
Abstract
The occurrence of an ectopic pregnancy that implants within the peritoneal cavity is a rare, life-threatening event. Poor maternal and fetal outcome, especially in pregnancies within the range considered to be viable, is the norm, with most abdominal ectopic pregnancies being terminated early in gestation. We present a case study in which the abdominal pregnancy was detected in the second trimester by sonography and confirmed by magnetic resonance imaging, both of which are considered essential diagnostic tools to provide optimal outcome for maternal and fetal well-being.
An ectopic pregnancy located within the peritoneal cavity with a blood supply derived from the visceral vasculature presents a diagnostic challenge for sonographers and physicians. Because of the rare occurrence of abdominal ectopic pregnancy, great care must be given to the determination of placental implantation and the vascular connections associated with the maternal-placental complex. In cases in which an abdominal pregnancy is not identified until the mid-late second trimester and the parent(s) wish to continue the pregnancy despite the noted risks, it is imperative that amniotic fluid levels are monitored using sonography.1,2 Massive maternal hemorrhage from the visceral blood supply secondary to poor presurgical planning is often the outcome when these rare pregnancies go undetected. 3 In cases that present early in the gestation in which no intrauterine pregnancy is identified and an adnexal or abdominal mass is noted, along with increasing serum human chorionic gonadotropin, the sonographer is challenged to ascertain the location of the pregnancy as well as placental location. The diagnostic question that must be answered is the following: Is the pregnancy within the fallopian tube where most ectopic pregnancies occur, or is it located within the peritoneal cavity with a visceral/omental vascular supply to the maternal-placental complex?
Case Report
A 33-year-old woman, gravida 2, para 1, with an estimated gestational age (EGA) of 19 3/7 weeks by menstrual history, presented to the sonography department for further evaluation of a possible abdominal ectopic pregnancy identified on an outside sonogram. Access to any other recent medical history of this patient was limited. The transabdominal and endovaginal examinations were performed with a GE Voluson E8 Expert scanning system using M6C 1–7 MHz transabdominal and IC5 4–9 MHz endocavitary transducers.
The initial transabdominal sonographic examination showed an anteverted uterus with an empty endometrial cavity. Measurements of the uterus were 9.38 cm in length and 6.03 cm in antero-posterior diameter. A mid-level gray, homogeneous structure abutted the uterine fundus and was consistent with the sonographic appearance of placental tissue (Figure 1). A single, viable fetus within a membranous sac with adequate amniotic fluid was also identified. Fetal biometry was consistent with a gestational age of 19 3/7 weeks. Both endovaginal and transabdominal color Doppler imaging showed a placental vascular supply from the uterine fundus (Figures 2 and 3). Following the sonographic examination, the patient was admitted to the hospital for further medical management and for a magnetic resonance imaging (MRI) evaluation, which confirmed the placental attachment to the superior aspect of the urinary bladder, the left lateral pelvic wall, the retroperitoneum, left iliac vessels, and the left ureter. The MRI also showed a vascular supply to the placenta from the uterine fundus as well as from the adnexal and iliac vessels. In addition, the fetal lie was established as transverse (Figure 4). Hydronephrosis of the maternal left kidney was noted secondary to mass effect compression of the left ureter.
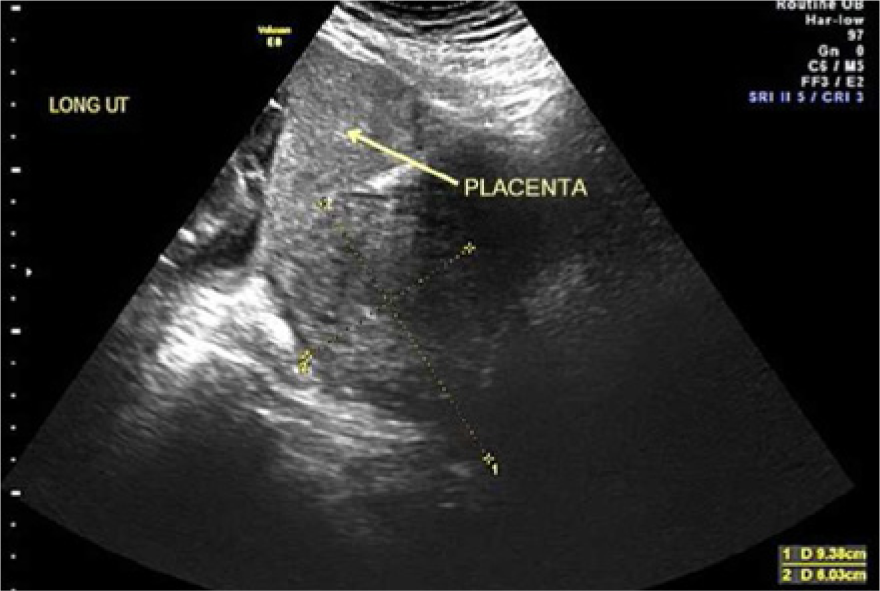
Longitudinal transabdominal gray-scale image of empty uterus (calipers) and extrauterine abdominal pregnancy with the placenta abutting the uterine fundus.
