
Abstract
Osteoarthritis of the sternoclavicular joint (SCJ) is a common entity. Plain radiographs and computed tomographic scans are the modalities commonly used for diagnosis of SCJ osteoarthritis. Classical imaging findings are joint space narrowing, marginal sclerosis, and osteophyte formation. Widespread application of ultrasonography (US) in the evaluation of multiple musculoskeletal pathologies has been made recently. However, the sonographic features of SCJ osteoarthritis have not been reported. We report a case of unilateral SCJ osteoarthritis in a patient with rheumatoid arthritis (RA) and describe its typical sonographic features.
Introduction
Common pathological entities affecting the sternoclavicular joint (SCJ) include osteoarthritis, rheumatoid arthritis, and infection. Involvement of the SCJ in rheumatoid arthritis is reported to range from as low as 1% to as high as 41% in different series.1-3 However, isolated osteoarthritis of the SCJ without involvement of other joints may be common. 1 The classic features of SCJ osteoarthritis such as joint space narrowing and sclerosis may not be evident in conventional radiography due to overlapping shadows or structural variability.2,4 Clinicians have significant diagnostic and therapeutic challenges while managing patients with SCJ symptoms when there is a clinical history of rheumatic diseases such as rheumatoid arthritis. Computed tomographic (CT) scans of the SCJ are the most commonly used diagnostic modality in this scenario, as CT is able to show the typical changes of SCJ osteoarthritis. There is also an increasing role for sonography, with its capabilities of high-resolution real-time imaging and such features as color Doppler imaging, in various rheumatic disorders including both rheumatoid arthritis and osteoarthritis. Specific to the sternoclavicular joint, however, there are no data regarding the sonographic features of SCJ osteoarthritis. 5 This report presents a case of SCJ osteoarthritis in a patient with rheumatoid arthritis, a problem encountered frequently in clinical practice, and describes the typical sonographic features of this disease.
Case Report
A 44-year-old female presented to the rheumatology outpatient clinic with a three-month history of painless enlargement of the right sternoclavicular joint. She was known to have seropositive rheumatoid arthritis (RA), which was diagnosed three years previously. At the time of diagnosis, her disease activity was considered to be moderate according to the Disease Activity Score (DAS28) scale, 6 an index measuring the degree of disease activity in RA patients in which 28 selected joints are evaluated for evidence of tenderness and swelling. This score has been validated against physical function and radiographic progression in RA. 6 A score >5.2 is considered indicative of high disease activity. In RA, DAS28 scoring is recommended as a basis for decisions regarding treatment initiation and alteration. 3
Physical examination at the present visit showed hard, non-tender swelling over the right sternoclavicular joint with a mild limitation of right shoulder shrugging in comparison to the left. Rheumatoid arthritis disease activity was low at this time (2.8 on the DAS28 scale). Sonography of the right sternoclavicular joint showed reduction of the joint space and irregularity of the medial end of the clavicle (Figure 1) along with osteophyte formation (Figure 2). No hypervascularity of the right SCJ was noted by color or spectral Doppler. Color Doppler imaging of the wrist did show a mild degree synovial hypervascularity (Figure 3). These classical sonographic features strongly suggested a diagnosis of osteoarthritis of the right sternoclavicular joint, and this was confirmed by CT scan. The patient’s anti-rheumatoid medications were kept unchanged, and a period of rest and physiotherapy produced good clinical improvement in respect to pain reduction and shoulder mobility.

Gray-scale image of the right sternoclavicular joint showing significant cortical irregularity of the medial end of the clavicle.

Gray-scale image of the right sternoclavicular joint showing significant joint space reduction and osteophyte formation at the medial end of the right clavicle; the corresponding image of the medial end of the left clavicle is shown for comparison.
