
Abstract
Segmental pressure and air plethysmography waveform (APW) analyses are widely used for noninvasive diagnosis of lower extremity peripheral arterial disease (PAD). The contribution of APW analysis to the diagnosis of PAD at the common femoral artery level or above (INFLOW) has been minimally assessed. This study examines APW characteristics in the thigh to determine which features best identify flow-limiting (>50% diameter) INFLOW disease. Nondiabetic vascular laboratory patients with segmental APW analysis, systolic pressure measurements, and arteriography within 30 days of their noninvasive vascular ultrasound procedure were included for study. Thigh plethysmographic waveforms were evaluated for acceleration time (TIME) from onset of systole to peak systole, relative amplitude reduction (RAR) one-fifth of a second after peak systole, and waveform downslope curvature (CURV). Patients with nonsignificant INFLOW disease were defined by thigh plethysmography waveforms with inward CURV regardless of TIME or with TIME <0.28 seconds and even CURV. Significant INFLOW disease was defined by TIME >0.28 seconds and outward or even CURV. Sensitivity for defining INFLOW disease was 94% (15/16) and specificity 81% (26/30); positive predictive value was 79% (15/19) and negative predictive value 96% (26/27). Thigh-level APW characteristics may improve identification of INFLOW disease in nondiabetic patients undergoing physiologic testing for lower extremity PAD.
Keywords
Segmental systolic pressure measurements and air plethysmography waveform (APW) analysis have been widely used for noninvasive diagnosis of lower extremity peripheral arterial disease (PAD). Physiologic testing has been shown to be a reliable method for the determination of normal arterial hemodynamics, demonstration of the presence of flow-limiting disease, and estimation of the extent of collateral circulation.1–5 Differentiating stenosis from occlusion and definition of the precise level of arterial disease, however, have proven to be more problematic. Physiologic assessment of arterial obstructions above the level of the common femoral artery (INFLOW) has been particularly challenging, especially in the presence of concomitant superficial femoral artery disease.1,3,5 While pressure protocols and criteria for defining INFLOW disease have been extensively investigated, the contribution of APW analysis to the evaluation of the severity of INFLOW disease at the present time is minimal. The purpose of this study was to examine APW characteristics at the level of the thigh cuff to determine which features best identify hemodynamically significant (>50% diameter) INFLOW disease.
Methods
The study group comprised of nondiabetic patients who underwent segmental systolic pressure measurements, APW analysis, and arteriography within 30 days of their noninvasive vascular laboratory examination. Patients with prior aortoiliac intervention were excluded from the analysis. Institutional review board approval for a retrospective review was obtained through our organization.
Systolic limb pressures and air plethysmographic waveforms were obtained with Unetixs Multilab 2-LHS and 2-CP physiologic testing equipment and 8- or 5-MHz bidirectional continuous wave (CW) Doppler transducers (Unetixs Vascular, North Kingstown, Rhode Island). Following 10 minutes of rest and with the patient lying in the supine position, systolic pressures were obtained at brachial, thigh, below-knee, and ankle (posterior tibial and dorsalis pedis) levels using appropriately sized blood pressure cuffs. Thigh pressures were obtained at the uppermost segment of the thigh using a 12 × 42–cm blood pressure cuff. Brachial, calf, and ankle bladder widths were dependent on limb girth and varied from 10 to 12 cm; all pressure cuff bladders were 42 cm in length. Upper thigh and below-knee (calf) pressure measurements were obtained using the Doppler signal at the ankle from the posterior tibial (PT) or dorsalis pedis (DP) artery, whichever had the highest systolic pressure. Thigh, calf, and ankle pressure indices referenced the higher of the two brachial pressure measurements.
