
Abstract
Instability arthropathy of the sternoclavicular joint is most commonly managed by rehabilitation, injection, and either arthroscopic or open debridement with or without interposition arthroplasty. When these options fail to achieve symptom relief, excision arthroplasty is an option. This is associated with a risk of persistent instability and incomplete pain relief. We describe two cases in which custom sternoclavicular joint replacement was performed for painful insufficiency of scapular suspension. Although the prostheses remained secure in both cases, the first case was complicated by persistent instability due to insufficient reconstruction of the intrinsic sternoclavicular capsular ligaments. This was recognised and corrected for in the second case, in which stability of the sternoclavicular joint replacement has been noted on more than a 5-year review. We conclude that sternoclavicular joint replacement is an option for patients in whom instability arthropathy remains an intrusive problem in daily life after other conventional treatments have not controlled symptoms. Stability of the joint remains a concern. We offer one method of achieving stability through an iterative design process including the ability to reconstruct the intrinsic capsular ligaments around the articulation.
Introduction
Traumatic and atraumatic instability of the sternoclavicular joint (SCJ) may be successfully managed, when indicated by intrusive symptoms, by a combination of rehabilitation, 1 nonsurgical intervention for pain1,2 and surgery.3–10 Arthritis of the SCJ is relatively rare, 11 more often developing spontaneously in late middle-aged females 12 and after trauma if subluxation persists or recurs,13,14 particularly if there is articular or periarticular fracture.2,13,14
The intrinsic (capsular) sternoclavicular ligaments and intraarticular disc, and extrinsic (costoclavicular) ligaments provide constraints to excessive motion at the SCJ.15,16 The internal (sternothyroid and sternohyoid) and external (sternocleidomastoid [SCM] and pectoralis major) muscular layers embrace the SCJ posteriorly and anteriorly, respectively. The pectoralis major has an attachment to, and, therefore, may reinforce, the inferoanterior capsule, but the superior and posterior capsule is not similarly protected, allowing for greater SCJ motion in the coronal plane than the axial and sagittal planes. SCJ motion is determined by the fulcrum of the costoclavicular ligament (CCL),15,16 a robust bilaminar obliquely placed ligament between the under surface of the medial clavicle and the upper surface of the first rib and its cartilage, being contiguous with the attachment of the subclavius laterally 17 and the capsules of the SCJ and first costosternal joints medially. It follows that disruption of the CCL is possibly the most important factor in permitting persistent SCJ instability15,16,17: high energy lateral compression trauma of the shoulder girdle may be associated with greater likelihood of persistent SCJ instability.
Fractures of the medial clavicle medial to, or through, the CCL cause a dissociation between the shoulder girdle and the axial skeleton and consequent shoulder girdle dysfunction. 18 In a comparable manner, loss of clavicular bone medial to or through the region of attachment of the CCL will lead to a dissociation of the shoulder girdle and the axial skeleton. The combination of SCJ instability and loss of bone continuity (fracture or bone loss for other reasons), therefore, comprises a challenge to upper extremity function. 18 Reconstruction for stability should, therefore, consider both the intrinsic SCJ capsular ligaments and the extrinsic CCL. The intrinsic ligaments may be repaired, 19 reinforced with autogenous local SCM tendon graft,9,20 distant autogenous tendon grafts, 16 allografts 21 or synthetic material. 22 The extrinsic (CCL) ligaments may be repaired 23 or replaced with distant autogenous or allogeneic 24 grafts, or synthetic material. 25 Trans-articular wires,26,27 buttressing plates 28 and plate-based fusion7,29 have also been advocated for the treatment of SCJ instability, but have been associated with high rates of failure26,27 and complications.30,31 Excision arthroplasty5,8 with intrinsic capsular imbrication does not resolve axial instability, particularly when there is disruption of the CCL: the loss of the articulation limits the effectiveness (load-sharing) of scapular protraction and retraction, and, therefore, is not advocated for young patients, being indicated for late onset osteoarthritis of the SCJ. 8 If medial bone loss has occurred, the restoration of clavicular length with autogenous or allogeneic grafts without replacement of the SCJ 32 has the same limitations as excision arthroplasty.
