
Abstract
Ectopic pregnancy is a life-threatening condition that warrants immediate treatment due to the risk of rupture and resultant hemorrhaging. Less than 1% of all pregnancies are ectopic; of these, 90% or more are located in the fallopian tubes. In a clinical setting, sonography can diagnose an ectopic pregnancy in conjunction with beta-human chorionic gonadotropin (B-hCG) levels above 1500 mIU. A case is presented in which the diagnosis of ectopic pregnancy was supported through sonographic features. Medication was given to terminate the ectopic pregnancy; however, surgery was later needed when the ectopic ruptured.
An ectopic pregnancy is a pregnancy that does not occur inside the uterus, most commonly occurring in the fallopian tubes, but it may also occur in interstitial, cervical, and abdominal areas. 1 Ectopic pregnancy can be life threatening if not diagnosed in a timely manner. Ectopic pregnancy requires immediate intervention through surgery or medication. The ectopic pregnancy can rupture, and shock and internal hemorrhage can lead to an emergency situation. 2 Sonography is a key imaging modality used in diagnosing ectopic pregnancy since it can determine whether the pregnancy is an intrauterine or extrauterine gestation. With the advance of transvaginal sonography, clearer and more detailed images can be obtained when evaluating the uterus, and especially the ovaries, because of the ability to use higher transmit frequency probes as compared to transabdominal sonography.
Case Report
A 28-year-old female presented to the emergency department with concern for an ectopic pregnancy. Blood work was ordered that revealed her serum quantitative beta-human chorionic gonadotropin (B-hCG) level was 15 248 mIU/mL. (Normal values in nonpregnant females are < 5 mIU/mL.) She displayed no emergent physical symptoms and had no medical history to increase her risk of having an ectopic pregnancy.
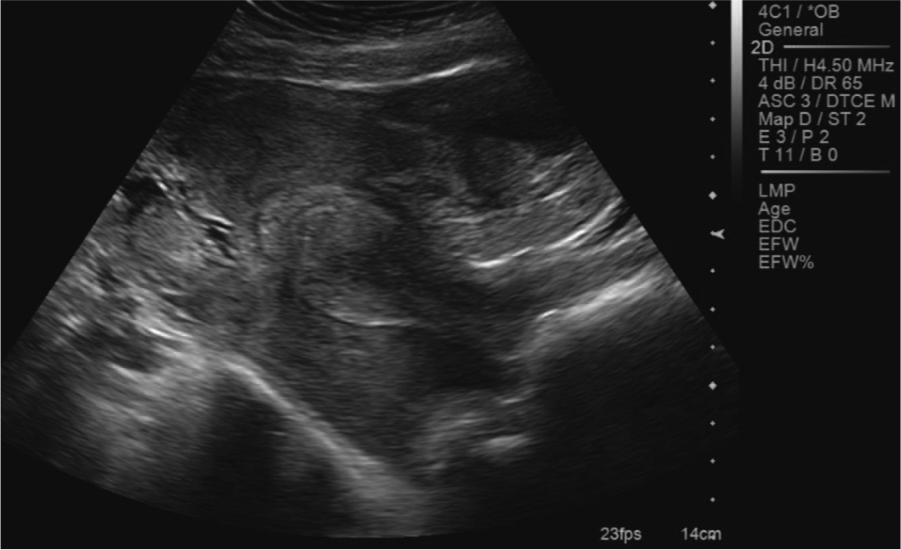
A sonogram was performed and demonstrated an anteverted uterus that measured 9.9 × 3 × 5 cm with an endometrial measurement of 1.8 cm (Figures 1 and 2). No evidence of an intrauterine gestation was found. As shown in Figures 3 and 4, the left ovary measured 2.9 × 2.9 × 2.2 cm with an irregular cystic component that displayed increased vascularity surrounding the ovary (Figure 5). Figures 6 and 7 show a left adnexal mass measuring 2.2 × 2.2 × 1.8 cm that was highly suspicious of an ectopic pregnancy. The right ovary demonstrated normal flow and measured 3.1 × 1.8 × 2 cm with a 1.3 × 1.2 × 1 cm septated cyst (Figure 8). No free fluid was found in the cul-de-sacs. These results were called to the emergency department physician by the reading radiologist as soon as the sonographic examination was completed.