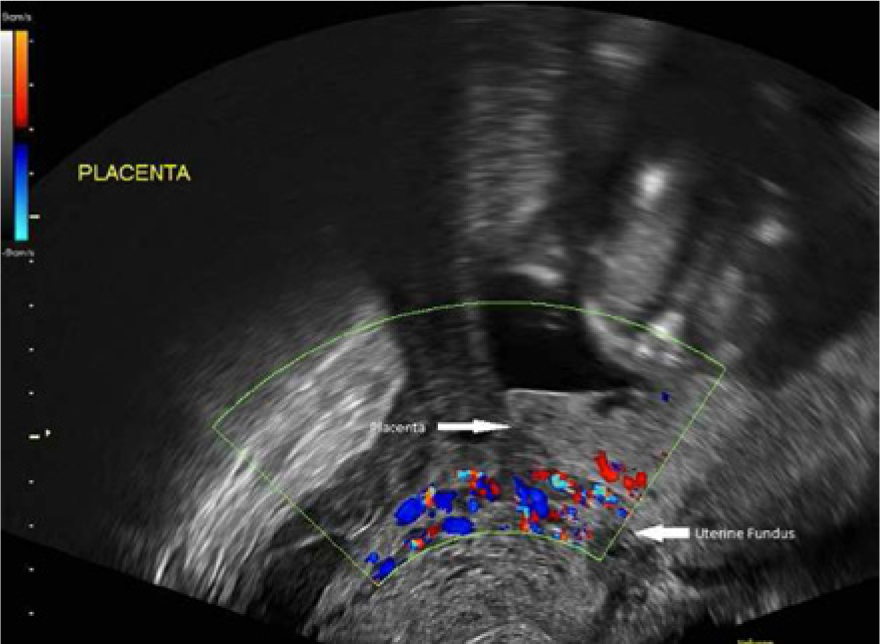
Coronal endovaginal color Doppler image of the blood supply from the uterine serosa to the placenta.
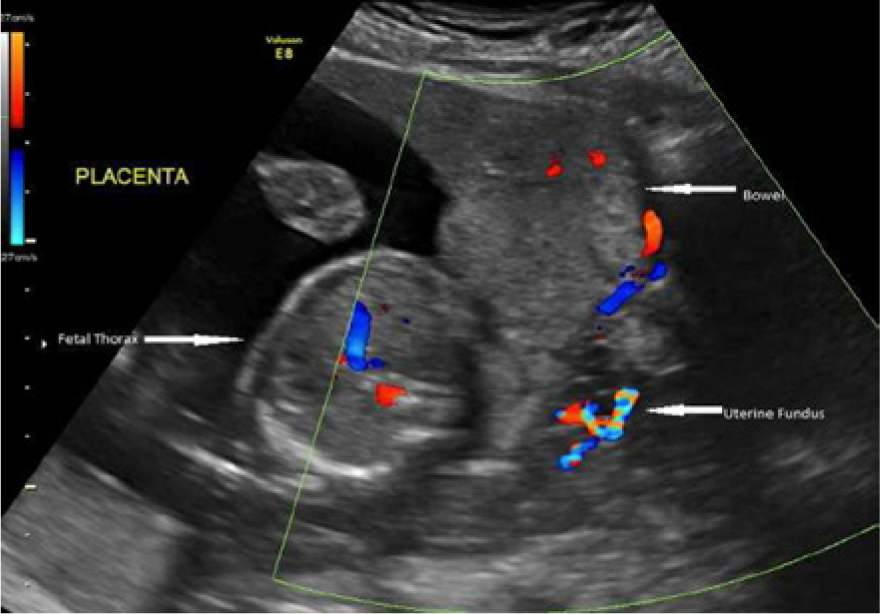
Sagittal transabdominal color Doppler image of the blood supply from the uterine serosa to the placenta.