Patient-specific SCJ replacement arthroplasty (SCJR) has been reported in one patient who had previously had a partial excision arthroplasty of the medial clavicle, medial to (and, therefore, not disrupting) the CCL. 10 Although anteroinferior instability occurred early in the postoperative period, both components were noted to be securely fixed in bone at the subsequent revision, and a simple soft tissue repair sufficed to restore stability to the SCJR with good pain relief and a durable functional outcome. Other, nonanatomical, hemiarthroplasty solutions utilising off-label use of implants have been reported. 33 There is, therefore, no existing solution for medial clavicular bone loss involving the SCJ if the objective is to reconstruct a load-sharing articulation, particularly after previous surgery in which varying loss of intrinsic and extrinsic ligaments has occurred.
The purpose of this report is to describe the surgical treatment of two patients in whom patient-specific custom-manufactured SCJR arthroplasties were used. In one extensive medial clavicular bone loss occurred as a result of excision of the SCJ for painful instability arthropathy with multiple revision procedures; in the other, severe instability arthropathy of the SCJ was associated with painful medial clavicular radiation osteonecrosis, requiring extensive excision of the bone for pain relief.
Case presentation 1
A 50-year-old male patient (comorbid status American Society of Anesthesiologists [ASA] grade 3) with a nonmanual profession sustained a fracture dislocation of the dominant SCJ with medial clavicular fracture, for which operative intervention had been performed at another institution. The patient had poorly controlled insulin-dependent diabetes mellitus, hypertension and high body mass index without peripheral extremity vascular disease. The fracture failed to heal, and the persistent nonunion had been managed by a total of nine further procedures (including transosseous carbon fibre tape fixation with bone grafting, further bone grafting, and autologous hamstring grafting), two of which were complicated by ipsilateral pneumothoraces. Eventually, excision of the sternal end of the medial clavicle was performed with the resection margin lateral to the CCLs. This resulted in scapular ptosis, medial (venous) thoracic outlet syndrome (there was no clinical evidence of a proximal arterial obstruction or compression on provocative testing) with venous engorgement across the front of the chest, neuropathic arm pain and no useful active unassisted arm function above waist level. There was malunion of the residual medial clavicle through a previous transclavicular graft tunnel, and heterotopic ossification between the medial extent of the remaining clavicle and the first rib and sternum with a distal pseudarthrosis, causing the persistent scapular ptosis (Figure 1). Computerised tomography (CT) of the upper chest and both clavicles was undertaken, and the clavicular bone loss measured relative to the intact clavicle. The medial clavicle bone loss measured 78 mm (54% of the estimated intact clavicle length). In the absence of arterial compromise, vascular imaging was not performed.
Case 1. (a) Anteroposterior and (b) Zanca preoperative radiographs showing right clavicular mal- union, bone loss of the medial clavicle, surrounding heterotopic ossification and sterno-osseous pseudarthrosis. The scapula is protracted and in a fixed lateral displacement.
At surgery, the periclavicular soft tissue envelope containing residua of the previous ligament augmentation devices was dissected off the supraclavicular brachial plexus. The anterior muscles (SCM and pectoralis major) were dissected free from the distorted scar, and heterotopic bone was excised. There were no definable costoclavicular or sternoclavicular ligaments. After exposing the periclavicular space and releasing the medial end of the remaining clavicle, the scapula could be restored to a symmetrical posture when compared with the normal shoulder girdle. A custom cemented medial clavicle replacement with a hydroxyapatite-coated rough collar region (Stanmore Implants Worldwide, Elstree, London, United Kingdom) was implanted (Figure 2). The medial end of the clavicular prosthesis was perforated to facilitate reconstruction of the extrinsic CCL using a SCM tendon sling to stabilise the ‘head’ of the clavicle as described previously. 4 The custom metallic sternal tray (Stanmore Implants Worldwide, Elstree, London, United Kingdom) was fixed with two 3.5 mm interlaminar cortical screws into the cancellous bone of the manubrium sterni (Figure 2), and the ultra high molecular weight polyethylene liner was cemented into the tray. There was no tissue that resembled the intrinsic capsular ligaments of the SCJ, and reconstruction was not performed. In the supine position, the prostheses appeared to remain located during ranging motion of the arm below shoulder level while avoiding cross-body adduction and any internal rotation in elevation at 45° in the scapular plane. A full-body thoracobrachial cast was applied to limit motion of the arm to the same range. The clavicular component dislocated antero-medially in the first postoperative week when the patient sat up unassisted. The patient’s unstable medical comorbidities precluded revision from being undertaken until 7 months later. A shorter clavicular prosthesis was manufactured to reduce excessive tension within the healed medial periprosthetic tissues. An Achilles tendon allograft was utilised to reconstruct the recurrently insufficient CCL. The superomedial attachment of the pectoralis major was transposed further superiorly to cover the anterior aspect of the SCJR in an attempt to provide greater stability. A thoracobrachial spica was reapplied postoperatively for a further 6-week period. Shortly after removing the spica, a further dislocation occurred.