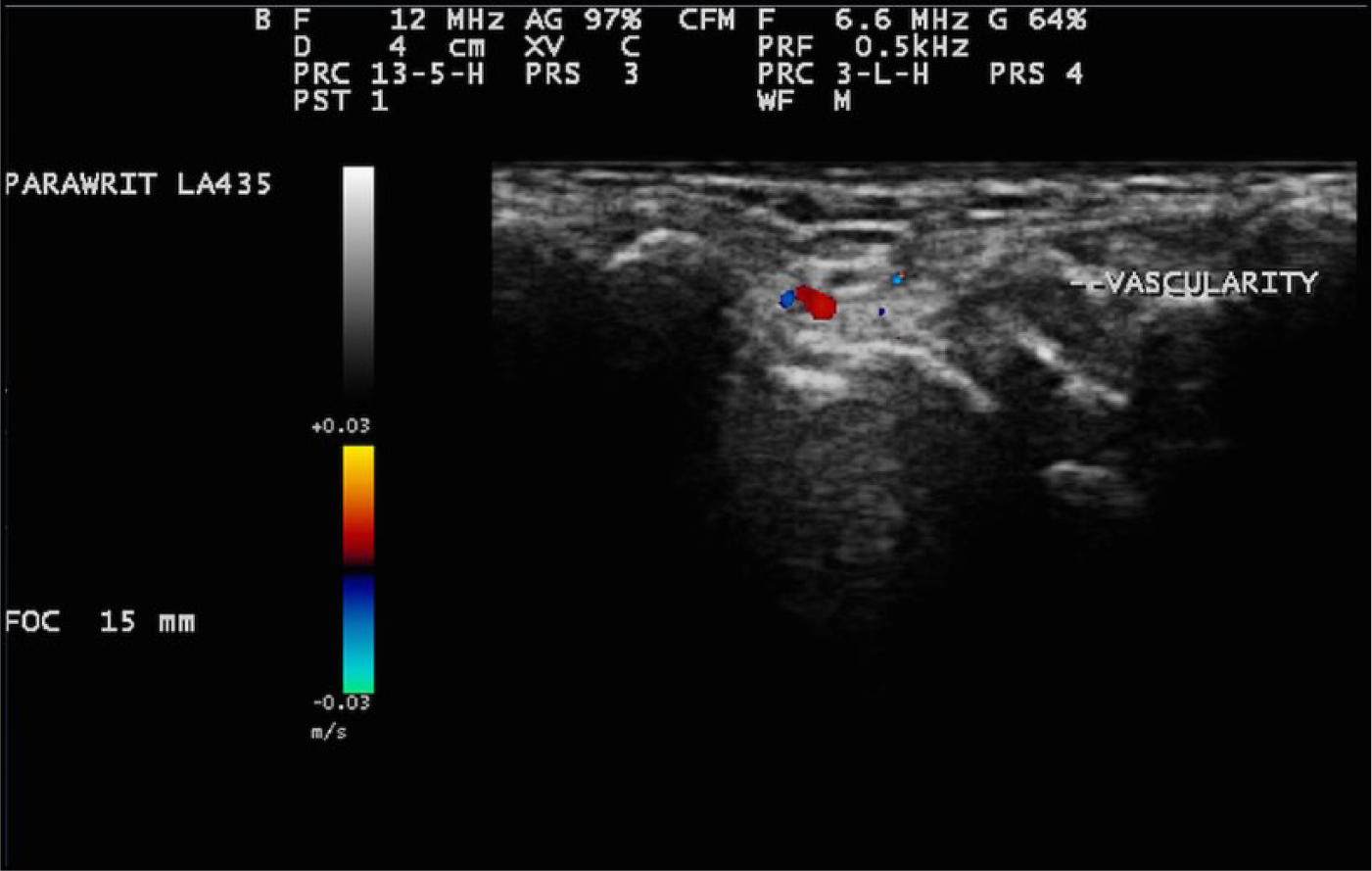
Color Doppler image of the wrist joint in the same patient showing a mild degree of synovial hypervascularity characteristic of rheumatoid arthritis.