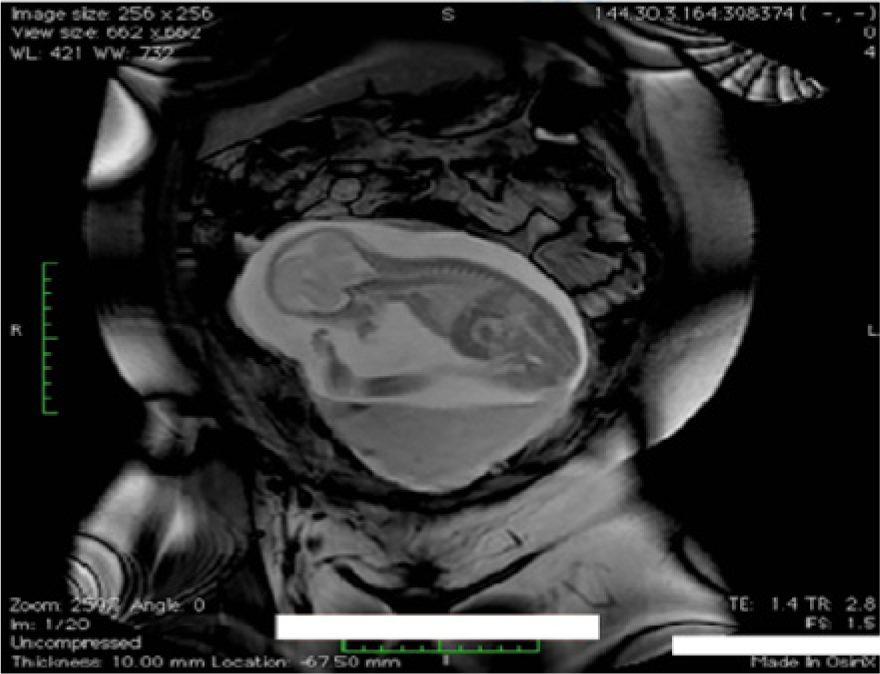
Coronal magnetic resonance image showing the transverse fetal lie.
The patient was counseled concerning the risks involved with continuing the pregnancy, but she chose to continue the pregnancy with close supervision using sonography and MRI. Follow-up examinations using both imaging modalities were performed at 23 and 24 weeks of gestational age. The 23-week sonogram showed that the amniotic fluid index (AFI) was again within normal limits (AFI = 18.9 cm; Figure 5), with normal interval growth of the fetus (EGA 22 3/7 weeks). The fetal heart rate was 158 bpm, and spectral Doppler evaluation of the systolic/diastolic ratio of the umbilical cord artery and resistive index calculations for the middle cerebral arteries were within normal limits. Eleven days later, at 24 1/7 weeks EGA, a limited sonographic evaluation demonstrated an AFI of 8.0 cm, which was a clinically significant change in amniotic fluid volume. 1 An MRI was performed immediately following the sonogram, because body habitus severely limited visualization of a possible cause of the decrease in AFI. The MRI demonstrated a perforation in the amniotic sac with retroplacental hemorrhage (Figure 6). The decision was made to deliver the fetus at this point via laparotomy. A viable, male fetus was delivered. Maternal and neonatal follow-up were not available to the staff.