Calibrated pulse volume recordings were employed to standardize the air volume within each cuff. Waveform gain varied between patients but was standardized for each patient at the thigh, calf, and ankle levels; chart recorder speed was 25 mm/s for all measurements. An upper thigh waveform felt to be most representative of the displayed waveform cycle was selected and evaluated in Microsoft PowerPoint (Microsoft, Redmond, Washington). Bitmap images of individual waveforms were enlarged to full screen so that the amplitude and timing pixels were noticeably visible. Microsoft PowerPoint drawing tools were used to aid in the completion of manual measurements of the following upper thigh waveform characteristics:
Acceleration time (TIME), in seconds, from the onset of systole to mid-peak systole and rounded off to the nearest whole division (1 mm, or 0.04 s) on the recording (Figure 1)
Relative amplitude reduction (RAR) expressed as a ratio: maximum peak systolic waveform amplitude measured from the onset of systole to mid-peak systole, minus the downslope waveform amplitude one-fifth of a second after mid-peak systole, divided by maximum peak systolic waveform amplitude and rounded off to the nearest whole number (Figure 2)
Downslope curvature (CURV) based on the direction of the dicrotic limb curvature in relationship to a reference line drawn from mid-peak systole to end diastole
Inward CURV—inward-directed deflection from the established reference line of 50% or greater (Figure 3A)
Even CURV—inward and/or outward deflection from the established reference line of less than 50% (Figure 3B)
Outward CURV—an outward deflection from the established reference line of 50% or greater (Figure 3C)
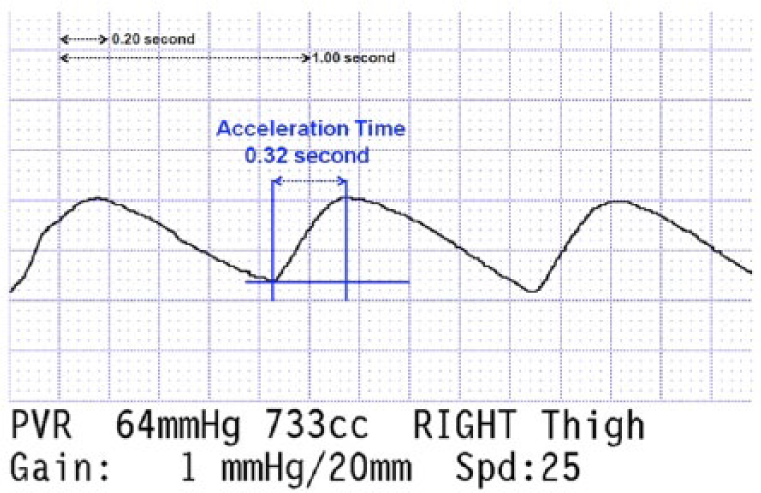
Thigh air plethysmographic waveform (APW) illustration demonstrating the calculation of acceleration time (TIME) in seconds.
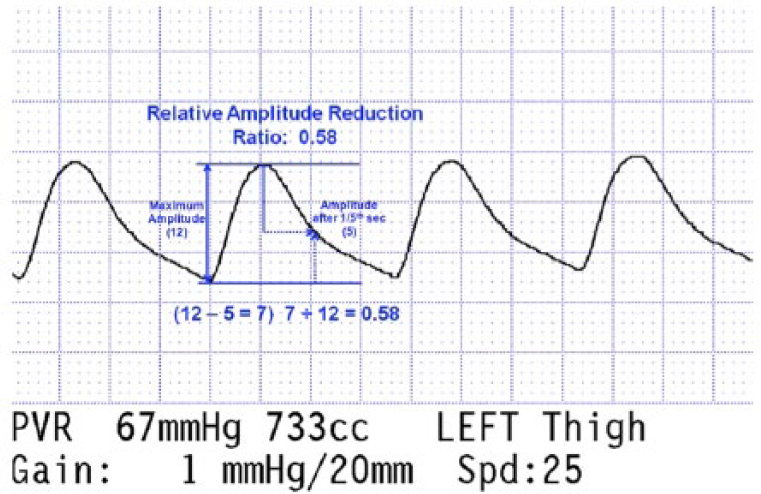
Thigh air plethysmographic waveform (APW) illustration demonstrating the calculation of relative amplitude reduction (RAR).