Case 1. Implant design. A custom cemented medial clavicle replacement with a hydroxyapatite-coated rough collar region (Stanmore Implants Worldwide, Elstree, London, United Kingdom). The custom metallic sternal tray (Stanmore Implants Worldwide, Elstree, London, United Kingdom) was fixed with two 3.5 mm interlaminar cortical screws into the cancellous bone of the manubrium sterni, and the UHMWPE liner was cemented into the tray.
At subsequent revision surgery, it was apparent that there had been rupture of the allograft. Attempted stabilisation of the SCJR using a polyurethane mesh (Artelon, Lavendar Medical, United Kingdom) to create a new SCJ ‘capsule’ was subsequently undertaken, following the successful outcome of the second SCJR. Despite the use of a thoracobrachial spica, radiographs at 6 weeks showed anterior subluxation of the medial end of the clavicle and, after discussion with the patient, it was decided not to intervene further. Two years after the most recent intervention, the Disability of the Arm, Shoulder and Hand (DASH) score 34 was 71.7, and the patient had movement sufficient only for personal care activities at waist level.
Case presentation 2
A 76-year-old female patient (comorbid status ASA grade 2) presented with painful osteonecrosis of the medial clavicle with destructive arthritis of the nondominant SCJ caused by radiotherapy used as adjuvant therapy for breast cancer many years previously. The patient was independent, self-caring and living in her own home with family assistance. Motion of the upper extremity was severely restricted by medial clavicular, pectoral and scapulothoracic pain, and a sling was used for comfort and support. There was a suspected pathological fracture of the left clavicle, which had been managed conservatively and CT confirmed a chronic nonunion of the clavicle without evidence of recurrent malignancy. There was no clinical evidence for irradiation brachial plexus neuritis. There was no impairment of distal upper extremity perfusion. Vascular imaging was not considered necessary, and the arm could not be moved to a provocative position for ultrasonography to be of value in the diagnosis of potential vascular thoracic outlet obstruction. The treatment options were discussed and included continuation of nonoperative management, excision of the medial clavicle with excision arthroplasty of the SCJ, augmentation of the medial clavicle with bone graft and plate osteosynthesis, or replacement using a custom SCJR. The persistent painful dysfunction of the forequarter, extensive medial clavicular bone necrosis and persistent nonunion, destruction of the SCJ, and poor local tissue nutrition following radiotherapy favoured SCJR over bone grafting whether this was free-vascularised, pedicled or nonvascularised. An implant, based on that used in the former case, was designed with the addition of perforations in the sternal metal tray to facilitate the attachment of a polyurethane mesh hood (Artelon, Lavendar Medical, United Kingdom) posteriorly, medially and anteriorly to reconstruct the intrinsic capsular ligaments for improved stability (Figure 3). The resection of the medial clavicle was designed to ensure that the implant was cemented into bone of optimal quality while not resecting lateral to the isthmus of the clavicle, which would make intramedullary canalisation more difficult, particularly in osteonecrotic bone. The medial clavicular bone loss segment was measured at 55 mm, giving a ratio of resection (measured resection length: total estimated clavicular length) of 40%. The techniques of fixation of the clavicular and sternal components were the same as those used in the first case. The SCM tendon was used to reconstruct a CCL. Sutures were passed through the sternal tray, and the mesh brought up to the posterior aspect of the tray prior to cementation of the liner. After tensioning the SCM tendon transfer, the mesh hood was brought superiorly and then sutured to the anterior aspect of the sternal tray using the same sutures previously passed for the posterior leaf of the hood. By alternately adjusting the tension in both SCM tendon and the mesh hood articulation and mobility of the prostheses could be balanced against laxity. The pectoralis major was advanced in the same manner as the first case and the cleidomastoid part of the SCM brought anteriorly over the advanced pectoralis major, to provide a muscular buttress, both to contribute to stability and to provide a robust anterior soft tissue cover. The platysma layer was also closed meticulously to ensure optimal quality soft tissues anterior to the implant. A simple sling was used for support in the postoperative period until wound healing. Scapular postural exercises were commenced, limited by discomfort at the SCJR and guided by observation of the limits of laxity of the new joint. Activation of the pectoralis major was avoided by limiting active forward elevation to ‘gravity-eliminated’ motion across the surface of a table. The limitations imposed by ipsilateral early cuff tear arthropathy were initially helpful in reducing the active range of motion during daily life activities.