Discussion
While osteoarthritis is the most common abnormality affecting the SCJ, other degenerative diseases and rheumatoid arthritis also can affect the joint.4,7 The history of rheumatoid arthritis presented a diagnostic challenge in determining the etiology of the present (new) symptoms in the patient presented here, as sternoclavicular joint pain could have been caused by rheumatoid arthritis itself or be secondary to some other degenerative disorder. Osteoarthritis commonly affects the SCJs bilaterally. 1 The recognized risk factors for SCJ osteoarthritis are postmenopausal status and a history of manual labor. 7 Patients typically present with mild pain, swelling, and limitation of shoulder joint movement. Restriction of shoulder movement is particularly seen in unilateral involvement. 1 A CT scan or magnetic resonance imaging (MRI) are the commonly used modalities for diagnosis of sternoclavicular joint pathology. 4 Classical CT scan findings are joint space narrowing, osteophyte formation, and bony sclerosis, similar to degenerative diseases of other arthroidal joints (Figure 4). 8 Bone marrow, cartilage, and extra-articular soft tissue are better delineated by MRI, though MRI can also demonstrate the joint space narrowing, capsular hypertrophy, and osteophyte formation, which are typically seen in osteoarthritis. 9
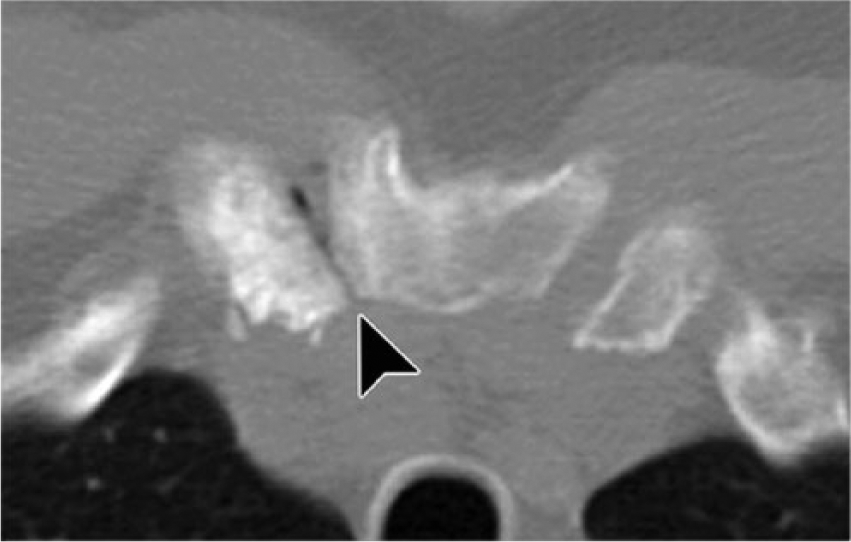
Computed tomographic scan of the sternoclavicular joint in a patient with osteoarthritis, showing osteophytosis, sclerosis, and subtle subchondral cyst formation (arrow head). Intra-articular gas is also seen. Reproduced with permission from Restrepo CS, Martinez S, Lemos DF, et al. Imaging appearances of the sternum and sternoclavicular joints. Radiographics. 2009;29(3):839-59. Copyright 2013 Radiological Society of North America.
Sonography is emerging as a valuable diagnostic tool in rheumatic diseases. 5 Gray-scale sonography, complemented by color Doppler imaging, is able to demonstrate the classical findings of SCJ osteoarthritis, but there is very little in the literature regarding sonographic features of arthropathy of this joint. Degenerative osteoarthritis of the sternoclavicular joint is sonographically characterized by narrowing of the sternoclavicular joint space, osteophytosis, and para-articular cyst formation. Synovial hypervascularity is usually absent in osteoarthritis of the SCJ. Rheumatoid arthritis of the SCJ was another important diagnostic consideration in the patient presented, especially with a known history of this disease. On sonography, the osteophytosis of the medial end of the clavicle, along with joint space narrowing, were more characteristic of degenerative pathology of the SCJ. In rheumatoid arthritis of the SCJ, sonography typically shows widening of the joint space and osseous irregularity, In addition, the absence of hypervascularity in the affected joint by color Doppler imaging excluded the likelihood of RA, which usually shows synovial hypervascularity. A mild degree of synovial hypervascularity was seen in the wrist joints of the patient secondary to RA disease activity.
Conclusion
Sonography can be a useful initial diagnostic modality in SCJ osteoarthritis as it can detect typical articular changes, even if conventional radiography is negative. However, more work is required to develop the necessary standardized definitions of pathology and demonstrate the validity of ultrasonography in osteoarthritis in larger numbers of patients. Application of sonography to osteoarthritis may enhance the understanding of the disease process and the relationships between the anatomic abnormalities and symptoms, and it also may aid in the assessment of future therapies.
Footnotes
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.