
Abstract
The current standard of care for the treatment of flow-limiting calcific iliac artery disease is balloon angioplasty and subsequent stent placement. However, the presence of calcified lesions may prevent adequate stent expansion or impede the delivery of large bore devices, such as those for transcatheter aortic valve replacement or endovascular aneurysm repair implants. Plaque modification through vessel preparation with orbital atherectomy may enable stent expansion and subsequent proper large device delivery with low rates of procedural complications. A retrospective, single center, case series of 13 subjects treated with orbital atherectomy in iliac arteries to enable large bore device delivery was conducted. Patients were selected for treatment based on iliac artery disease or inability to deliver devices. The procedural complication rate was defined as the composite of flow-limiting dissection, perforation, slow flow, vessel closure, spasm, embolism, and thrombosis. Technical success was assessed as angiographic luminal gain and subsequent successful delivery of large bore devices through the treatment area, as well as freedom from procedural complications. Orbital atherectomy vessel preparation of severely calcified iliac artery lesions resulted in adequate stent expansion safely and enabled delivery of rigid/large profile devices. Further studies are warranted to evaluate patient selection criteria, as well as long-term efficacy and safety rates of orbital atherectomy in the iliac artery.
Keywords
Introduction
Endovascular intervention of iliac artery disease is less invasive than bypass surgery, does not require general anesthesia, has a high rate of technical success, and provides durable patency. 1 The 2016 American College of Cardiology/American Heart Association (AHA/ACC) Guidelines on the Management of Patients with Lower Extremity Peripheral Artery Disease (PAD) state that endovascular procedures are an effective revascularization strategy for patients with lifestyle-limiting claudication and hemodynamically significant aortoiliac occlusive disease (AOID). 2 The standard of care for the endovascular treatment of iliac artery disease is stenting and it provides comparable patency compared with aorto-femoral bypass surgery with a lower risk of infection and bleeding. 3 However, the presence of calcification may preclude the delivery of large bore devices, as well as stent placement or optimal stent expansion that could lead to restenosis, recurrence of ischemia, and repeat revascularization. Modification of calcified plaque with orbital atherectomy (OA) may facilitate the delivery and expansion of a balloon or stent, as well as other large bore devices. Data on OA in the iliac artery are limited, but a recent analysis indicated that OA in the iliac artery is feasible with few reported angiographic complications and compared favorably with a superficial femoral artery (SFA) control group. 4 Since there is a dearth of information, we present here a case series of OA utilization in the iliac artery to allow for large bore device delivery.
Case report series
The Diamondback 360 Peripheral Orbital Atherectomy System (Cardiovascular Systems, Inc. (CSI), St. Paul, MN, USA) was utilized in all 13 cases at a single center (WakeMed Heart & Vascular, WakeMed Hospital, Raleigh, NC, USA). As previously reviewed, the mechanism of the OA device has been shown to be useful in the treatment of calcified, noncompliant peripheral lesions prior to appropriate percutaneous transluminal angioplasty and adequate stent deployment if needed.5–7 As indicated in Table 1, the patient demographics of this case report series included elderly smokers with a high prevalence of diabetes and hypertension. These demographic risk factors are indicative of patients with severe peripheral artery disease and heavily calcified lesions. 5 In addition, the OA 2.0-mm crown was the most common crown size and a consistent algorithm of low-, medium-, and then high-speed rotation was utilized in all cases (Table 1).
Summary of baseline demographics and lesion/procedural characteristics.
