
Abstract
Abdominal ectopic pregnancy is a rare type of ectopic pregnancy that is associated with high morbidity and mortality. This study reports a case of advanced abdominal ectopic pregnancy at 26-weeks’ gestation in a 31-year-old primigravida whose conception was a result of in vitro fertilization because of infertility due to male factors. Her past history is significant for a congenital Horseshoe kidney. Initially, she presented at the 8th week of gestation with a clinical picture that is consistent with ectopic abdominal pregnancy; however, she refused to terminate her pregnancy despite medical advice. At 26 weeks gestation, she presented to the emergency department again complaining of lower abdominal pain and vaginal spotting, and underwent an abdominal laparotomy without any complications. The postoperative period was unremarkable, and she was discharged after 7 days. In conclusion, early diagnosis and management of such cases are of paramount importance and lead to favorable outcomes. Nevertheless, we stress the importance of providing effective counseling to patients presenting with serious conditions through clear information along with proper psychological support for couples.
Introduction
Ectopic pregnancy refers to the implantation and development of a fertilized ovum outside the main cavity of the uterus. The current incidence of ectopic pregnancy is difficult to estimate; surveillance data is imprecise and limited, but in the United States, the incidence of ectopic pregnancy between 2006 and 2013 increased from 11 to 13.7 ectopic pregnancies per 1000 live births. 1 Several risk factors are associated with ectopic pregnancy, including previous ectopic pregnancy, history of pelvic inflammatory disease, history of infertility, and use of assisted reproductive technology.2,3 Abdominal ectopic pregnancy is a rare condition that accounts for 0.6%–4% of all ectopic pregnancies and is associated with mortality rate that is eight times higher than tubal pregnancies. 4 Abdominal pregnancy can be classified according to the gestational age at presentation; early ectopic pregnancy presenting before the 20th week of gestation, and advanced ectopic pregnancy that is diagnosed later on. Evaluation and management of abdominal ectopic pregnancies are challenging, particularly in advanced cases, due to their insidious presentation and high rates of complications and mortality. 5 In this study, we report a case of advanced abdominal ectopic pregnancy presenting at 26th week of gestation.
Case presentation
Our case is a 31-year-old primigravida, at 26-weeks’ gestation presenting to the emergency room of Al-Shifa Medical Complex. She underwent in vitro fertilization (IVF) with a frozen embryo because of male factor infertility. She is known to have a congenital Horseshoe kidney. Her past surgical and family history are unremarkable. In the first trimester (8 weeks’ gestation), she had complained of recurrent vaginal spotting and abdominal pain with absence of intrauterine pregnancy on transvaginal ultrasound along with elevated human chorionic gonadotropin hormone (β-hCG); therefore, a diagnosis of abdominal ectopic pregnancy was presumed. However, the patient refused to be admitted to the obstetrics and gynecology department for further evaluation and management despite medical advice. Although she had further recurrent abdominal pain and vaginal spotting, she did not attend any outpatient follow-up appointments. At 26 weeks gestation, she presented to the emergency department complaining of lower abdominal pain and vaginal spotting with urinary retention, which she attempted to relieve by warm water baths.
On examination, the patient was vitally stable, and her abdomen was distended with moderate tenderness. Laboratory blood tests showed normal hemoglobin (Hgb) (10.8 g/dl) and a normal white blood cell count (WBC) (8.4*109/L). Abdominal ultrasound (US) revealed an empty uterus ,an intact abdominal gestational sac containing a deformed viable fetus, and a placenta that is adjacent to the bladder (See Figure 1). On the same day, the patient underwent an abdominal laparotomy to deliver a 15 cm × 10 cm size gestational sac. Large bowels were adherent to the gestational sac, for which adhesiolysis was done with complete excision of the attached mesentery. As the placenta was rendered free from surrounding bowel, the surgeon decided to remove the placenta completely. The baby was delivered with the placenta without significant bleeding. The baby had deformed lower limbs and skull bones (Figure 2). As the patient had a horseshoe kidney, double J-stents were inserted bilaterally by cystoscopy in order to avoid any injury to the ureters. There was evidence of left ovarian tube rupture due to adherence to the sac; as a result, left salpingo-oophorectomy was performed. She received one packed red blood cell unit during the operation.