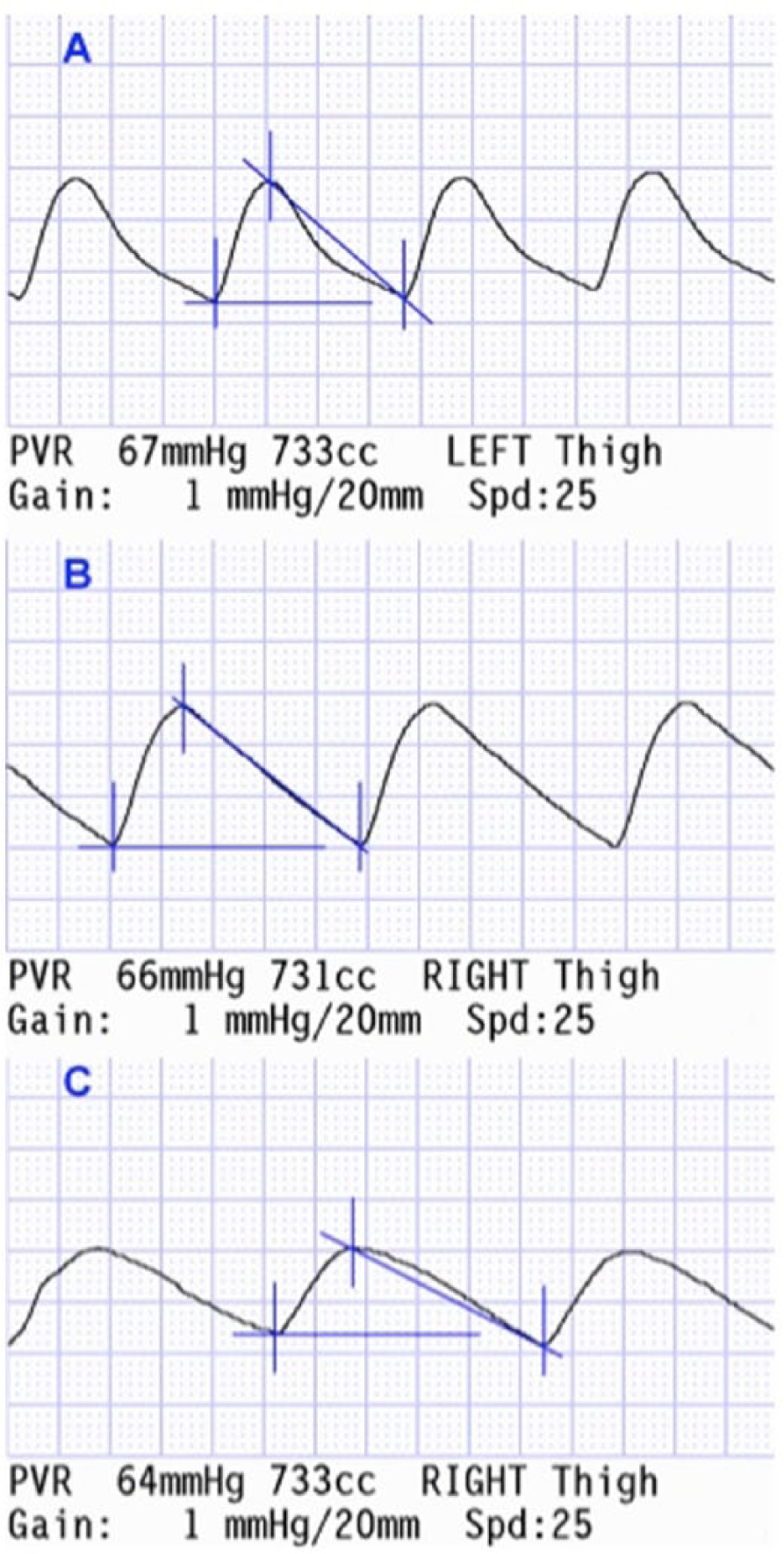
(A) Thigh air plethysmographic waveform (APW) illustrating an inward downslope curvature (CURV). (B) Thigh APW illustrating an even downslope curvature (CURV). (C) Thigh APW illustrating an outward downslope curvature (CURV).
Historically, normal plethysmographic waveforms have been characterized by a sharp systolic peak and prominent dicrotic wave; abnormal waveforms have an absent dicrotic wave, a downslope bowed away from the baseline, flattened systolic peaks, and an equal upslope and downslope time.1,3–10 These historic characteristics were the basis for the waveform elements outlined in this study. Acceleration TIME objectively defines waveform acceleration to within four hundredths of a second. Plethysmographic RAR was a secondary acceleration parameter developed to more clearly define the extent of waveform deceleration and corresponding waveform elongation in extremities with pressure-flow reducing lesions. (This plethysmographic relative amplitude reduction [RAR] should not to be confused with the renal duplex acronym for renal-aortic ratio.) Plethysmographic downslope curvature (CURV) was defined to attempt to more objectively define the historic observation that the downslope curvature bows inward following peak systole in normal extremities and outward (away) from the downslope during deceleration in abnormal extremities.
