormal karyotypes. Of the 33 fetuses with normal karyotypes, 27 were normal neonates and three had cardiac anomalies. In addition, therapeutic termination was performed for the three remaining patients with normal karyotypes based on findings from the second-trimester screening. Among the participants, 15 were under the supervision of the perinatologist. These participants did not undergo amniocentesis; however, missed abortion was documented in 12 pregnancies (14–16 weeks), and therapeutic termination was performed in three due to fetal hydrops.
The Participant’s Baseline Demographic and Clinical Data.

The relationship between the DV Doppler parameters between the experimental and control groups is shown in Table 2. There were significantly higher values for DVPI (P < .001), DVRI (P < .001), and S/A ratio (P < .001) in fetuses with an NT ≥3 mm than in their counterparts with an NT <3 mm. TAMAX demonstrated no significant association between the two groups (P = .09).
Doppler Parameters of the Ductus Venosus in the Experimental Versus Control Groups.
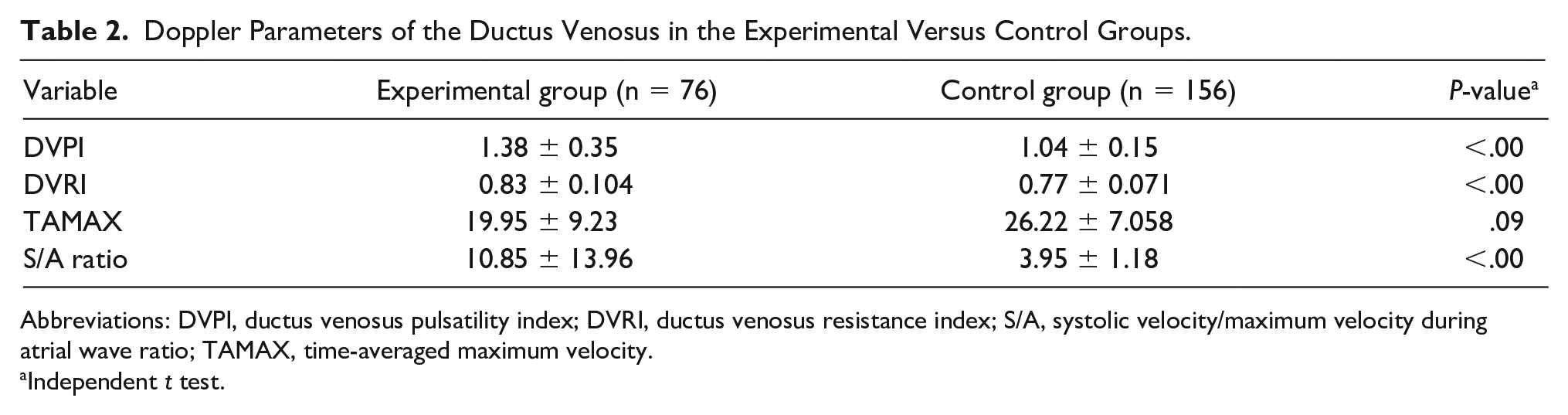
Abbreviations: DVPI, ductus venosus pulsatility index; DVRI, ductus venosus resistance index; S/A, systolic velocity/maximum velocity during atrial wave ratio; TAMAX, time-averaged maximum velocity.
Independent t test.
As shown in Table 3, in fetuses with an NT ≥3 mm, a significant positive correlation between DVPI and DVRI was observed, with an increased NT (P < .001; r = 0.44 and P < 0.001; r = 0.37, respectively), while TAMAX and the S/A ratio did not show any correlation (P = .44 and P = .025, respectively).
The Ductus Venosus Doppler Parameters and Correlation With Nuchal Translucency.
