
Abstract
Sternoclavicular joint septic arthritis is rare and commonly associated with specific risk factors. We report the case of a 58-year-old female with no previous medical or surgical history who presented complaining of a warm, indurated mass overlying the right sternoclavicular joint. Computed tomography of the chest showed erosion of the sternal end of the clavicle and the manubrium sternum associated with thickening of the synovium and a sternoclavicular joint space narrowing, suggestive of an infective process. Intraoperative finds a purulent collection extending both over the clavicle and the sternum. Limited destruction of small parts of the sternoclavicular joint was noted. The abscess was drained. Simple debridement and limited curettage were preferred to en bloc resection given the limited size of necrotic tissues. Sternoclavicular joint septic arthritis is a condition with significant morbidity and potential mortality. All medical practitioners must maintain a high degree of suspicion, even in healthy patients, as it can lead to serious complications.
Introduction
Sternoclavicular joint (SCJ) septic arthritis (SCJSA) is rare and represents less than 1% of all bone and joint infections. 1 Most cases of SCJSA are reported in patients with predisposing factors such as immunosuppressive disorders and heroin addiction. 2 Nevertheless, up to 25% of SCJSA can occur in otherwise healthy patients. 1 Medical treatment, along with surgical debridement, is often recommended. 3 We describe a rare case of SCJSA in a healthy adult.
Case report
A 58-year-old female with no previous medical or surgical history, presented to the emergency department with a 3-week history of progressive painful swelling of the right “shoulder.” She denied any history of trauma, intravenous drug abuse, or any predisposing factors for infections. Analgesic medication did not alleviate her symptoms. On physical examination, the patient’s vital signs were stable with a body temperature of 37.3°C, a heart rate of 90 beats per min, and a blood pressure of 130/80 mmHg. The patient had a warm, indurated mass overlying the right SCJ. The rest of the physical examination had found no abnormalities. Mobility of the right shoulder joint was not restricted. She underwent a blood workup that showed a white blood cell count of 7000/μL and a C-reactive protein level slightly raised at 4.5 mg/dL. The initial chest X-ray revealed no abnormalities.
Computed tomography (CT) of the chest with intravenous (IV) contrast agent was performed. It showed erosion of the sternal end of the clavicle and the manubrium sternum associated with thickening of the synovium and a SCJ space narrowing, suggestive of an infective process. No extensive abscess to the chest wall or retrosternal signs of mediastinitis were noted (Figure 1). The contralateral SCJ was normal. At this stage, she was referred to the orthopedic surgery department of our institution.
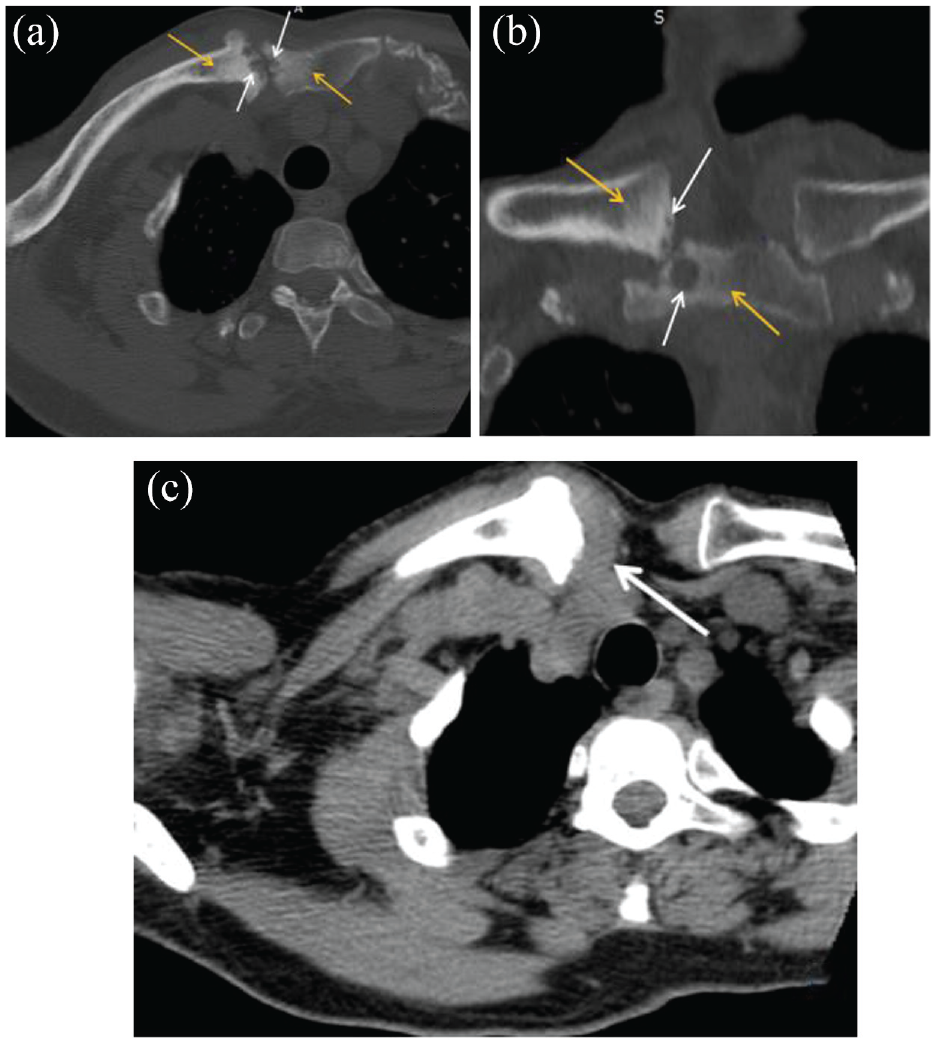
CT scan of the right sternoclavicular joint in axial (a) and coronal (b) sections with bone window study showing pinching of the SCJ space with cortical erosions, subchondral geodes (white arrows) and osteocondensation with blurred boundaries (yellow arrows). CT scan of the right sternoclavicular joint in axial (c) section with soft tissue window study showing thickening of the synovium (arrow).
The patient was taken to the operating room. Under general anesthesia, the procedure was done by two orthopedic surgeons. A 4-cm incision starting horizontally over the proximal 1/3 of the clavicle and then curved vertically along the left border of the sternum was made. As soon as the joint space was opened, a purulent collection, extending both over the clavicle and the sternum, was drained. Limited destruction of small parts of the SCJ was noted (Figure 2). Simple debridement and limited curettage were preferred to en bloc resection given the limited size of necrotic tissues (Figure 3). A suction drain was placed in the space created following the excision of the SCJ. A specimen was sent through for microscopy, culture, sensitivity, and histology.