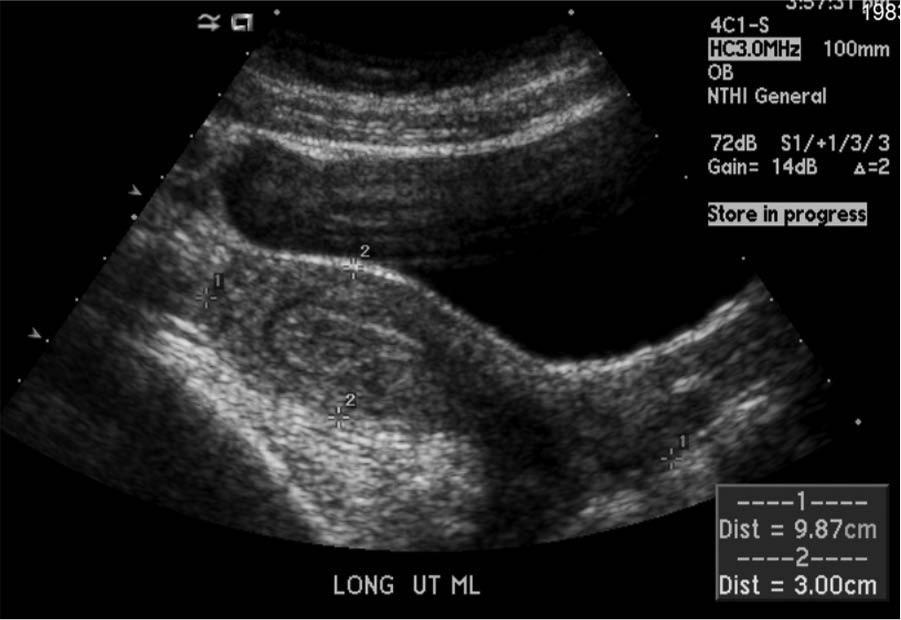
A transabdominal longitudinal midline image showing an anteverted uterus measuring 9.9 × 3.0 cm; no gestational sac was seen inside the uterus. Note was made of a thickened endometrium.
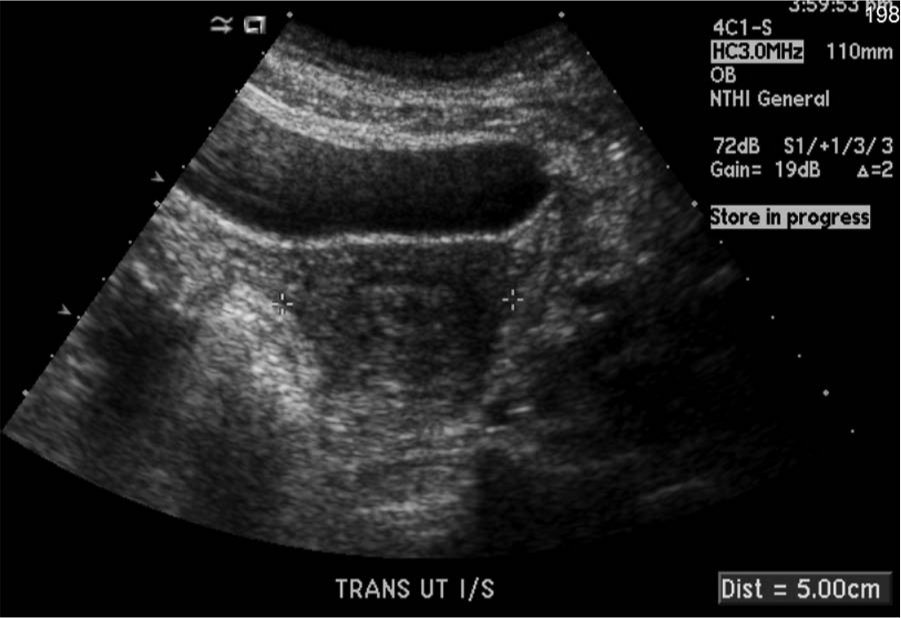
A transabdominal transverse image of the uterus, which measured 5.0 cm across.
