
Abstract
Dermoid cysts are rare benign tumors that arise from ectopic epiblastic inclusions and account for 0.4% to 1.5% of all tumors. They are usually 1 to 5 cm in size and composed of a pasty semisolid material. The orbital dermoid cyst is the most common type. Dermoid cysts can also occur in the spinal cord, ovaries, and pancreas. We encountered a 24-year-old man with a dermoid cyst over the left sternoclavicular joint. He reported intermittent secretion of a white tofu-like exudate from an underlying congenital sinus tract since birth. The secretion had turned hemorrhagic for the last month and had been accompanied by progressive swelling and pruritus for 1 week. Ultrasonography and magnetic resonance imaging revealed characteristics of a dermoid cyst, and histopathological examination confirmed the diagnosis. The patient underwent surgical excision of the cyst under local anesthesia. The incision healed well with no postoperative complications. Considering that a dermoid cyst has the potential to become infected or progress into squamous cell carcinoma, its removal at an early stage is suggested. Few reports in the literature have described a dermoid cyst that secretes hemorrhagic contents from a congenital sinus tract. We present this case to provide a reference for clinicians.
Keywords
Introduction
A dermoid cyst is a rare type of benign tumor arising from ectopic epiblastic inclusions, and it accounts for 0.4% to 1.5% of all tumors. 1 The incidence of dermoid cysts is roughly 3 per 10,000 pediatric patients. 2 Dermoid cysts are usually 1 to 5 cm in size and consist of a pasty semisolid material. 3 Among the different types of dermoid cysts, orbital dermoid cysts occur most frequently. Dermoid cysts can also occur in the spinal cord, ovaries, and pancreas.4–6 However, a dermoid cyst with a concomitant congenital sinus tract that drains an exudate has rarely been reported in the literature. We herein present such a case to provide a reference for clinicians.
Case presentation
A 24-year-old man presented with a gradually increasing mass in a congenital sinus tract located in the region of the left sternoclavicular joint (Figure 1). This subcutaneous mass, which had been present since birth, was smooth, fluctuant, and adherent to the surrounding tissues. A congenital sinus tract was present inside the cystic mass and intermittently secreted a white tofu-like content. The exudate had turned hemorrhagic about 1 month previously. The sinus tract had closed 1 week previously, after which the swelling progressively increased in size and pruritus developed.

The dermoid cyst localized over the left sternoclavicular joint.
The patient underwent ultrasonography and magnetic resonance imaging (MRI) to identify the features of the subcutaneous mass. Ultrasonography showed a hypoechogenic, well-defined lesion in the skin and subcutaneous fat layer over the left sternoclavicular joint. The lesion was approximately 1.2 × 0.9 × 0.5 cm in size (Figure 2). There was a flocculent, heterogeneous echo in the cystic lesion that seemed to flow under probe pressure. Color Doppler flow imaging revealed signals of peripheral blood flow. The cystic mass appeared isointense on T1-weighted sequences and showed high signal intensity on T2-weighted sequences (Figure 3). The cyst was excised under local anesthesia. The mass was identified as a dermoid cyst by histopathological examination (Figure 4). Hematoxylin and eosin staining revealed that the dermoid cyst wall was surrounded by squamous epithelium and keratosis, and no cutaneous appendages were observed in the cyst. Chronic infiltration of macrophages and multinucleated cells was observed, implying a foreign body inflammatory reaction. Based upon the above findings, it was reasonable to deduce that the hemorrhagic exudate was due to infection, leading to local swelling and subsequent blockage of the sinus tract. Accordingly, surgical resection was suggested. The incision healed well after surgery with no complications. The patient developed no recurrence during 3 years of follow-up. The institutional review board of the Third Hospital of Hebei Medical University approved this study. Informed written consent was obtained from the patient for publication of this case report and accompanying images.

Ultrasonography. A hypoechogenic well-defined lesion of 1.2 × 0.9 × 0.5 cm in size in the skin and subcutaneous fat layer.