Case 2. (a) Three-dimensional reconstruction of the preoperative CT images showing osteonecrosis of the medial end of the left clavicle, loss of the normal SCJ articular surfaces with deformity, and axial rotation of the clavicle at the nonunion site; (b) Implant design. The medial spherical ‘head’ was of smaller dimension than in the first case. Perforations were designed in the clavicle implant to facilitate reconstruction of both the intrinsic and extrinsic ligaments. The prosthesis was coated with hydroxyapatite to facilitate soft tissue (muscle) adherence; (c) Detail of the sternal tray and liner: note the perforations in the tray for the attachment of the polyurethane mesh hood (neo-‘capsule’). These facilitated attachment of remaining capsular tissue and reinforcement with the mesh hood. The sternal tray was press-fit into the instrumented sternal resection and fixed with intralaminar manubrial 3.5 mm cortical screws.
The wound healed primarily, and the patient was pain-free 6 weeks after surgery. The SCJR was congruent with no signs of early loosening or abnormal displacement. Healing of the SCJR capsule was considered sufficient at the 3-month review, and active unassisted activities of daily living were encouraged within the limits of discomfort. The patient did not require formal physiotherapeutic guidance thereafter. Six months following surgery, the patient was able to actively flex to 80° and abduct to 70° without pain or instability of the implants. At the 2-year clinical review, the SCJR remained pain-free and stable. The DASH score was estimated at 73.3. There were no wound-related problems and no clinical evidence of periprosthetic infection. Radiographs showed no concerns regarding the sternal prosthesis while there was a 2 mm lucent zone at the tip of the clavicular prosthesis the significance of which was uncertain (Figure 4). This had not progressed at a 5-year clinical review, at which time the patient had progressive cuff tear arthropathy in the ipsilateral shoulder joint for which prosthetic replacement was planned.