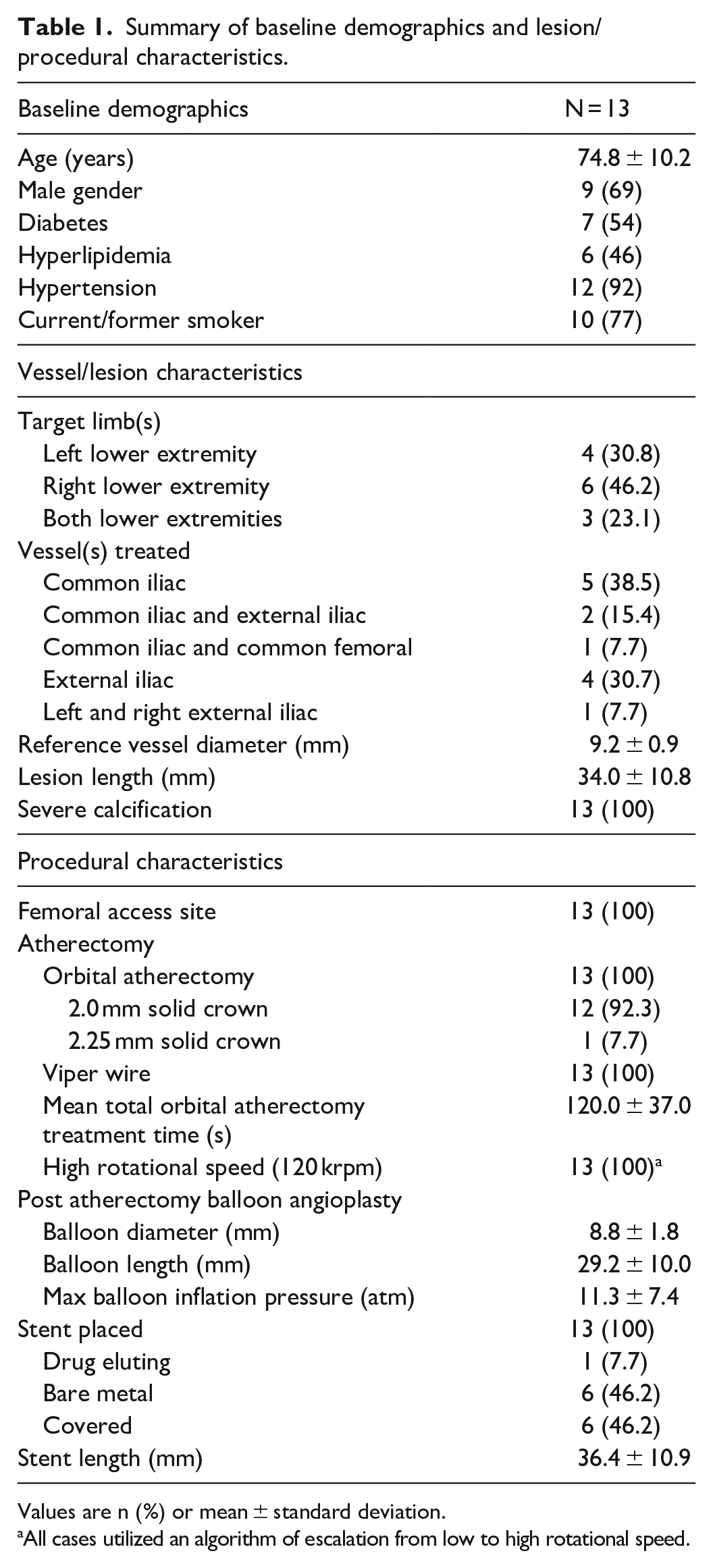
Values are n (%) or mean ± standard deviation.
All cases utilized an algorithm of escalation from low to high rotational speed.
Figures 1–3 provide examples of the OA utilization in severely calcified arteries after failed balloon angioplasty. Briefly, the asterisk in Figure 1(a) indicates a flow-limiting lesion preventing delivery of a guide sheath over an iliac bifurcation despite two failed attempts to advance the sheath with balloon angioplasty. Figure 1(b) shows the angiographic image post-treatment with the OA 2.0-mm solid crown and balloon angioplasty, enabling the delivery of the guide sheath and stent placement.
