
Abstract
Hepatocellular carcinoma is the most common primary malignancy of the liver, with a poor 5-year survival rate of only 15% to 20%. This article presents a case of a large hepatocellular carcinoma in an essentially asymptomatic young woman in good health. She had no history of any of the traditional risk factors of hepatitis, alcoholism, hepatic fibrosis/cirrhosis, hemochromatosis, or diabetes. Sonographic diagnosis was confirmed by computed tomography–guided biopsy.
Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver and is the fifth most common neoplasm in the world.1,2 It is typically associated with viral hepatitis or cirrhosis.3,4 It is more prevalent in males than in females and is more prevalent after the fifth decade of life. 5 The survival rate is generally poor, with reported 5-year survival rates ranging from 10% to 20%. Treatment options for HCC vary and are usually dependent on tumor size, infiltrative pattern, and vascularity, as well as any evidence of metastasis.2,6,7
Case Study
A young woman in her early 30s presented for an abdominal sonogram to evaluate a feeling of vague fullness in her upper abdomen. She had no pain, nausea, or vomiting. Her appetite was good without weight loss. She had no jaundice, bloating, or fatigue. There was no medical history of hepatitis, alcoholism, hepatic fibrosis/cirrhosis, hemochromatosis, or diabetes. The sonographic examination was performed using a Toshiba Nemio (Tustin, California) ultrasound system using a standard 6.0-MHz curved-array transducer. Imaging of the liver showed a large 15.8-cm heterogeneous, slightly hyperechoic mass involving most of the right lobe and a portion of the left lobe (Figures 1–3). The mass was noted to have moderate internal vascular flow on power Doppler imaging (Figure 4), and some posterior displacement of the inferior vena cave was seen (Figure 5). The hepatic and portal veins were also displaced by the tumor and difficult to image, although no definitive thrombus or tumor invasion was identified. No lymphadenopathy in the porta hepatis or retroperitoneum was seen.
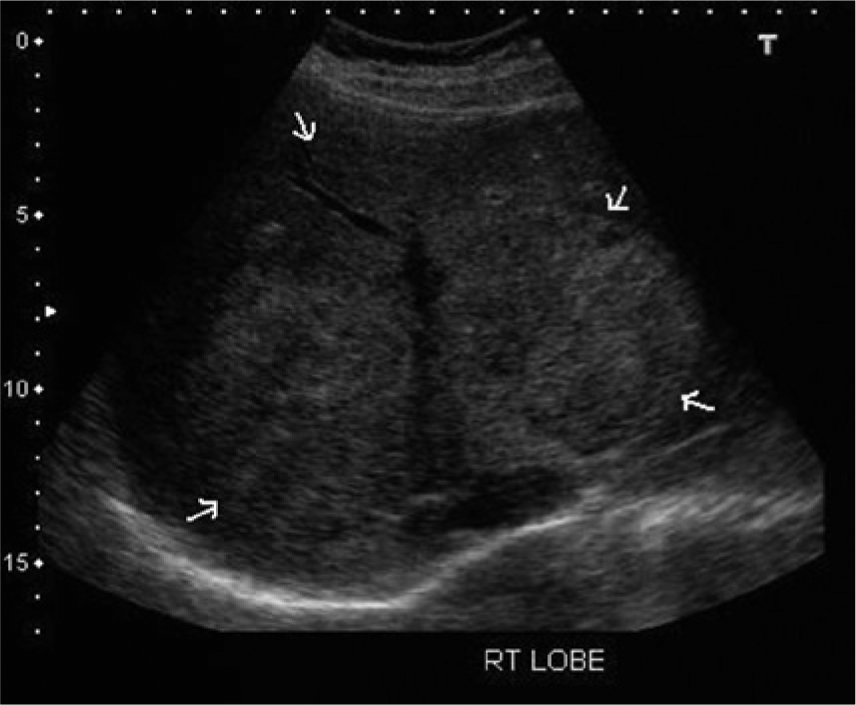
Transverse gray-scale image showing the large heterogeneous, slightly hyperechoic infiltrative mass in the liver.