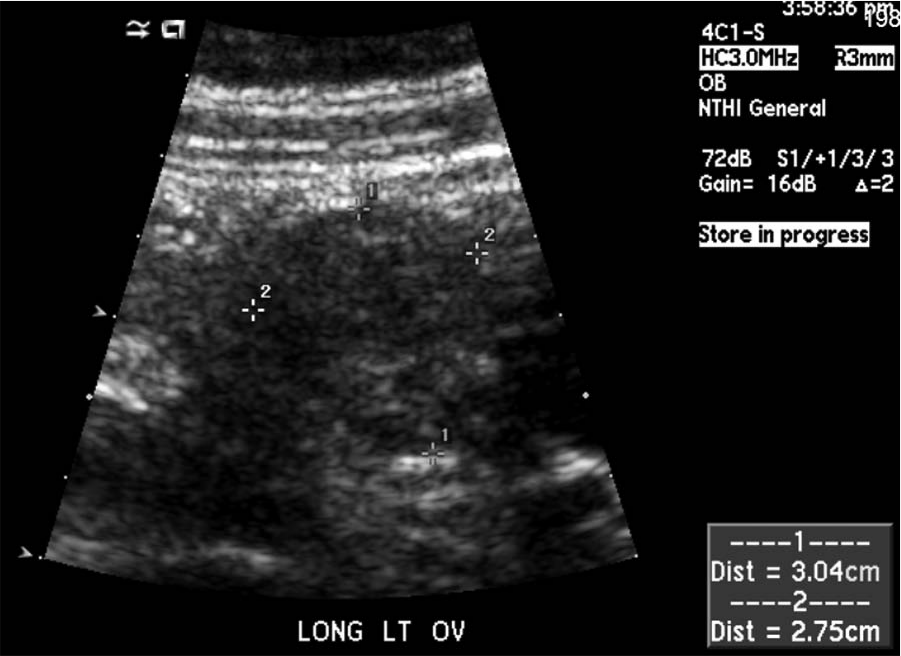
A transabdominal image of the left ovary shown in a longitudinal plane, measuring 3.0 × 2.8 cm.
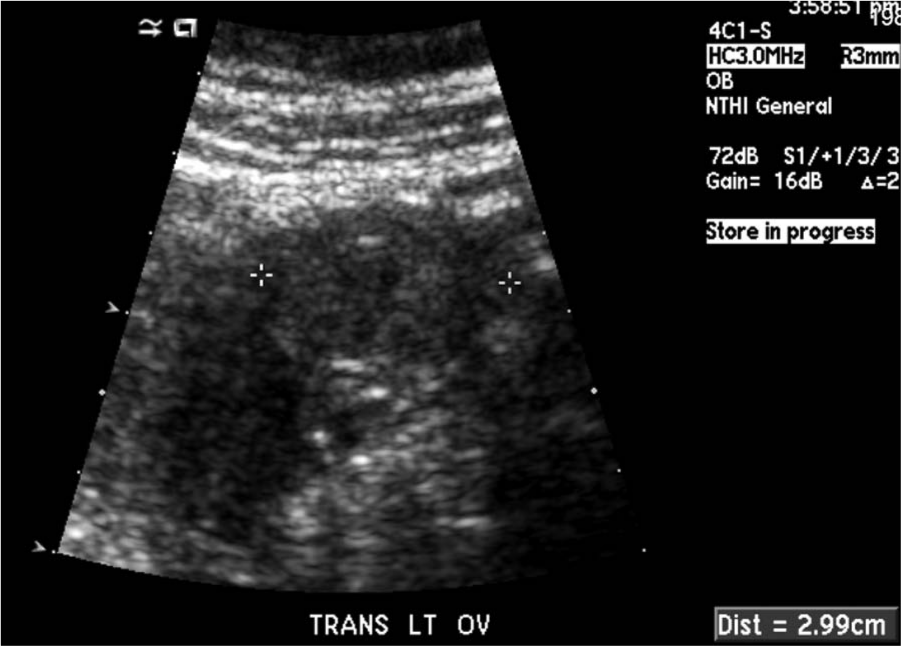
A transabdominal image of the left ovary in a transverse plane, measuring 3.0 cm.
