
Abstract
There is little description of the Wallstent to treat infrapopliteal arterial disease. This may be a viable option due to its high conformability and ability to elongate in vessels of varying diameters. This case report highlights its use in this clinical situation.
Introduction
Treatment of infrapopliteal arterial disease with endovascular therapy can be challenging, especially if the disease extends from the popliteal artery into the tibial vessels. The challenge occurs if the intervention requires stent placement because of the varying diameters between the tibial vessels and popliteal artery. This is especially true if the disease involves the distal anastomosis of a bypass graft as the graft is usually of a larger diameter. This case describes the use of a carotid Wallstent to treat this type of disease and takes advantage of the elongation that occurs with the stent when placed in a smaller diameter vessel.
Case report
The patient is a 53-year-old male who has a history of a left femoral-popliteal bypass for trauma. He subsequently underwent treatment for a stenosis at the distal anastomosis and popliteal artery. He presented with critical ischemia of the left leg, and a duplex ultrasound revealed significantly elevated velocities in the popliteal artery which prompted an angiogram to be performed. The angiogram showed a patent bypass with a popliteal artery stent with severe neointimal hyperplasia extending into the tibioperoneal trunk and compromising flow into his single posterior tibial artery run-off (Figure 1). Due to the significant stenosis that was still present post-angioplasty and the varying diameters of the posterior tibial, popliteal, and bypass graft, the decision was made to use a 6 mm diameter by 22 mm length Carotid Wallstent from Boston Scientific. The patient was systemically heparinized, and via a 6 French sheath from right femoral access, the stent was placed and then angioplasty was performed within the stent. A completion angiogram showed no residual stenosis with excellent size matching to the posterior tibial artery (Figure 2). Post-intervention, the patient was seen in follow-up with an improvement in the ankle-brachial index from 0.51 to 0.87 as well as an improvement in the Rutherford category from 4 to 1. The duration of follow-up has been 1 year with a stable clinical exam and palpable posterior tibial artery pulse.
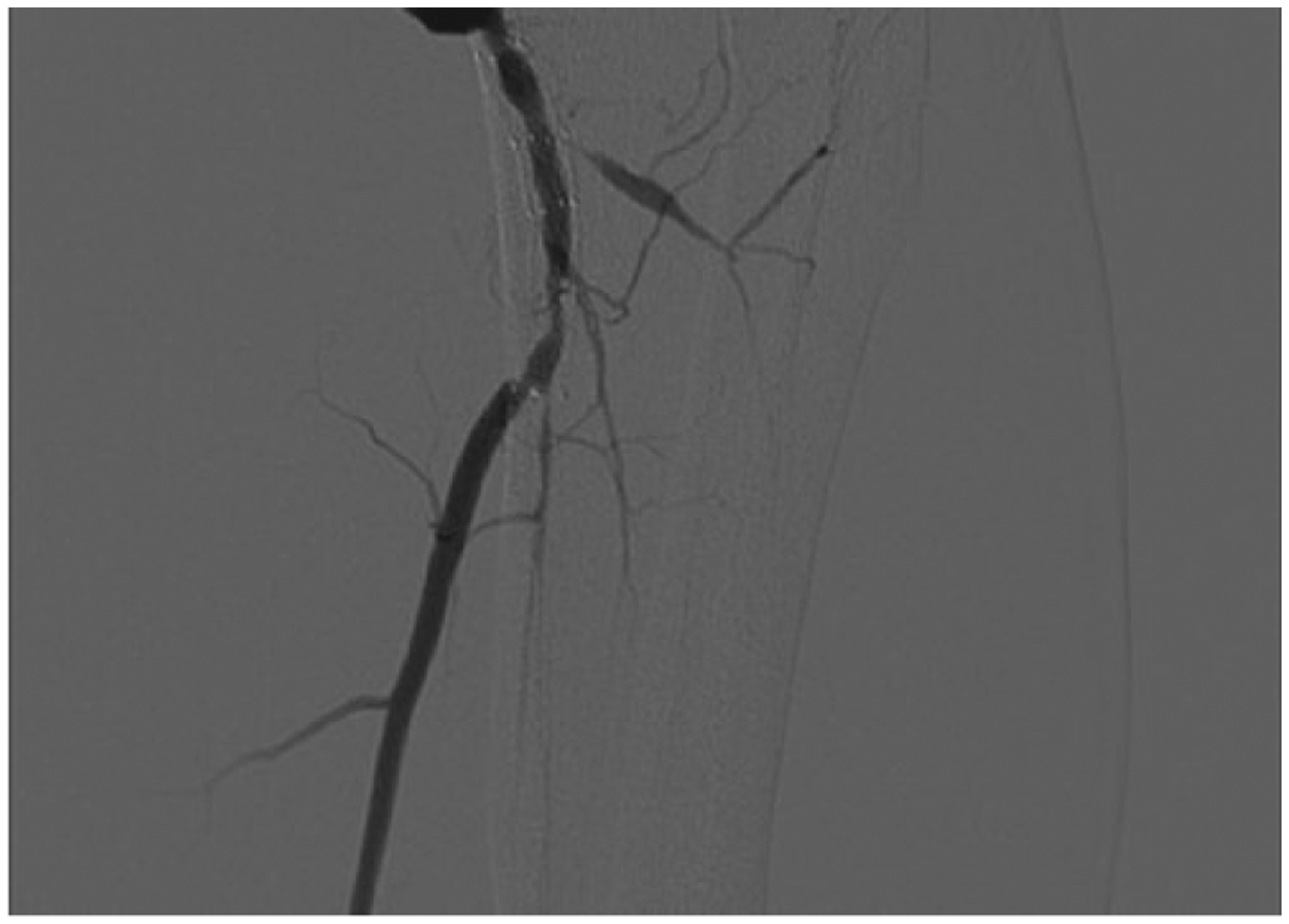
Significant in-stent restenosis distal to femoral-popliteal bypass graft compromising outflow through single posterior tibial artery run-off.

Completion angiogram after placement of Wallstent with no residual stenosis.
Rutgers Robert Wood Johnson Medical School does not require ethics approval for individual case reports. Written consent was obtained from the patient to publish radiographic images and describe this endovascular procedure.
Discussion
Neointimal hyperplasia is a risk after femoral-popliteal bypass grafting and usually occurs at the distal anastomosis. Treatment of this with endovascular therapy can result in recurrent stenosis that now involves the popliteal artery and may extend to involve the tibial vessels.
Diseased tibial arteries have been shown to have early recoil post-angioplasty.1,2 Also, to reduce the possibility of dissection in a tibial vessel, stent placement has been shown to be effective. Stenting for either dissection or recoil post-angioplasty has been shown to be safe and effective, with primary patency of >90% on short-term follow-up (3 months to 1 year).3–7
The Wallstent can be considered when dealing with disease that extends between vessels of different diameters especially if a dissection occurs post-angioplasty. The Wallstent has excellent patency rates in the carotid artery. 8 It is designed to work with the change in diameter between the internal carotid and common carotid arteries and is sized based on the common carotid artery diameter.
The advantage of the wall stent is the closed cell design which provides scaffolding for optimal lesion coverage. It is highly flexible and radiopaque with the ability to elongate when placed in a smaller diameter vessel which makes it ideal for treatment of popliteal disease which extends into a tibial artery as long as the tibial artery is of a larger diameter. In this particular case, the patient’s posterior tibial artery was 4 mm. The radial force of the Wallstent is known to be lower which allows its flexibility therefore post-dilation will be needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.