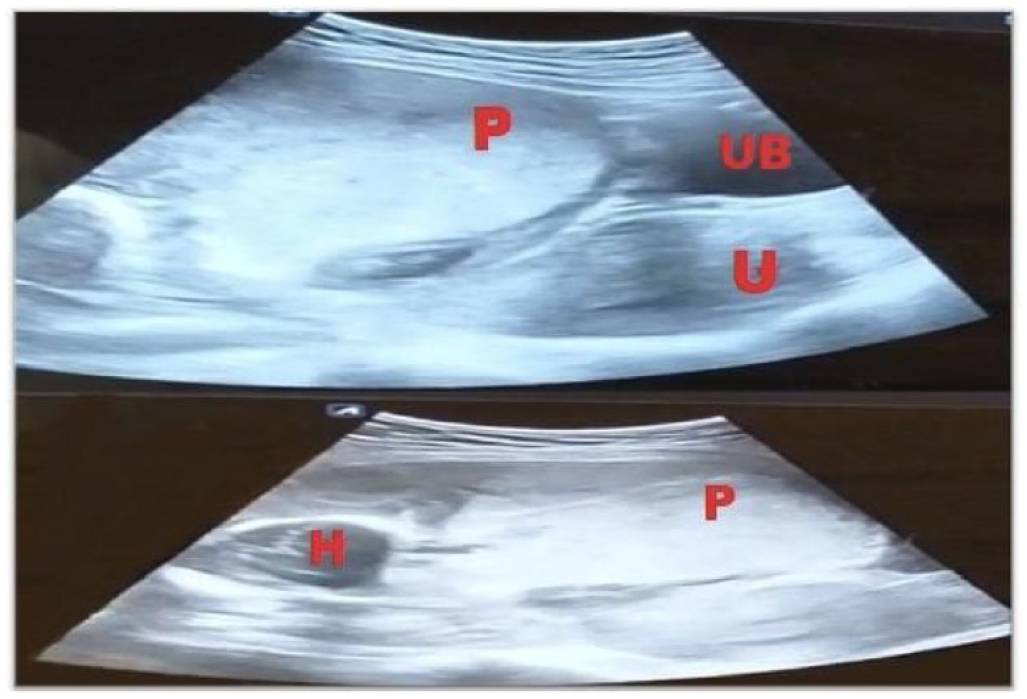
Ultrasound picture for the ectopic abdominal pregnancy showing an empty uterus (U), an extra-uterine gestational sac as well as the head of the fetus (H) with the placenta (P) overlying the urinary bladder (UB).

Two pictures showing the malformed baby (a) and the placenta (b).
The postoperative period was unremarkable, and she was discharged after 7 days. Two weeks after the operation, her condition was good with no complaints or complications. One week later, the double J-stents were removed.
Discussion
In this study, we reported an interesting case of an unruptured advanced abdominal ectopic pregnancy presenting in the late second trimester in a nulliparous female. The rarity of this condition makes it a valuable case to report. Additionally, by exploring a unique form of ectopic pregnancy, management strategies, and possible counseling gaps, this case should guide future clinical practice in order to achieve earlier detection and management for such acute entity.