Bilateral waveform and pressure data were performed on all extremities in this study; however, only those extremities having arteriographic correlation were analyzed for the upper thigh waveform characteristics detailed above. Two physicians shared responsibility for interpreting the arteriograms and were blinded to the noninvasive data. Each limb was classified as negative or positive for hemodynamically significant INFLOW disease. Positive INFLOW disease was defined as greater than 50% diameter stenosis or occlusion in one or more of the following vessels: abdominal aorta, common iliac, external iliac, or common femoral artery.
Statistical analysis for waveform and pressure data was performed using SAS 9.2 (TS level 2M3, XP_PRO platform; SAS Institute, Cary, North Carolina). Descriptive statistics are expressed as mean ± standard deviation (SD). For all analyses, a P value of less than .05 was used to define statistical significance.
Results
A total of 30 patients were analyzed; 63% were male (19/30) and 37% female (11/30). The average age was 71 years (range, 43–91 years). There were 16 bilateral and 14 unilateral extremity evaluations that met inclusion criteria and had appropriate clinical indications. The indications for extremity evaluation were claudication (53%), limb ischemia (13%), rest pain (23%), and ulceration (10%).
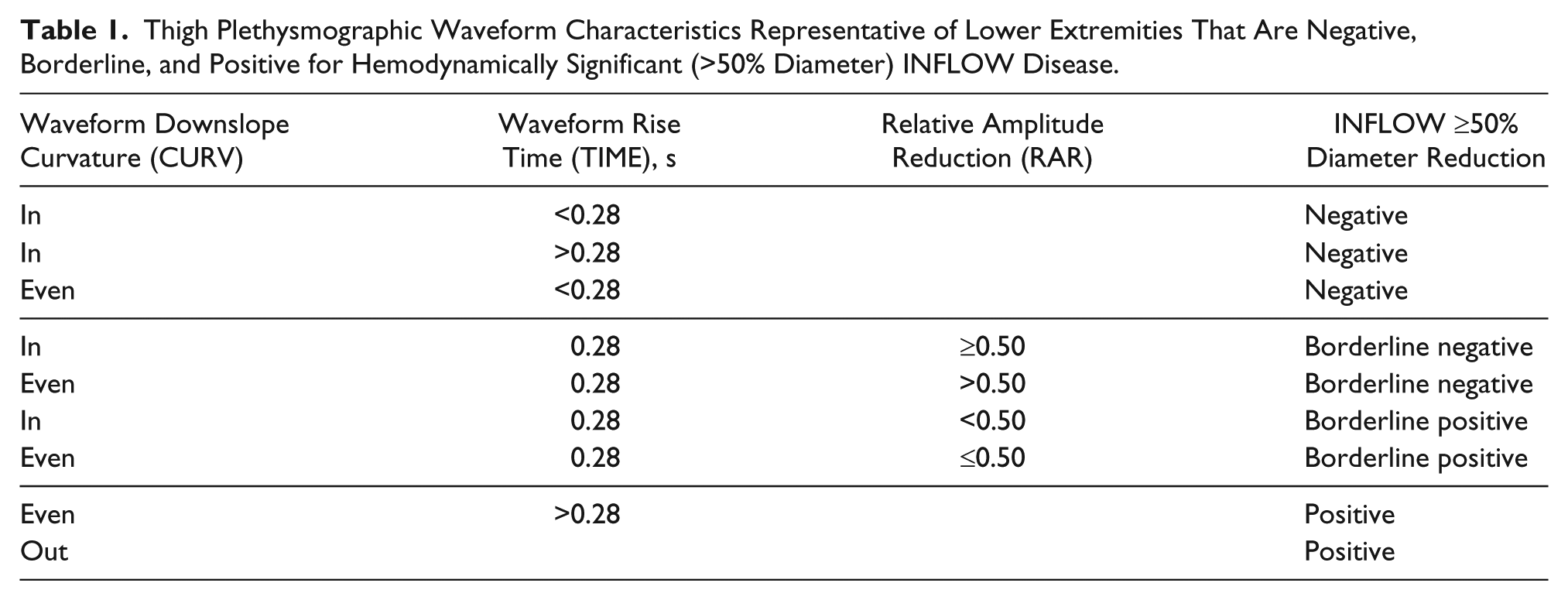
Forty-six extremities were investigated: 48% (22/46) right and 52% (24/46) left. The combined average of ankle brachial indices from all study extremities was 0.64. Average thigh waveform gain in all extremities was five (range, 3–12). Thigh waveform characteristics representative of plethysmographic examinations that were negative, borderline, and positive for hemodynamically significant (>50% diameter-reducing stenosis) INFLOW are summarized in Table 1.