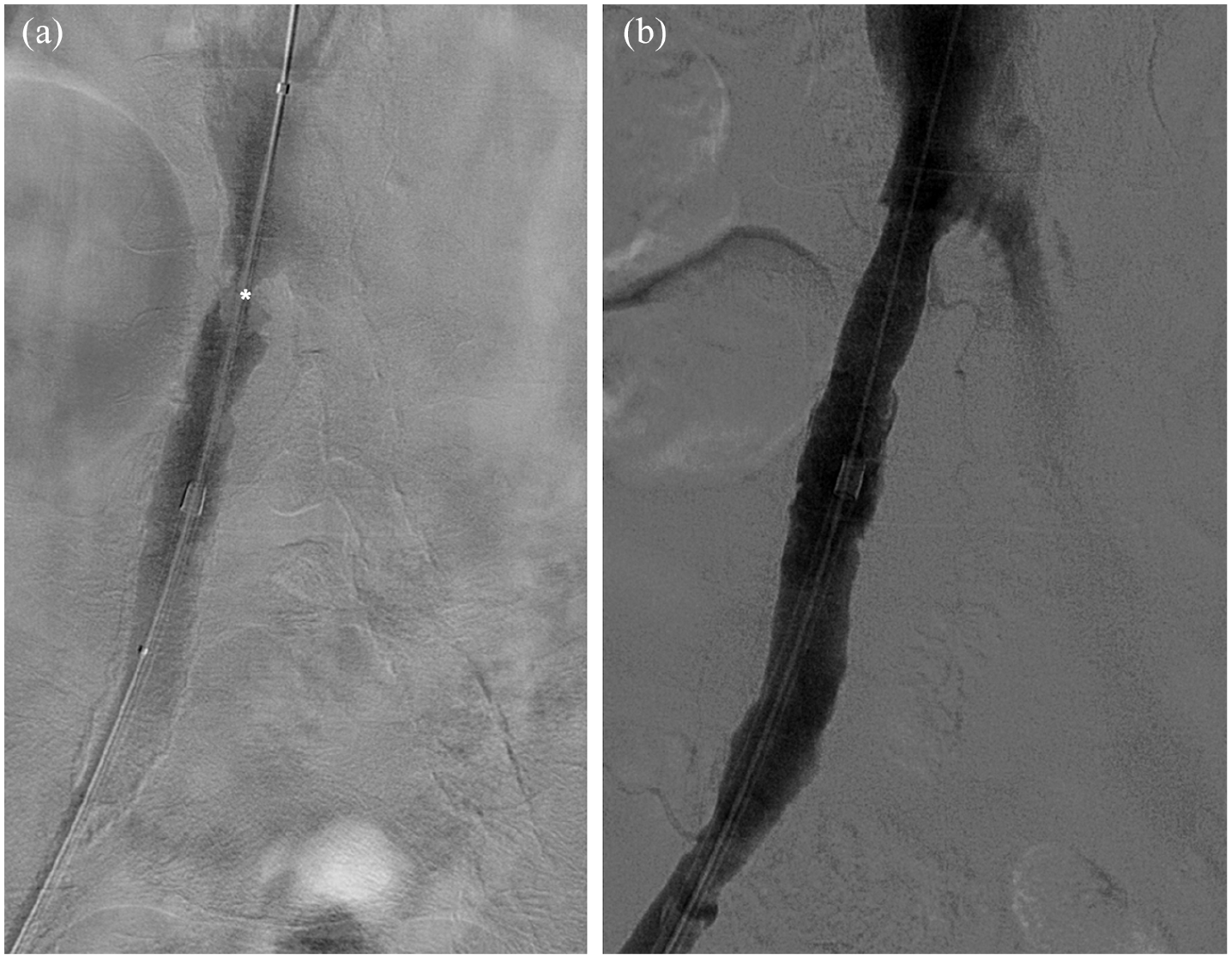
Treatment of the right common iliac to facilitate delivery of a guide sheath. *=flow-limiting lesion

Comparison of treatment methods in the left common iliac artery. *=proximal severely calcified stenosed target lesion; **=previous under-expanded stent
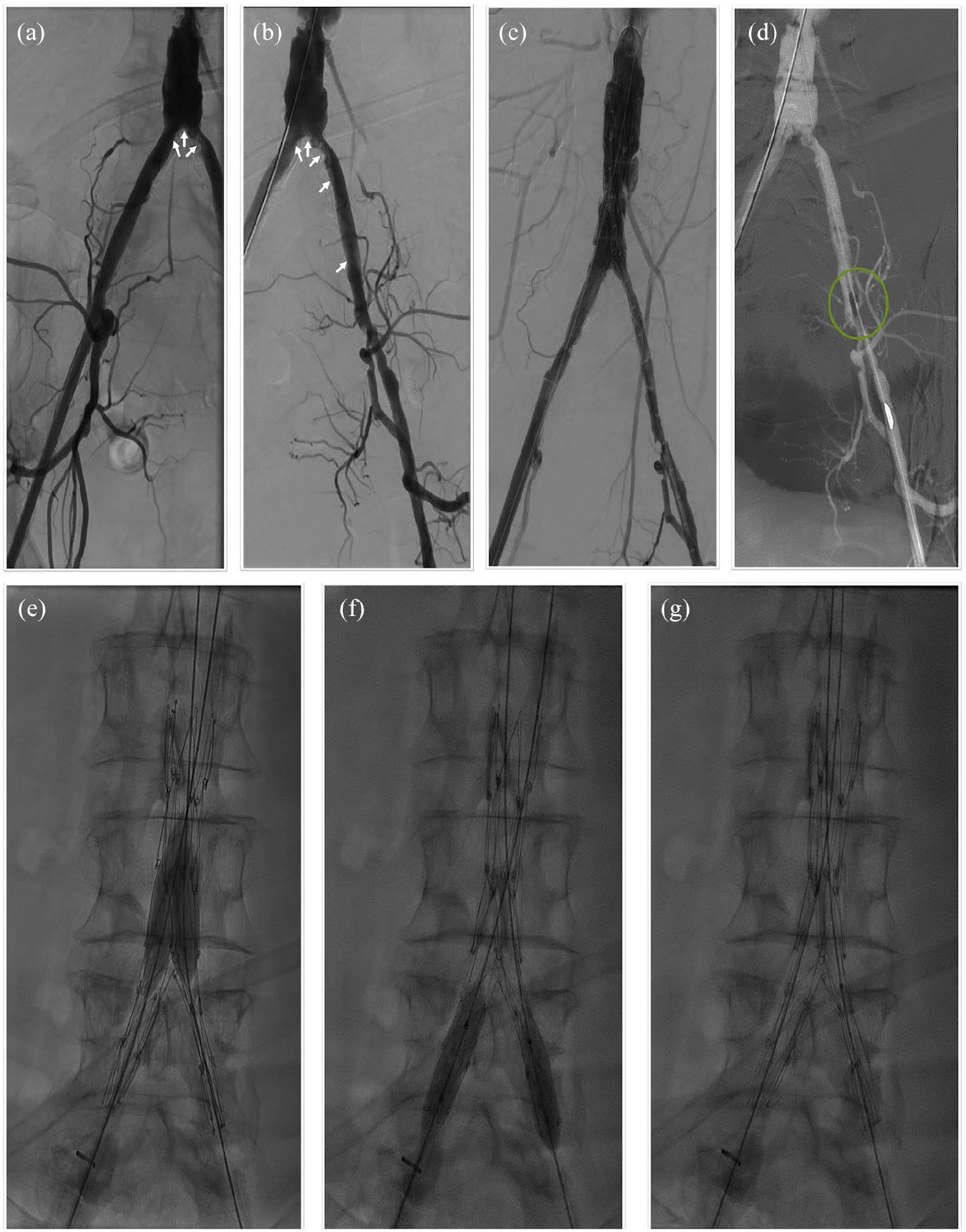
Bilateral iliac intervention for the delivery of a bifurcating endograft stent in an endovascular aneurysm repair. Arrows=severely calcified stenosed target lesions; green circle=OA crown
In a second case, the asterisk on a pre-treatment angiographic image (Figure 2(a)) shows a proximal severely calcified stenosed target lesion (outside/proximal to previously placed stent) that failed to respond to balloon angioplasty, while the double asterisk (Figure 2(a)) indicates a previous under-expanded stent due to failed balloon angioplasty and no treatment with OA. Figure 2(b) shows an angiographic image post-treatment of the proximal lesion (non-in-stent) with the OA 2.0-mm solid crown, balloon angioplasty, and stent placement, resulting in a fully expanded stent.