Magnetic resonance imaging. The cystic mass (a) appeared isointense on T1-weighted sequences and (b) showed high signal intensity on T2-weighted sequences.
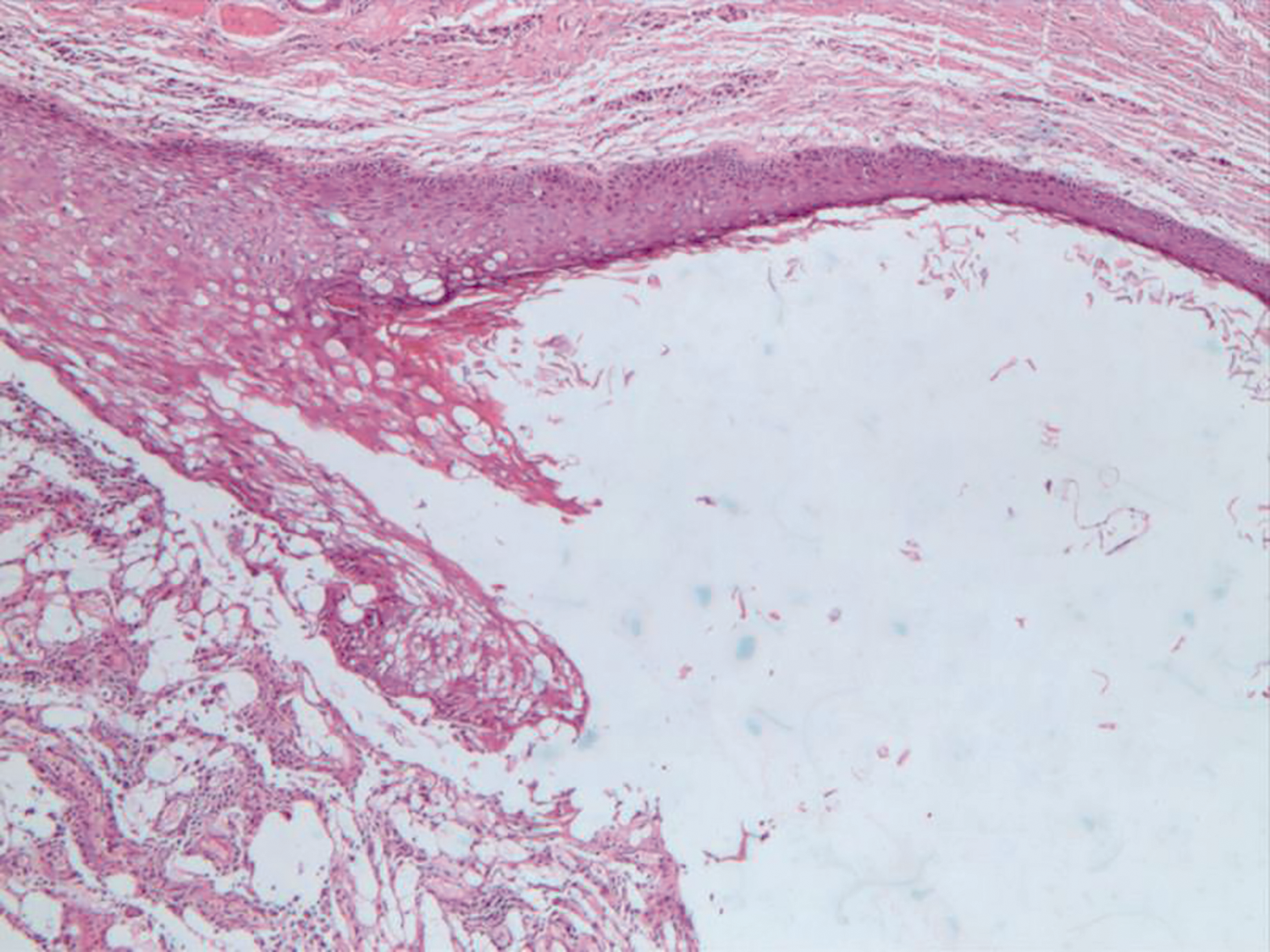
Hematoxylin and eosin staining. The dermoid cyst wall was surrounded by squamous epithelium, keratosis, and chronic inflammation characterized by macrophages and multinucleated cell infiltration (×40).
Discussion
Dermoid cysts are usually located in the midline of the human body. They are commonly found in the periorbital region and can also be seen in the spinal cord, ovaries, and pancreas.5–8 There is no sex predominance. Dermoid cysts can be divided into congenital and implantable dermoid cysts. Congenital dermoid cysts are more likely to occur on the embryo fusion line because of ectodermal isolation. Nonetheless, dermoid cysts may not appear until late childhood or even later. Implantable dermoid cysts have different pathogenesis. They occur secondary to epidermal mechanical implantation of subcutaneous tissue secondary to injury or surgery. 9 Because dermoid cysts have the possibility of progressing into squamous cell carcinoma, 10 surgical intervention is often suggested to remove this lesion. 11
In this report, we have described a patient with a dermoid cyst along with a concomitant discharging congenital sinus tract located in the region of the left sternoclavicular joint. Ultrasonography showed a hypoechogenic, well-defined lesion in the skin and subcutaneous fat layer that appeared similar to a typical dermoid cyst. However, visual inspection, MRI, and histopathological examination revealed several differentiating features.
First, a dermoid cyst secreting hemorrhagic contents from a congenital sinus tract has rarely been reported in the literature. In our patient, the congenital sinus tract underlying the dermoid cyst had been secreting white tofu-like contents since birth. The exudate had turned hemorrhagic 1 month before the patient sought medical advice. The sinus tract had closed 1 week before he visited the hospital, leading to progressive swelling and pruritus, which are signs of infection. Second, hematoxylin and eosin staining demonstrated chronic infiltration of macrophages and multinucleated cells in the dermoid cyst, which are features of a foreign body inflammatory reaction. Therefore, we deduced that the hemorrhagic exudate was due to infection, leading to local swelling and subsequent blockage of the sinus tract. Third, the MRI scan revealed that the dermoid cyst wall was hypointense on both T1- and T2-weighted sequences. Hypointense lesions are consistent with fibrous tissue. However, T1- and T2-weighted sequences showed heterogeneous signals from the dermoid cyst, which might have been due to different compositions of the cyst. 12
In short, we have herein described a patient with a dermoid cyst associated with a congenital sinus tract located in the region of the left sternoclavicular joint. The cyst had become infected, leading to blockage of the sinus tract. It has been suggested that a dermoid cyst should be resected at an early stage because of its possibility of becoming infected or progressing into squamous cell carcinoma.