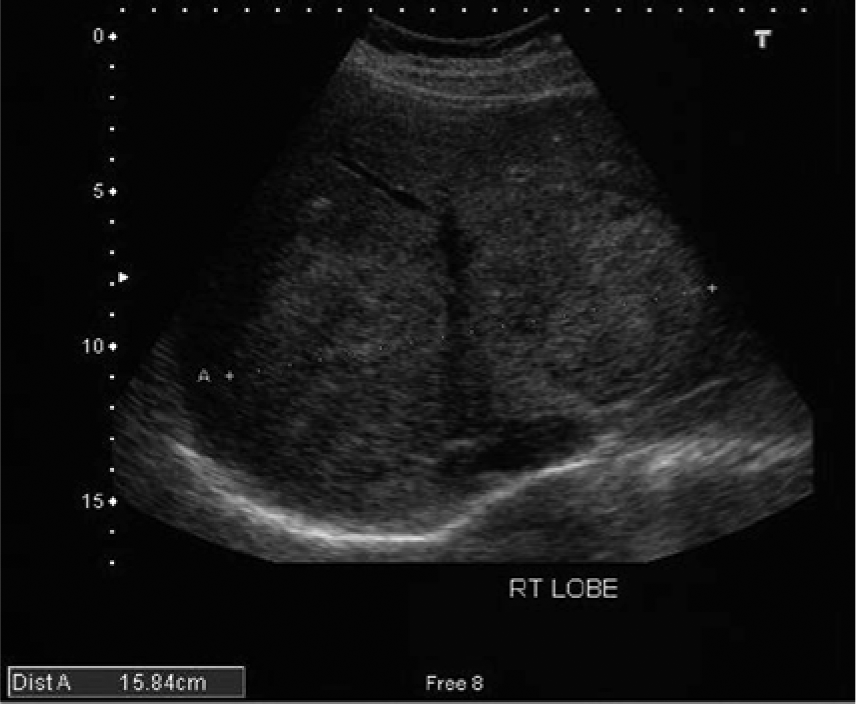
Transverse gray-scale image in the same region with measurement calipers showing a 15.8-cm mass.
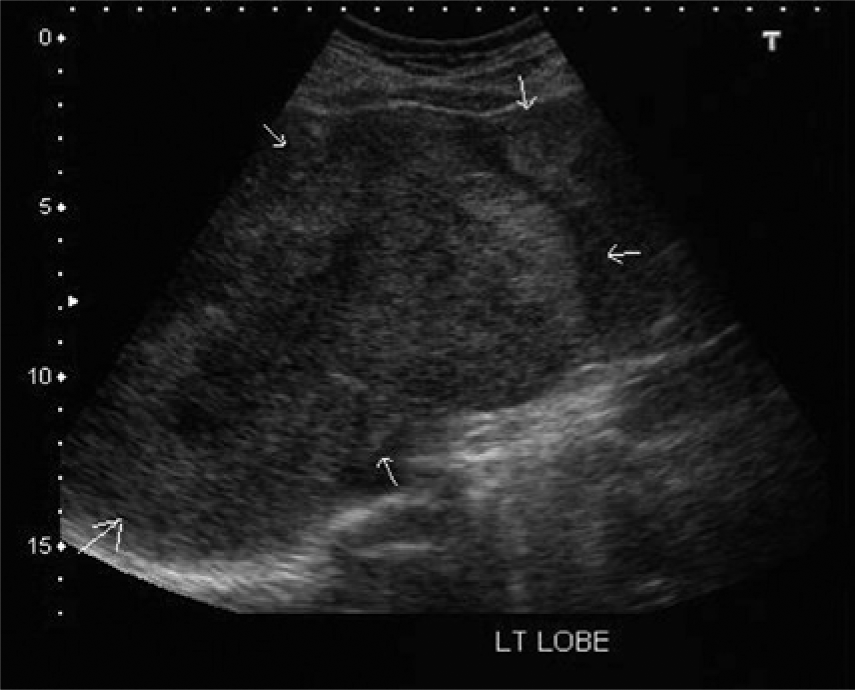
Transverse gray-scale image showing extension of tumor involvement into the medial left hepatic lobe.