(a and b) Photos showing pre-operative aspect: swelling near the right sternoclavicular joint. (c) Pre-operative photo in the operating room showing the incision which was performed. (d) Photo showing operative findings including partial necrosis to the SCJ (arrow).

Photos (a and b) showing clinical aspects after partial debridement was performed. Photo (c) showing synovium of the SCJ taken for anatomopathological examination.
Postoperatively, empiric IV antibiotics were prescribed, consisting of an association of amoxicillin and clavulanic acid with gentamycin for 5 days.
Bacteriological laboratory findings from the specimen taken revealed a high count of altered leucocytes. However, cultures from operative wounds and blood samples yielded no growth. Histological examination did not find any signs of malignancies or specific infections such as tuberculosis. The findings however were in favor of a septic origin.
In the absence of a causing organism on cultures, many other etiologies of non-infectious mono-arthritis should be considered as differential diagnosis. However, intra-operative findings as well as histological appearance were highly suggestive of septic arthritis.
On day eight postoperative, the surgical wound examination revealed no signs of infection, and the suction drain was removed. Body temperature was normal. White blood cell count was 6600/μL, and C-reactive protein level was 8.5 mg/dL. The patient was discharged on oral antibiotics (amoxicillin/clavulanic acid) for 8 weeks to prevent any relapse.
During her last visit to the outpatient clinic, 18 months postoperatively, the patient had no signs of infection, full range of shoulder motion, and excellent function of her arm. The aesthetic outcome was judged satisfactory by the patient (Figure 4). X-ray examination of the right SCJ was completely normal (Figure 5).

Clinical and aesthetic outcome at the latest follow-up 18 months postoperatively.

Radiographs of the right claviculae at the latest follow-up 18 months postoperatively.
Discussion
SCJSA is an uncommon disease and accounts approximately for 0.5% to 1% of all joint infections.2,4 It is mostly found in patients with underlying diseases.2,5 As in the present case, isolated cases of SCJSA have been described in healthy adults.1,6 The pathogenesis of SCJSA is not well understood, but it appears to result from either hematogenous or contiguous spread. 2 SCJSA is unilateral in almost all the reported cases, 2 affecting mainly the right side. 6 Clinical presentation is often sudden/insidious, and patients might complain for days to months of spontaneous pain in the shoulder, neck, or chest, with limited motion of the upper extremities, and associated fever.1,2,4 Joint swelling and erythema might also occur.1,2,4
There are no definite criteria for diagnosing SCJSA. The diagnosis is based on a thorough history, physical examination, laboratory workup, imaging modalities, and arthrocentesis if possible. 7 A CT scan of the chest is recommended as the initial imaging study. Its findings include joint effusion, joint space narrowing, irregular joint surface, subchondral bone erosion, soft tissue swelling, and gas bubbles in the joint.2,4 MRI also gives excellent imaging information. 4 Unfortunately, this examination was not available in our setting. SCJSA can be accompanied by a loco-regional extension of the abscess. The most serious complication is mediastinitis, which occurs in less than 15% of cases.2,8
Staphylococcus aureus is the most commonly isolated microorganism in patients with SCJSA. Other microbial pathogens have also been reported such as β hemolytic streptococci, Streptococcus pneumoniae, Pseudomonas aeruginosa, Brucella species, and other gram-negative bacilli. 2 However, in 30% of cases, the causative pathogen could not be identified, 4 as is the case in our patient. When the bacteriological investigation is negative and in the case of a non-nosocomial infection, empiric antibiotic regimen targeting methicillin-sensitive Streptococcus aureus should be carried on. 1 Other antibiotics such as vancomycin should be used in the case a methicillin-resistant S. aureus is suspected. 9 In our case, the antibiotic choice was explained by the fact that the patient has no history of hospital stay or risk factors of nosocomial infection.
The duration of antibiotic treatment in SCJSA is controversial with some authors advocating long courses reaching 52 days in some reports. 2 While surgical intervention alongside appropriate antibiotic therapy is the gold standard of treatment, 2 there have been several cases of confirmed SCJSA treated with antibiotics alone.4,10 In our patient, because SCJ infection was limited to a small area, partial debridement was performed instead of complete resection. 6
Conclusion
SCJ septic arthritis is a condition with significant morbidity and potential mortality. All medical practitioners must maintain a high degree of suspicion, even in healthy patient, as it can lead to serious complications.
Footnotes
Acknowledgements
The authors would like to thank Ms Slim Jerbi and Ms Mohamed Gannar for their kind assistance in the elaboration of this article.
Credit authorship contribution statement
All the authors participated in the design, performance, analysis, and drafting of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.