Thigh Plethysmographic Waveform Characteristics Representative of Lower Extremities That Are Negative, Borderline, and Positive for Hemodynamically Significant (>50% Diameter) INFLOW Disease.
Thirty extremities (65%) were negative for INFLOW disease: one extremity with an insignificant (<50%) lesion, eight with single-level femoropopliteal (outflow) disease, five with tibioperoneal (runoff) disease, and 16 extremities with both femoropopliteal and tibioperoneal disease. The average systolic pressure difference between the brachial and upper thigh cuff was −13.63 ± 46 mm Hg. Mean thigh waveform amplitude was 16.43 ± 1.2 mm (divisions on the recording), TIME was 6.13 ± 1.2 divisions (24.52 ± 4.8 ms), and RAR was 0.48 ± 0.13. Percent waveform downslope CURVE was 63% (19/30) inward, 33% (10/30) even, and 3% (1/30) outward.
Sixteen extremities (35%) were positive for INFLOW disease: four extremities with single-level inflow lesions, three extremities with multilevel inflow and femoropopliteal disease, four extremities with multilevel inflow and tibioperoneal disease, and five extremities with multilevel inflow and femoropopliteal and tibioperoneal disease. The average systolic pressure difference between the brachial and upper thigh cuff was −24.19 ± 32.7 mm Hg. Mean thigh waveform amplitude was 10.38 ± 4.01 mm, TIME was 7.88 ± 1.02 divisions (31.52 ± 4.08 ms), and RAR was 0.39 ± 0.17. Percent waveform downslope CURVE was 25% (4/16) inward, 33% (8/16) even, and 25% (4/16) outward.
Normal arteries or insignificant INFLOW disease were defined by thigh air plethysmography waveforms with inward CURV, regardless of TIME, or by TIME <0.28 seconds and even CURV. Borderline INFLOW disease was defined with TIME equal to 0.28 seconds and inward or even CURV regardless of RAR. Significant INFLOW disease was defined with TIME >0.28 seconds and outward or even CURV. Using these criteria, sensitivity for defining INFLOW disease was 94% (15/16) and specificity 81% (26/30); positive predictive value (PPV) was 79% (15/19) and negative predictive value (NPV) 96% (26/27).
If borderline extremities were included in the negative INFLOW disease category, sensitivity would be 63% (10/16), specificity 97% (29/30), PPV 91% (10/11), and NPV 83% (29/35). The borderline negative interpretation value of TIME equal to 0.28 seconds, inward or even CURV, and RAR of greater than 0.50 allows flexibility to increase the NPV of the interpretation of INFLOW disease. If borderline extremities were included in the positive INFLOW disease category, sensitivity would be 94% (15/16), specificity 73% (22/30), PPV 65% (15/23), and NPV 96% (22/23). The borderline positive interpretation value of TIME equal to 0.28 seconds, inward or even CURV, and RAR of less than 0.50 allows flexibility to increase the PPV of the interpretation of INFLOW disease.
Discussion
The utilization of air plethysmography in the noninvasive physiologic evaluation of PAD has long been established.1,3–8 Inherent elements to this evaluation were segmental systolic blood pressures in conjunction with plethysmographic waveform analysis. While single-level arterial and segmental blood pressure measurements have been extensively investigated, plethysmographic waveform characterization, with the exception of amplitude, is largely subjective and based on pattern recognition.1,7,9,10
The focus of this study was objective plethysmographic waveform analysis because the diagnostic accuracy of plethysmographic waveform data excluding pressure data has rarely been reported. Rutherford et al 1 demonstrated waveform accuracy to be 97% in healthy patients, 70% in patients with aortoiliac disease, and 75% in patients with multilevel aortoiliac and superficial femoral artery disease. In patients with ≥50% aortoiliac stenosis, Barringer et al 3 described 72% accuracy at the inguinal crease using a modified femoral sensor cuff and 60% at the lower thigh cuff level when waveform amplitudes were 18 mm or less. Cox and Barnes 11 incorporated dual (narrow) thigh cuffs and reported 79% accuracy for the high thigh cuff waveform in the presence of a significant (>50%) stenosis or occlusion of the aortoiliac segment.