Abdominal ectopic pregnancy can be classified as primary or secondary. Primary abdominal pregnancy is the result of direct implantation of the fertilized ovum in the abdominal cavity. In such cases, the fallopian tubes and ovaries are intact. Alternatively, a secondary abdominal pregnancy occurs when an extra-uterine tubal pregnancy ruptures or aborts and gets re-implanted within the abdomen. 6 Approximately 1.4% of ectopic pregnancies are abdominal pregnancies that can result from secondary implantation of an aborted tubal pregnancy.7,8 This study reports a case of abdominal ectopic pregnancy secondary to abdominal implantation of fertilized ovum during IVF procedure. Frozen embryo transfer was used for the study patient; however, the literature showed that ectopic pregnancy was 65% less likely to occur in patients who had a frozen embryo transfer compared with a fresh embryo transfer. This may be attributed to the use of hormone stimulation for fresh embryo transfers.9–13 Zhang et al. 12 hypothesized that the high levels of estrogen and progesterone used in frozen embryo transfer may account for higher rates of ectopic pregnancy. First, estrogen in high concentrations may impair the sensitivity of estrogen receptors, resulting in accelerated interstitial development compared with glandular development due to reduced endometrial glandular proliferation and increased stromal hyperplasia. 13 Second, misbalanced estrogen-to-progesterone ratio might lead to delayed glandular development in comparison to interstitial development, which in turn would impair implantation of embryos.
A delayed diagnosis and difficulty managing an abdominal pregnancy result in a significantly higher mortality rate than an uncomplicated ectopic pregnancy. In the United States, from 2011 to 2013, hemorrhage from ruptured ectopic pregnancy accounted for 2.7% of all pregnancy-related deaths during the first trimester. 14 Mortality rate for ruptured ectopic abdominal pregnancies is 89.8% higher than in intrauterine pregnancy. 15
In our case, the diagnosis was established early, but regrettably, the patient had chosen not to proceed with the recommended surgery. The counseling process may have had some gaps, which might have affected her understanding of the process and the significant risks that she was taking. In addition, it may have been beneficial to provide additional support and assistance in order to ensure that the surgery and its possible benefits are clearly understood.
Our patient was at high risk of ureteral injury due to mainly two reasons: first, she has a horseshoe kidney, a condition that carries a significant risk of ureteral injury during intra-abdominal surgeries. Second, adhesions in the operative field would necessitate careful and cautious manipulation during surgery in order to avoid any accidental injuries. Consequently, double J-stents were placed to assist with intraoperative identification of the ureter and prevent any secondary injury.
The surgeon rarely has difficulty removing the fetus from the sac, although the management of the sac, adhesions, and, in particular, the placenta, as well as the control of any hemorrhage, are more challenging tasks. For the management of the placenta, there are primarily two options, and the first is to remove the placenta after ligating the placental blood supply if placental separation is not difficult. This is done because, otherwise, surgeons may experience massive hemorrhages as they remove the placenta, which would require extensive management. Hence, the decision to remove the placenta should be undertaken upon the accessibility of ligation of the maternal vessels supplying the placenta. Placental removal may also be facilitated by selective arterial embolization preoperatively.5,16 In a case series of 12 patients with abnormal placental implantation, pelvic artery embolization was used in the prevention of postpartum hemorrhage, which led to a technical success rate of 100%. 17 Unfortunately, this was not performed in our case as it is a procedure that requires interventional radiology expertise that is available to operate in the obstetric operating room. The second option is leaving the placenta in situ after ligating the umbilical cord, which is safer for the patient. 8 For this reason, the decision of removing the placenta should be taken cautiously. With the placenta easily separated from adjacent mesentery, the decision in our case was to remove the placenta, which went uneventful.
The main limitation of our report is that we could not provide details about the course of pregnancy as the patient did not present for follow-up appointments after she was diagnosed at the 8th week of gestation.
Conclusion
This case highlights the risks of ectopic pregnancy and outlines the approach to operate on the placenta in order to avoid severe bleeding and organ injury by establishing a comprehensive clinical judgment. Furthermore, we recommend counseling for partners who are planning for IVF to discuss the possible complications along with provision of psychological support for vulnerable groups. In addition, clear information regarding the seriousness of ectopic pregnancy and its potential complications should be provided along with psychological support for this vulnerable group of patients.
Footnotes
Acknowledgements
Not applicable.
Author contribution
All authors contributed significantly to the preparation of this manuscript, and all are granted authorship. All authors reviewed the final version of the manuscript and approved its publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.