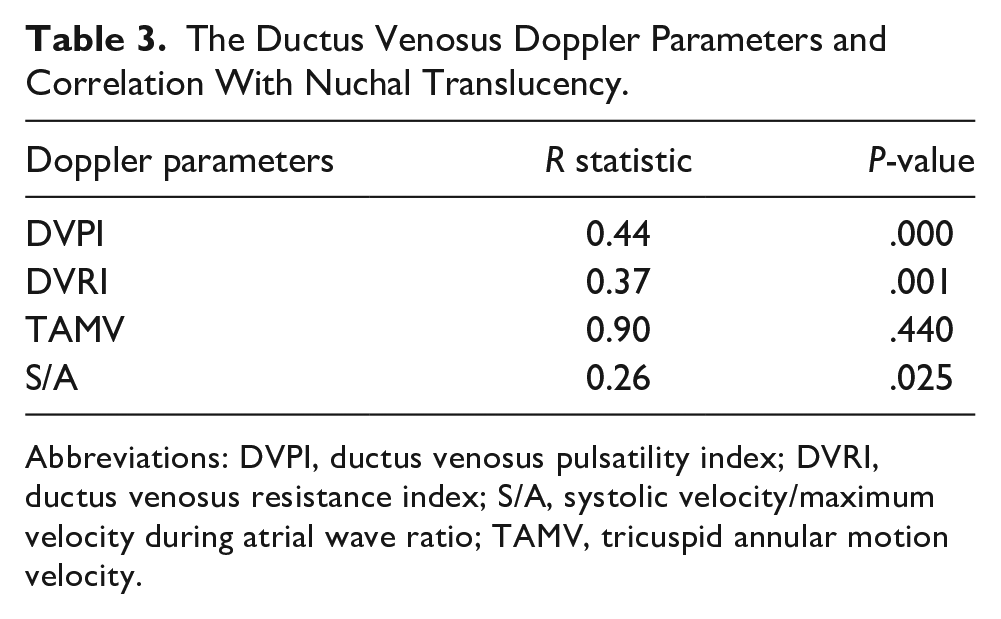
Abbreviations: DVPI, ductus venosus pulsatility index; DVRI, ductus venosus resistance index; S/A, systolic velocity/maximum velocity during atrial wave ratio; TAMV, tricuspid annular motion velocity.
To determine the best diagnostic DVPI cut-off point for predicting NT ≥3 mm, an ROC curve analysis was performed. The best DVPI cut-off point was 1.145 for predicting increased NT, with a sensitivity of 73.7% and specificity of 80%. The area under the ROC curve (AUC) was 0.83 (95% confidence interval [CI]: 0.77–0.89) for DVPI with acceptable discriminatory performance (Figure 2).
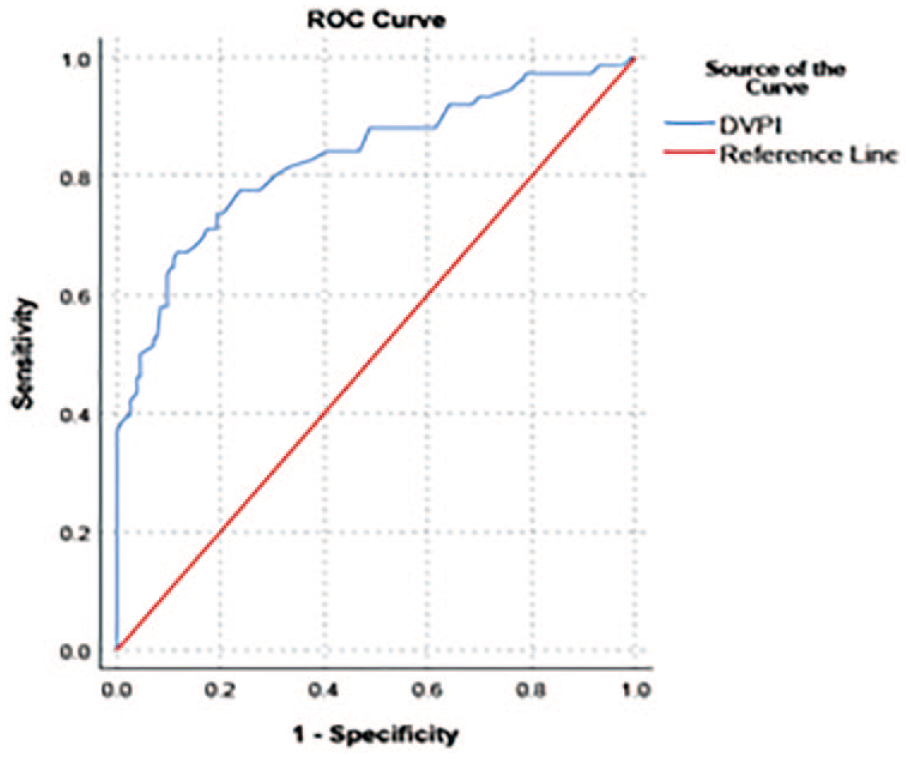
The receiver-operating curve (ROC) is provided for predicting nuchal translucency (NT) ≥3 mm by ductus venosus pulsatility index (DVPI).