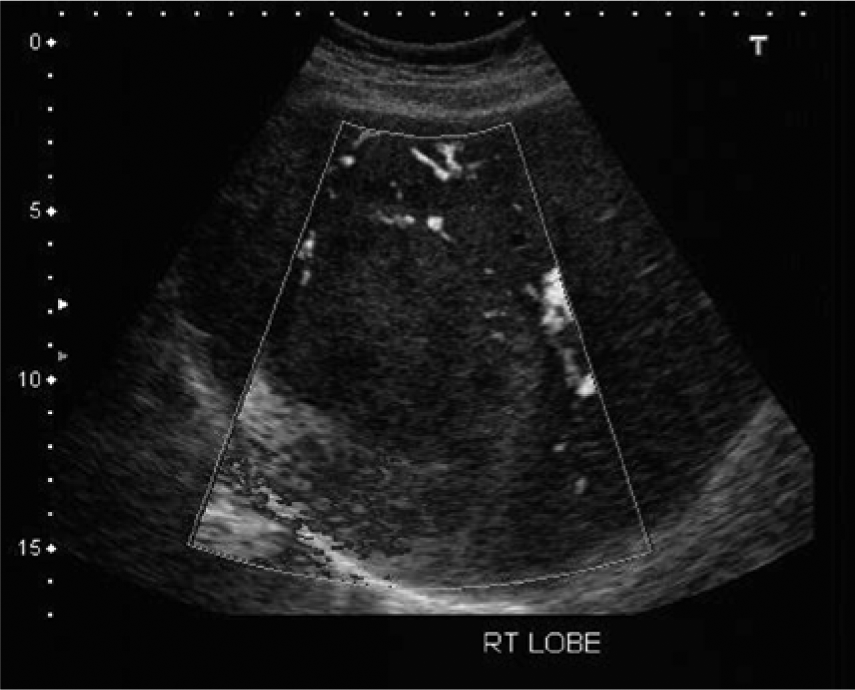
Power Doppler image showing the internal vascularity of the mass.
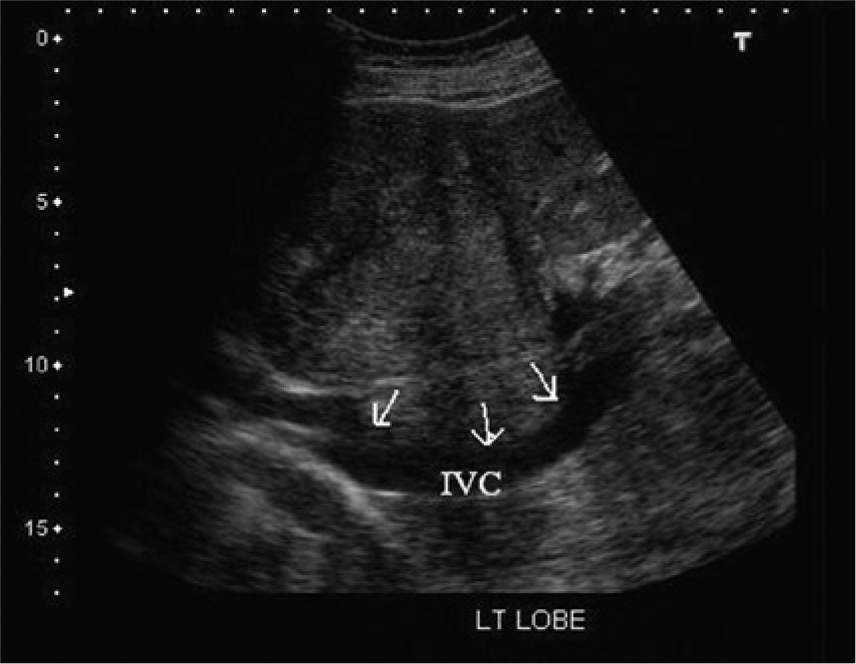
Longitudinal gray-scale image showing the mass and the posterior displacement of the inferior vena cava (IVC).