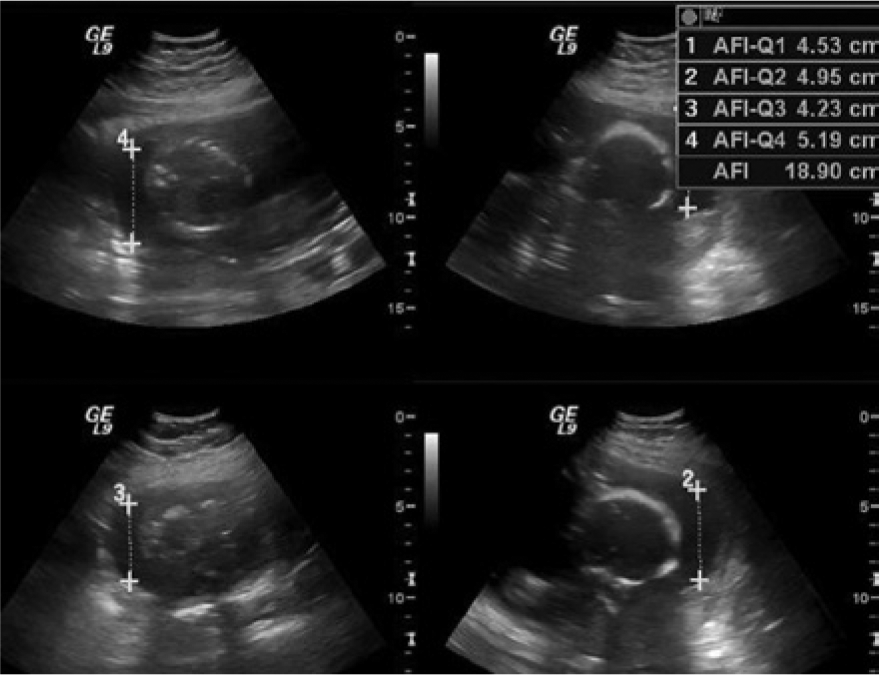
Transabdominal gray-scale images of the amniotic fluid index measurements.
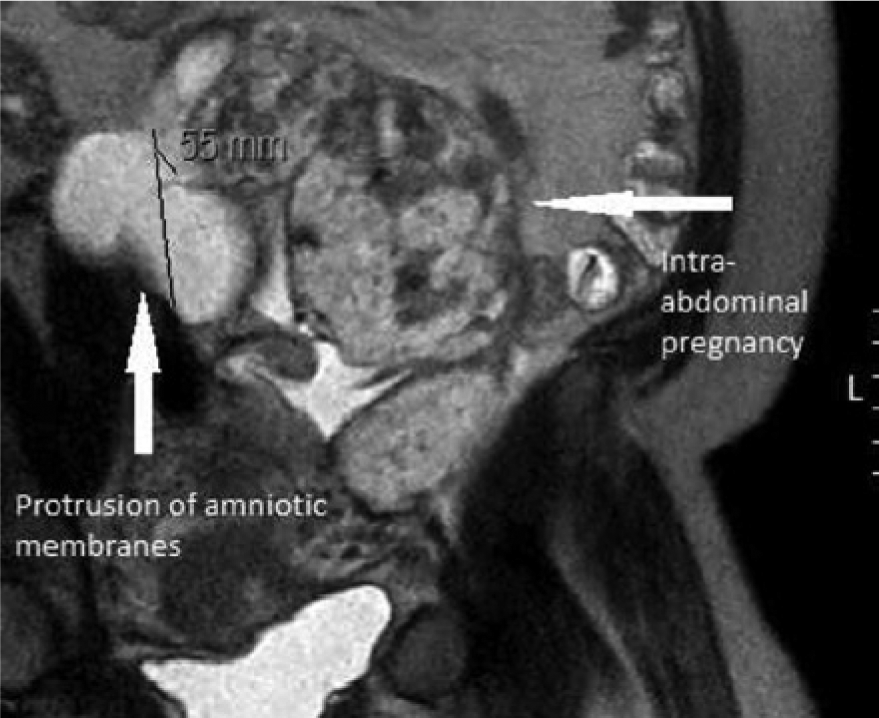
Sagittal magnetic resonance image of the ruptured amniotic sac.
Discussion
Extrauterine abdominal pregnancies are rare and are often missed during the initial sonographic examination. In the United States, approximately 1 in every 10 000 pregnancies is diagnosed as an extrauterine abdominal pregnancy, with the maternal mortality rate hovering at 90 times that of a normal delivery. The perinatal mortality rate for these rare ectopic pregnancies is in the 40% to 95% range.2,3 It is extremely important that sonographers examine each pregnancy for identification of the myometrium, placental attachment, and the adnexal structures to exclude the possibility of an abdominal ectopic pregnancy.