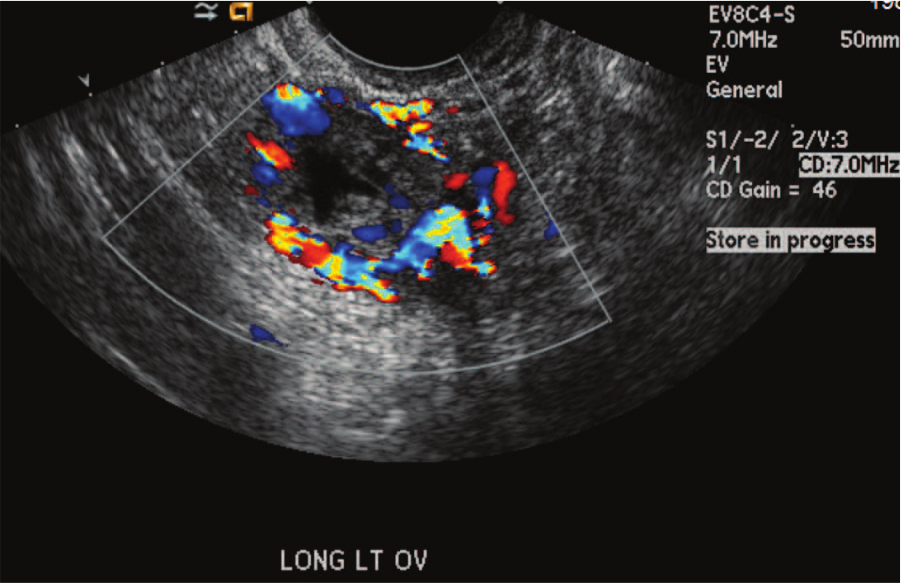
A transvaginal image of the left ovary in a longitudinal plane with color Doppler demonstrating the “ring of fire” appearance.
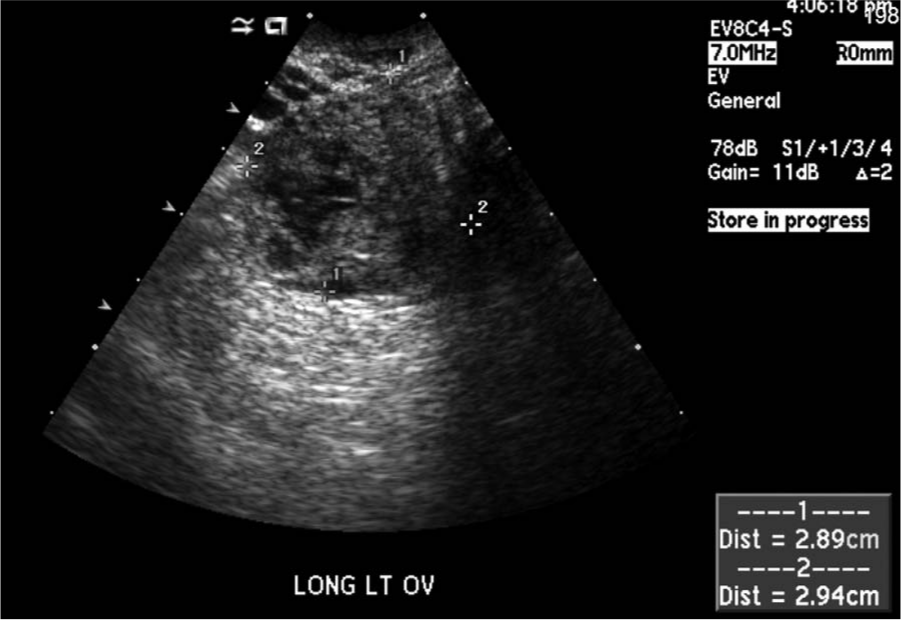
A transvaginal longitudinal image of the ectopic pregnancy next to the left ovary measuring 2.9 × 2.9 cm.