Follow-up computed tomography (CT) was performed at another facility using a multislice scanner. The precontrast CT showed a large, poorly defined, low-density irregular mass involving approximately three-fourths of the liver (Figure 6). There was early peripheral enhancement of the lesion on the early arterial phase (25 seconds) following contrast injection, with multiple enhancing septa. Imaging at 60 seconds and 5 minutes showed a lack of central lesion filling by contrast, suggesting underlying tumor necrosis (Figures 7 and 8). Contrast-enhanced CT images showed no definitive evidence of portal vein thrombus or tumor invasion (Figure 9). As in the sonographic examination, the hepatic veins were displaced by the lesion and difficult to image. CT-guided needle biopsy was performed at that time, and the suspected diagnosis of hepatocellular carcinoma was histologically confirmed. Because of the extensive and infiltrative involvement of the liver, surgical resection was not considered an option. Despite seeking alternative therapies, the young woman rapidly declined and died five months later.
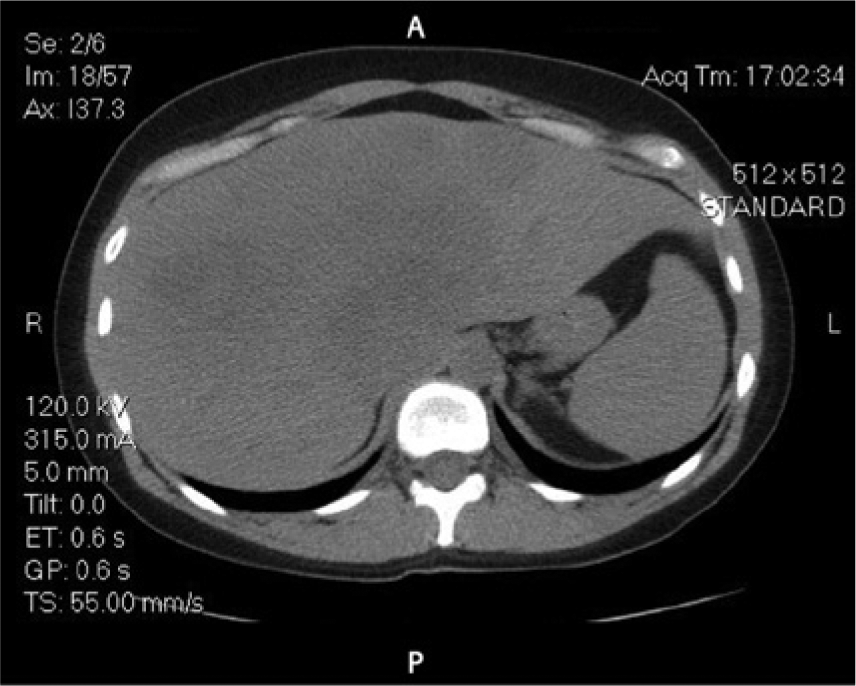
Baseline (precontrast) axial computed tomographic image showing a low-density mass with poorly defined borders involving approximately three-fourths of the liver.