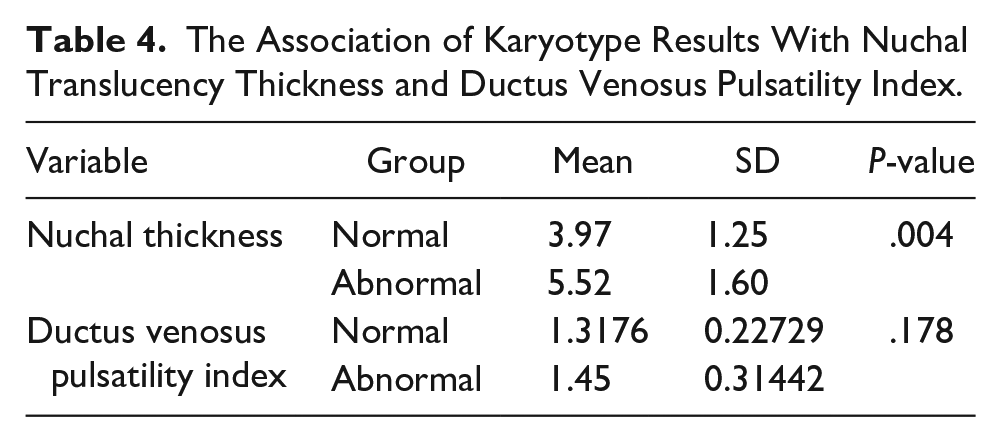
In a subgroup analysis of the participants who underwent karyotyping, the association between NT and DVPI with karyotyping results was investigated. As demonstrated in Table 4, fetuses with abnormal karyotypes had a value of 5.52 ± 1.60 mm for NT, while in those with normal karyotypes, the NT value was 3.97 ± 1.25 mm (P < .004). However, DVPI values did not show a significant difference in terms of karyotype results (1.317 ± 0.227 in normal karyotypes vs 1.450 ± 0.314 in abnormal karyotypes; P = .178).
The Association of Karyotype Results With Nuchal Translucency Thickness and Ductus Venosus Pulsatility Index.
Discussion
The current study investigated the potential relationship between DV quantitative Doppler parameters and NT using a matched case-control research design. Ductus venosus Doppler indices, especially DVPI, were significantly higher in fetuses with NT ≥3 mm than that in those with NT <3 mm. In addition, a significant correlation was observed between the DVPI and DVRI with increasing NT thickness. Notably, a DVPI cut-off of 1.145 had acceptable predictive performance for NT ≥3 mm.
Regarding the highest forward velocities of DV in the fetal venous system with an entirely antegrade flow, quantitative waveform analysis of DV is widely accepted. 18 Moreover, NT measurement is central to first-trimester obstetrical screening programs. 19 Given the hemodynamic dysfunction as the most important pathophysiological mechanism of an increased NT, any relation between DV-related Doppler parameters and NT thickness was investigated. 20 A previous research, based on an Iranian sample of participants, determined the DVPI reference values in 451 normal singleton pregnancies. Based on a limited literature search, this was the first study to investigate the relationship between DVPI and NT in an Iranian sample of participants.
The major findings were a significantly higher value of DVPI in fetuses with NT ≥3 mm than in those with NT <3 mm, as well as a significant positive correlation between DVPI and increased NT in the experimental group. Similar findings were obtained in the study of 186 fetuses in the first-trimester screening evaluation; a significant correlation was observed between NT and DVPI in their overall study population. 21 Inconsistent with the present study results, Borrell et al 22 found that in the small group of 11 fetuses with trisomy 21, the correlation between NT and DVPI was poor, while concordant findings were observed in 7 of the 11 fetuses.
Maiz et al 20 demonstrated that the prevalence of abnormal DV waveforms positively increased when NT was enlarged in fetuses without major cardiac defects. Another study reported abnormal DVPI in 41.8% of 318 fetuses with an NT above the 95th percentile. 23 Taken together, a positive correlation between DVPI and increased NT was documented in the current study and nearly all aforementioned reports. Accordingly, using the ROC curve analysis, an acceptable predictive value of the DVPI was obtained for increased NT measurement. Consequently, the DVPI could potentially be used to increase the effectiveness of first-trimester screening tests. Recently, several studies have been conducted to improve screening performance by including DV Doppler parameters for the detection of chromosomal abnormalities and cardiac anomalies, and the concept of incorporating DV Doppler measurement in screening programs is becoming the prevailing diagnostic trend.24 –26
Limitations
The current study has two major limitations. The research design poses a threat to internal and external validity owing to the lack of randomization in assigning patients to groups. Moreover, the sample size was relatively small, and this was a single-institutional investigation; therefore, selection bias was not inevitable. Future studies with prospective multicenter design and a larger sample size are needed.
Conclusion
The current study showed that, in the first trimester, DVPI was higher in cases with an NT ≥3 mm than in those with an NT <3 mm. Furthermore, a correlation between the increased DVPI and NT values was observed. DVPI had acceptable performance based on AUC for predicting NT ≥3 mm and unfavorable fetal development.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Ethics Committee of Isfahan University of Medical Sciences (IR.MUI.MED.REC.1399.798).
Informed Consent
Written informed consent was obtained from all participants before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Key Takeaways
1. A combined examination of fetal DVPI and NT measurements could complement screening for chromosomal abnormalities and congenital heart disease in the first trimester.
2. Previous studies have demonstrated a relationship between DV-derived Doppler characteristics and increased NT.
3. There was a correlation between increased DVPI and NT; DVPI alone had acceptable performance, based on the AUC for predicting NT ≥3 mm.