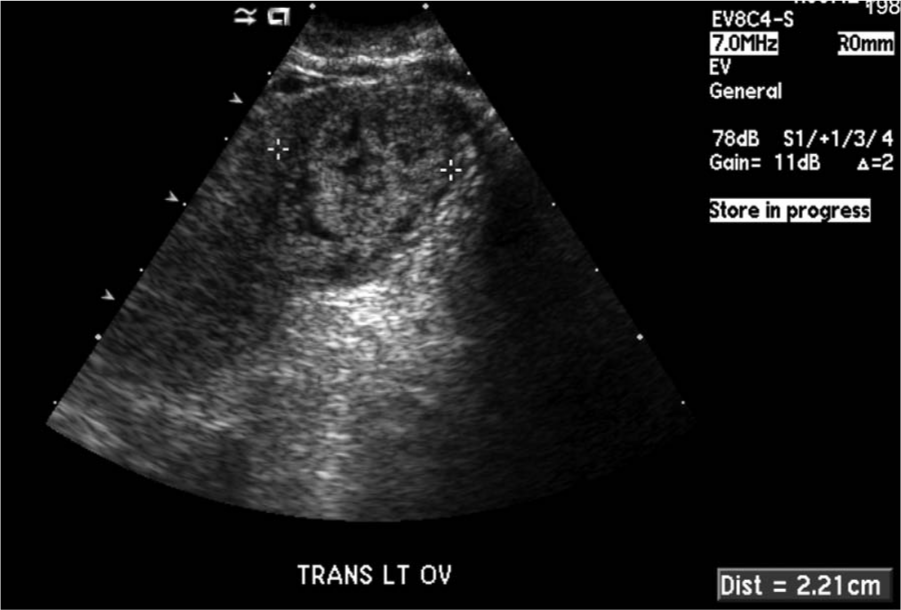
A transvaginal image showing the transverse measurement (2.2 cm) of the ectopic pregnancy next to the left ovary.
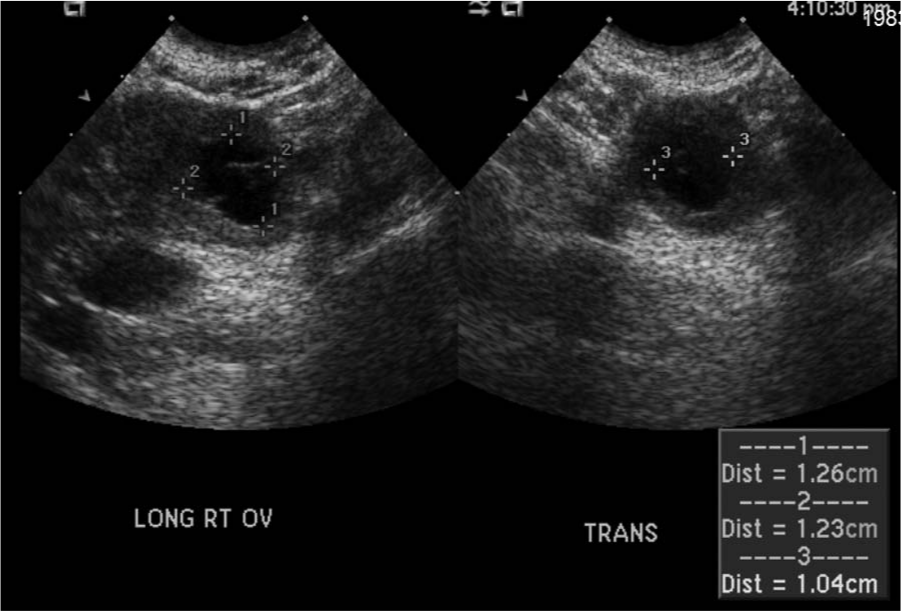
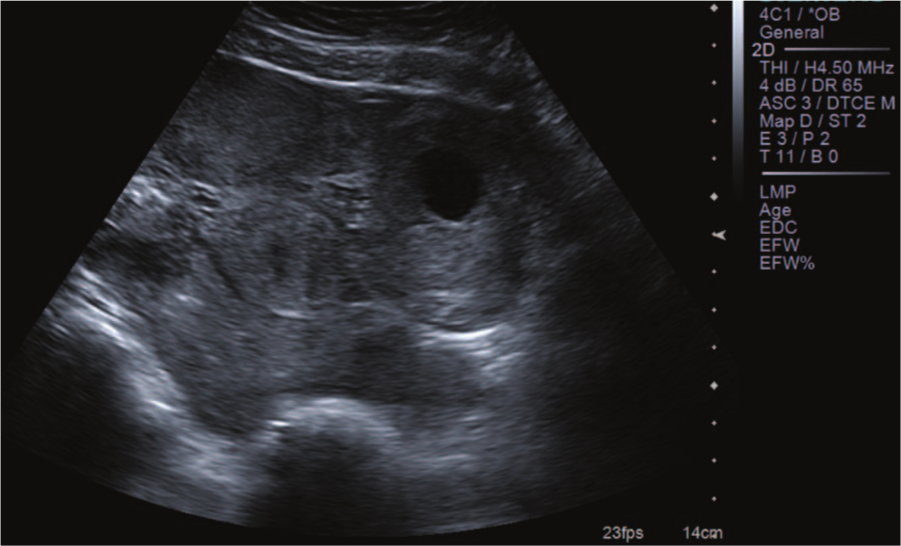
Longitudinal and transverse transvaginal images of the right ovary showing a 1.3 × 1.2 × 1.0 cm cyst.
Options for termination of the ectopic pregnancy were discussed with the emergency department physician and the decision was made to use the medication methotrexate, an inhibitor of the metabolism of folic acid, thus producing a toxic effect on rapidly dividing cells. Four days after this initial diagnosis of an ectopic pregnancy, the B-hCG level remained elevated at 17 608 mIU/mL, despite taking methotrexate. Three days later the level began to decrease to 14 760 mIU/mL. Eleven days after the initial diagnosis, the B-hCG levels continued to decrease to 8313 mIU/mL. One week after this measurement of the B-hCG level, the patient presented again to the emergency department with complaints of increasing lower abdominal pain. She appeared pale, diaphoretic, and was hypotensive; her serum hemoglobin was 10. These findings supported the diagnosis of a possible rupture of the ectopic pregnancy. A bedside sonographic examination was performed and demonstrated a large amount of echogenic material in the pelvis consistent with blood or a hematoma (Figures 9 and 10). The surgeon and emergency department physician were present during the sonographic examination, and the patient was immediately rushed to the operating room for a ruptured ectopic pregnancy with hemolytic shock. At surgery, 2500 mL of bright red and clotted blood was found in the peritoneal cavity. Evidence was found of a ruptured left tubal pregnancy. An area in the left broad ligament and left round ligament was actively bleeding, as well as the cornua of the uterus. The left ovary and fallopian tube were densely adherent into the left ovarian fossa; however, the left ovary could be palpated but never completely visualized. Laboratory evaluation found immature chorionic villi; some were hydropic, and there was minor trophoblastic proliferation. A drain was placed in the posterior cul-de-sac and a large amount of fluid was suctioned out before closure. The patient continued to be hypotensive and was infused with two units of blood in the operating room. The patient was then transferred to the intensive care unit to recover. On the day of the surgery her hematocrit was 33.5 g/dL; it continued to remain low for the next four days at a level of 28.8 g/dL. Her platelet count also remained low for the four days postoperative, ranging from 7.1 fL to 7.4 fL. The patient was discharged seven days after her surgery with no special instructions. The patient returned three days after discharge for blood work where her hematocrit was 34.7 g/dL and the platelet count was 7 fL; no further follow-up was deemed necessary.