This type of ectopic pregnancy, while carrying the same risk factors as other extrauterine pregnancies (for example, a tubal ectopic pregnancy), can be misdiagnosed as to its location when the pregnancy is identified later during the gestational period if the normal pelvic landmarks are not seen. One case report from Ghana states that a woman had five sonographic examinations that missed a term abdominal pregnancy. 4 This late identification, according to Gupta et al., 3 “carries a risk of sudden intra-abdominal bleeding and generally poor fetal prognosis.” In addition, the presence of congenital defects in many of these neonates further complicates their chances of survival. 4 In the cases presented by Dahab et al. 2 and by Gupta et al., 3 the ectopic abdominal location of the pregnancies was not identified until laparotomy was performed subsequent to extensive maternal bleeding.2,3 In both cases, the former at 40 weeks’ gestation and the latter at 41 1/7 weeks’ gestation, the laparotomy showed the abdominal locations, and excessive bleeding occurred because of a lack of presurgical planning for this eventuality. The decision was made to leave the placenta, or at least a large portion of the placenta, in situ because of the massive bleeding in both of these cases.
An abdominal pregnancy results from one of two events: primary abdominal pregnancies occur when implantation of an embryo is in the peritoneal cavity, and the fallopian tube and the ovary remain intact, whereas secondary abdominal pregnancies result from rupture of an existing tubal pregnancy with the embryo then reimplanting in the peritoneal cavity. The latter is more common and is typically evidenced by either tubal or ovarian damage. 2 Sonography is the primary imaging modality for diagnosing extrauterine abdominal pregnancies, with most women having a sonogram during prenatal care early in the gestational course for dating purposes or at the latest between 18 and 20 weeks for a general anatomic survey. Even so, abdominal ectopic pregnancies are commonly missed in the antenatal period, increasing the risks of massive hemorrhage as the pregnancy progresses or at delivery via laparotomy.
Sonography is instrumental not only in determining the location of the pregnancy and the origin of the blood supply to the placenta but also in identifying coexisting pathology that may affect the time element in identifying the abdominal location. Faustin et al. 5 reported the presence of uterine myomas, which obscured and delayed the diagnosis, and the ectopic abdominal site was discovered at 31 weeks of gestational age during an emergency laparotomy after failed induction secondary to noted oligohydramnios. Kim et al. 6 presented a case in which the patient had an 18-week gestation and a coexistent, large (>10 cm) mature cystic teratoma. After using sonographic imaging to determine that there was a high probability that the ectopic location was within the peritoneal cavity secondary to the demonstration of an empty uterine cavity and a coexisting adnexal mass, the patient was counseled concerning the risks and chose to continue the pregnancy. Serial sonograms monitoring fetal growth and amniotic fluid levels were performed, and at 34 weeks, a laparotomy was carried out to avoid the early rupture of membranes. Although MRI was the primary preoperative planning imaging modality in that case, sonography was essential for the monitoring of the pregnancy as to the overall well-being of the amniotic environment.
Controversy exists as to whether or not to intervene early in the pregnancy with surgery or to allow the pregnancy to continue if the identification of the abdominal location is discovered at or after 24 weeks’ gestation. The variables of amniotic fluid levels, patient wishes, and the availability of a comprehensive presurgical plan for removing the placenta from the visceral vascular supply play extremely important roles in the management of this very-high-risk pregnancy. 7 In the case presented here, the patient wished to continue the pregnancy and was monitored with both sonography and MRI. Laparotomy for delivery was done after the sonographic finding of the decrease in amniotic fluid as well as because the gestational age was greater than 24 weeks.
Summary
Advanced extrauterine abdominal pregnancies account for less than 1% of ectopic pregnancies. They are often life threatening, and antenatal diagnosis is essential to help decrease maternal and fetal morbidity and mortality. Sonography and MRI are two imaging modalities that can provide critical diagnostic information to clinicians to help improve the outcome for both the mother and the fetus. In the presented case, both sonography and MRI were used in diagnosing and evaluating the abdominal pregnancy. In part because of these advanced imaging modalities and accurate antenatal diagnosis, as well as proper surgical planning, a positive maternal and fetal outcome was made possible.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.