Finally, the third case (Figure 3(a)–(g)) is an example bilateral iliac OA treatment after a failed balloon angioplasty procedure, resulting in the successful placement of a large bore endovascular aneurysm repair (EVAR) endograft stent and subsequent resolution of a previously existing aortic aneurysm. Briefly, Figure 3(a)–(b) shows a baseline pre-treatment angiographic image of the aortoiliac region. Arrows indicate severely calcified stenoses of right and left common iliac arteries at the origin of the descending aorta, as well as further down into the left common iliac artery. Balloon angioplasty was attempted on these lesions, but it failed to create a large enough lumen to pass the large bore EVAR device through the aortoiliac region. Thus, the procedure escalated to OA treatment (Figure 3(c)–(d); green circle highlights the OA 2.0-mm solid crown) of these lesions which resulted in greater lumen gain and compliance change within the aortoiliac region for the successful placement of a bifurcating EVAR endograft stent (Figure 3(e)–(g)).
Overall, the retrospective analysis of the 13 cases revealed a low procedural complication rate (0%) and a high technical success rate (100%). The procedural complication rate was defined as the composite of flow-limiting dissection, perforation, slow flow, vessel closure, spasm, embolism, and thrombosis. Technical success was assessed as angiographic luminal gain and subsequent successful delivery of large bore devices through the treatment area, as well as freedom from procedural complications. Orbital atherectomy vessel preparation of calcified iliac artery lesions resulted in adequate stent expansion and enabled delivery of large profile devices.
Discussion
Aortoiliac occlusive disease (AIOD) occurrence will likely increase as the prevalence of PAD related co-morbidities becomes more widespread; a careful examination of treatment strategies and an appreciation for calcification will be necessary. Despite the challenges of treating AIOD, it is clear that patients want and need these procedures—a randomized study showed that patients’ quality of life improved after receiving endovascular treatment for AOID. 8 There are many available options for the treatment of calcification in AIOD, and new treatment options will surely offer additional opportunities to combat calcium. Current recommendations support an endovascular approach for AIOD, 9 but other methods are available when endovascular techniques fail. Endovascular techniques appear effective among different vascular beds and the risk/benefit themes remain. Studies have also shown endovascular treatment of aortoiliac calcific occlusive disease to be technically successful, low risk, and offer short-term success. More information is needed to fully appreciate how the presence of calcification alters the success of endovascular techniques and how it affects treatment strategies. More studies are needed to see how the presence of calcification affects restenosis rates in these larger vessels. Cost considerations will also become increasingly important as providers are required to operate under cost consignment programs. The case report series presented here provides examples of successful OA in iliac arteries that facilitated the delivery and expansion of a balloon or stent, as well as other large bore devices. One major limitation of this case series, however, is the lack of intravascular imaging (intravascular ultrasound (IVUS) or optical coherence tomography (OCT)) before and after OA to determine the precise effects of the device. Since IVUS and OCT are infrequently used during OA aortoiliac peripheral interventions, it would be of value to complete a prospective intravascular imaging study of OA treatment for AOID.
Conclusion
OA vessel preparation of calcified iliac artery lesions resulted in adequate stent expansion safely and enabled delivery of rigid/large profile devices. Larger studies are warranted to evaluate patient selection criteria, as well as long-term efficacy and safety rates of OA in iliac arteries.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.R. has a consulting agreement with Cardiovascular Systems, Inc. (CSI). D.P. has no declarations of interest. B.J.M., J.H., and H.D. are employees of CSI. These conflicts did not affect the study design, conduct, or reporting.
Ethical approval
Ethical approval to report this case series was obtained from WakeMed Institutional Review Board (approval number/ID: 1551249-1).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
In this single center case series, IRB waiver was received (a waiver of informed consent and a complete HIPPAA waiver were granted) by the WakeMed Institutional Review Board (approval number/ID: 1551249-1) for the anonymized information to be published in this article.