A longitudinal transabdominal image of the uterus following the rupture of the ectopic pregnancy.
A transabdominal image of the left adnexa showing the echogenic remains of the ruptured ectopic pregnancy consistent with blood and/or hematoma.
Discussion
The exact etiology of an ectopic pregnancy is unknown and can happen to any female; however, those who have had previous pelvic infections, an IUD, fallopian tube surgery, infertility treatments, or a history of ectopic pregnancies are at increased risk for ectopic pregnancies. 3 The most common site for an ectopic pregnancy is the fallopian tubes; tubal pregnancy occurs with the invasion of trophoblastic tissue within the fallopian tube mucosa. 3 However, ectopic pregnancies also can be located in the ovaries, cervix, or abdominal cavity. 2 The sonographic diagnosis of ectopic pregnancy has improved significantly over the past 15 years as the instrumentation has improved, and it is now the first diagnostic modality used in suspected cases.4-6 Transvaginal sonography has a reported sensitivity of 73% to 93%, with results primarily dependent on gestational age and the experience of the Sonographer.7,8 In the case presented, the Sonographer showed proper visualization of the ectopic pregnancy, for example, the vascular “ring of fire” surrounding the gestation. The Sonographer also showed good visualization of the ruptured ectopic and free blood in the pelvic cavity on the later examination.
The treatments for an ectopic pregnancy are limited; either the patient takes methotrexate if early enough in the pregnancy or has surgery to remove the ectopic and any tissues that may be involved. When detected early, an injection of methotrexate is given to halt the growth of new cells. B-hCG levels are monitored for response, and if the B-hCG level remains high, an additional injection of methotrexate can be given.9,10 Single- or multidose regimens of methotrexate may be used, but multidose regimens have been shown to be significantly more effective in cases of elevated baseline B-hCG levels > 5000 mIU/mL and/or in the presence of fetal cardiac activity. 11 The commonly used criteria for single-dose methotrexate use are a hemodynamic stable patient, an unruptured ectopic mass less than or equal to 5 cm at the greatest dimension on transvaginal sonography, B-hCG level less than or equal to 5000 mIU/ml, no cardiac activity seen, a wish for future fertility, and proper informed consent. 12 Monteagudo et al 13 have shown success with direct ultrasound-guided methotrexate injection, though in a very small series of four tubal pregnancies. More and more women are choosing methotrexate instead of surgical intervention as a way to preserve fertility, though Krag-Moeller et al 14 showed equivalent success rates and subsequent fertility in a randomized, multicenter trial comparing single-dose systemic methotrexate with laparoscopic surgery.
The success of methotrexate has been shown in part to depend strongly on the level of B-hCG when beginning the medication. Lipscomb et al 4 found that 91% of women with ectopic pregnancies who took methotrexate successfully terminated the pregnancy. They found the success rate to be high with B-hCG levels up to 15 000 mIU/mL; above this level the success rate fell to only 68%. Current guidelines suggest a B-hCG level of 5000 mIU/mL as an upper cutoff point for a single-dose methotrexate regimen. 12 In the case presented, the patient’s B-hCG was above this cutoff point for optimal success, and after the initial injection the B-hCG level continued to increase. This case demonstrates a methotrexate failure secondary to elevated levels of B-hCG and illustrates the importance of continued monitoring for complications that may become life threatening, such as rupture, which can lead to shock and hemorrhage.
Conclusion
In the presence of proper clinical history, a definitive diagnosis of an ectopic pregnancy can be based on sonography and a B-hCG blood test. An accurate diagnosis is essential for proper treatment. This case study supports sonography as an indispensable diagnostic imaging modality in gynecologic and obstetric studies.
Footnotes
Acknowledgements
The author would like to recognize the Sonographers who performed the examinations, Stacia Barber, RDMS RVT, and Mary Milberg, RDMS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.