While thigh plethysmographic waveform amplitudes of 18 mm or less were used to characterize extremities with INFLOW disease in the Cox and Barnes 11 investigation, in our study, 63% of the extremities without INFLOW disease had thigh waveform amplitudes that were 18 mm or less. In the Barringer et al 3 study, every thigh waveform without a dicrotic notch was positive for INFLOW disease; in our investigation, 67% of extremities negative for INFLOW disease had no discernible dicrotic notch. In 1969, Strandness 12 characterized “mildly abnormal” plethysmographic waveforms with downslope curvatures that bowed away from the baseline. In this investigation, only one patient with insignificant (<50%) INFLOW disease had a downslope curvature bowed away from the baseline; 33% had an even curvature that did not completely bend inward (toward) or outward (away) from the downslope of the waveforms, and most (63%) patients with insignificant INFLOW disease had a downslope curvature that was directed inward.
The limited, subjective, and dated nature of the historic plethysmographic waveform research makes a comparative analysis to our study largely speculative. While the technique of plethysmographic waveform acquisition is standardized, equipment used in most research devoted to this subject is markedly different from the devices in use today. In addition, the average American adult is more than 24 pounds heavier today than in 1960; adult obesity has increased from 15% in the mid-1970s to 36% in 2009. 13 Obesity and edema will attenuate the plethysmographic waveform; other common clinical factors that affect the waveform include stroke volume, blood pressure, vasomotor tone, blood volume, and the position of the limb. Finally, the relatively objective nature of the measurements performed in this study are compared with historic waveform characterizations based on text descriptions or drawings and not on actual plethysmographic recordings.1,12 One of the most commonly cited plethysmographic waveform references defines moderately and severely abnormal waveforms with upslope and downslope acceleration times that are nearly equal. 12 This reference has widespread acceptance despite contradictory abnormal plethysmographic recordings with deceleration times that appear nearly double the acceleration phase.10,14,15 Differences in equipment, patient physical characteristics, and variations in APW characterization and measurement methodologies, therefore, make it difficult to determine the degree to which our results differ from previous investigations.
Pressures and pressure indices at multiple levels in the thigh also have been employed to better differentiate inflow from femoropopliteal disease, with varying degrees of success.1–8,16 Accurate pressure measurements require the cuff bladder to be 20% wider than the diameter of the limb. 16 Cuffs that are narrower or wider than this parameter cause erroneously high and low pressure measurements, respectively, and this effect is commonly referred to as cuff artifact. In lower extremity segmental pressure measurement protocols that use two thigh cuffs, the highest thigh cuff should have a systolic pressure measurement 20 to 30 mm Hg higher than the brachial pressure for a normal study.1,16 Thigh pressure data from this study validate previous observations concerning the questionable clinical utility of segmental pressure measurements in the lower extremity. 17 In this investigation, which used a narrow high thigh cuff, extremities negative for INFLOW disease had an average thigh systolic pressure that was 14 mm Hg less than the highest brachial pressure. Similarly, in a larger patient cohort, thigh cuff pressure measurements averaged 12 mm Hg less than the highest brachial systolic cuff pressure. 18
In contrast to the technical issues with segmental pressure measurements, CW Doppler waveform acquisition, 19 and the current controversy with arterial Doppler waveform interpretation, 20 objective waveform classification with plethysmography devices has considerable potential. Computerized plethysmographic devices have the benefit of more precisely standardizing the waveform acquisition process, and plethysmographic devices are less dependent on the technical expertise of the operator. Computer-guided software algorithms could more precisely address the measurement and interpretive scenarios outlined in this study, with the flexibility to be modified to address postintervention scenarios such as bypass grafts, stents, and comorbidities such as diabetes.
In conclusion, this study substantiates and questions qualitative plethysmographic waveform characteristics reported in previous investigations. We believe thigh-level APW characteristics developed in this study may improve identification of INFLOW disease in nondiabetic patients. Greater investigation into this methodology may help reduce the subjectivity inherent to current APW analysis. More important, it may serve as a foundation for standardizing plethysmographic waveform characterization for the evaluation of lower extremity peripheral arterial disease. Until objective APW analysis has been more intensively investigated, however, it should be considered complementary to established air plethysmographic segmental pressure and waveform criteria for the determination of INFLOW disease.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.