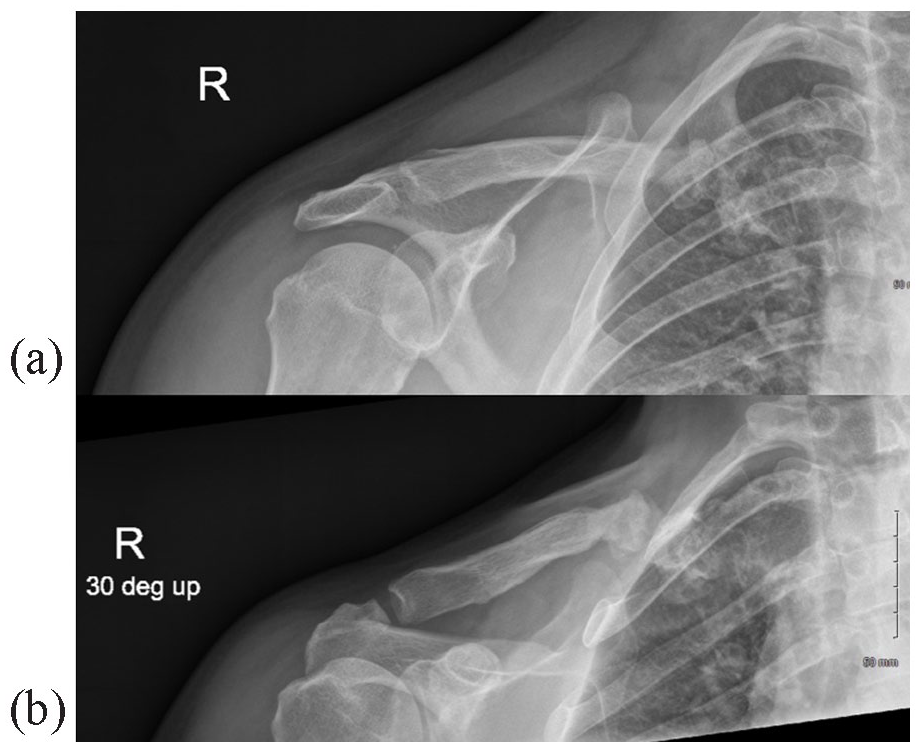
Case 2. Anteroposterior (a) and Zanca (b) radiographic views at the 6-month postoperative review. Both prostheses remain secure, and the SCJ remains enlocated 2 years after implantation.
Discussion
In the cases described in this report, the magnitude of medial clavicular bone loss and absence of both intrinsic and extrinsic SCJ stabilising ligaments (in the first case after previous interventions and in the second case after debridement of necrotic bone with chronic nonunion of a pathological fracture) precluded the use of conventional operative strategies for instability arthropathy of the SCJ.3–10 While repair or reconstruction of the extrinsic (CCL) ligament was important for the restoration of a fulcrum for clavicular motion at the SCJ, it became equally clear that restoration of the intrinsic (capsular) ligaments was critical for SCJR stability. The persistent postoperative instability present in the first case demonstrated the importance of the reconstruction of the periarticular capsular ligaments for SCJR stability. Having recognised this, reconstruction of the intrinsic capsular ligaments using an encapsulating mesh which facilitated secondary fibrogenesis to form an ‘intrinsic SCJ pseudocapsule’ restored SCJ stability in the second case over a medium term review of 5 years. The stability of this augmented construct was preserved, and the clinical outcome for the SCJR was clearly superior to that gained in the index case. A similar early postoperative instability following custom SCJR was managed by local tissue mobilisation and reinforcement with nonabsorbable sutures. 10 In the first case described, there was insufficient soft tissue for local reconstruction of the intrinsic capsular ligaments, and the relevance of the reconstruction for stability was underestimated: it was anticipated that reconstruction of the medial part of the CCL by transfer of the SCM tendon would be sufficient. This proved not to be the case, and a different approach was conceptualised for the second case. These cases demonstrate the challenges and pitfalls of SCJR as a surgical solution for complex SCJ disease. Our experience highlights the importance of the reconstruction of the periarticular (intrinsic) ligaments to gain SCJR stability to the success of this rare procedure.
The indications for SCJR are rare. The role of SCJR may be to offer an alternative to excision arthroplasty for instability arthropathy in younger patients with limited physical requirements in whom the persistent instability that may attend the excision is undesirable, and in whom arthroscopic or open debridement with or without interposition arthroplasty has not proven beneficial. The challenge of stability, particularly in a case in which soft tissues are lacking, remains a concern. Reconstruction using a mesh hood attached to the implant to replace the intrinsic ligaments appears to be a reasonable option, and avoids adding the risks associated with transosseous sternal passage of sutures, anchors and tendon grafts.
Footnotes
Acknowledgements
K.W. is a Design Engineer at Stanmore Implants Worldwide, Elstree, London, UK. K.Z., PhD CEng MIMechE MEng is Implant Design Engineer at Stanmore Implants Worldwide, Elstree, London, UK
Author contribution
Sophia Burns – Author that wrote and revised article for publication.
Tanujan Thangarajah, – Author that critically reviewed article.
Simon Lambert – Primary surgeon involved in cases presented. Critically reviewed article and approved final article for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.