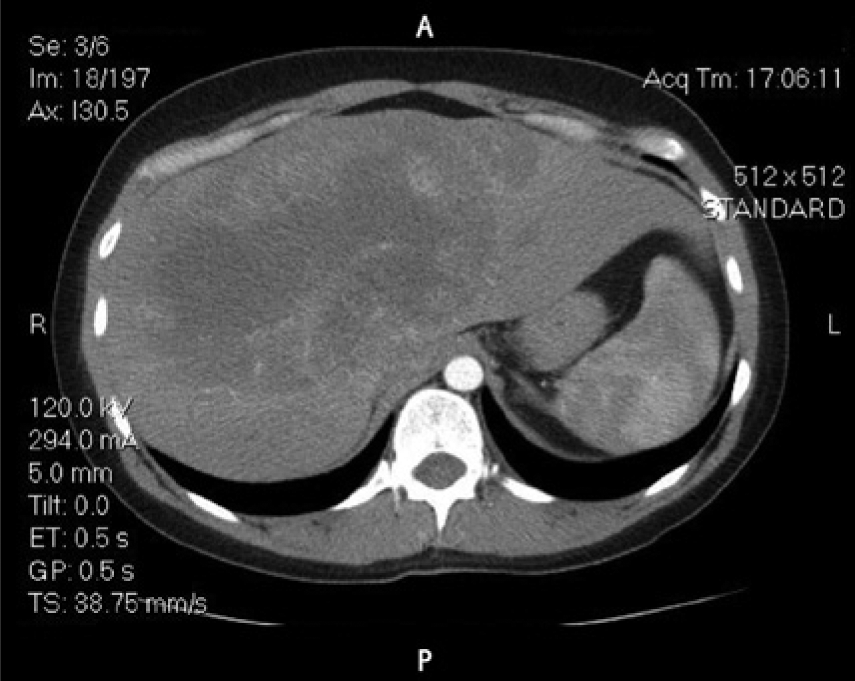
Axial computed tomographic image following contrast injection showing the early arterial phase with some peripheral enhancement of the lesion.
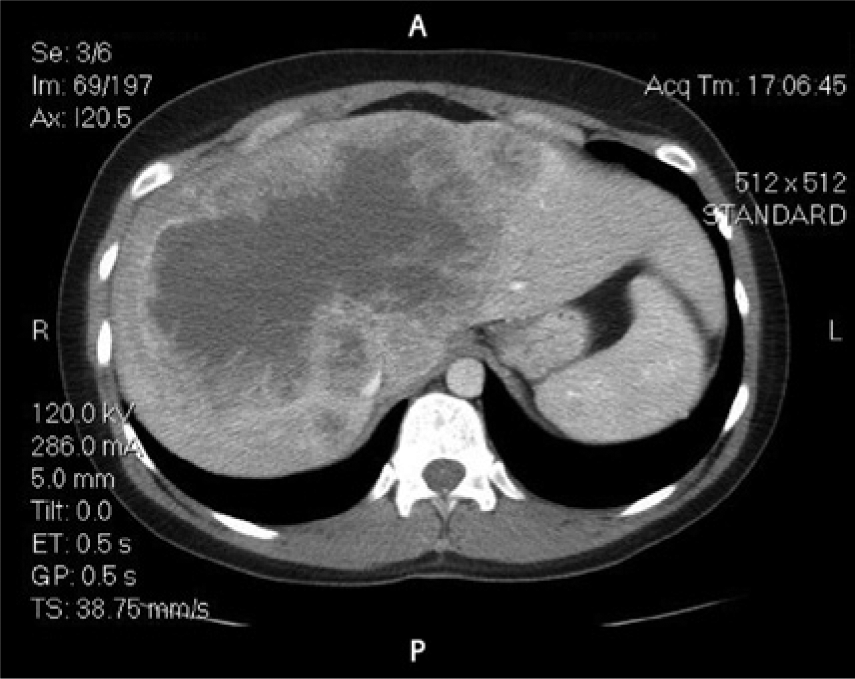
Axial computed tomographic image at one minute following contrast injection showing marked peripheral enhancement of the lesion with no central lesion filling characteristic of necrosis.
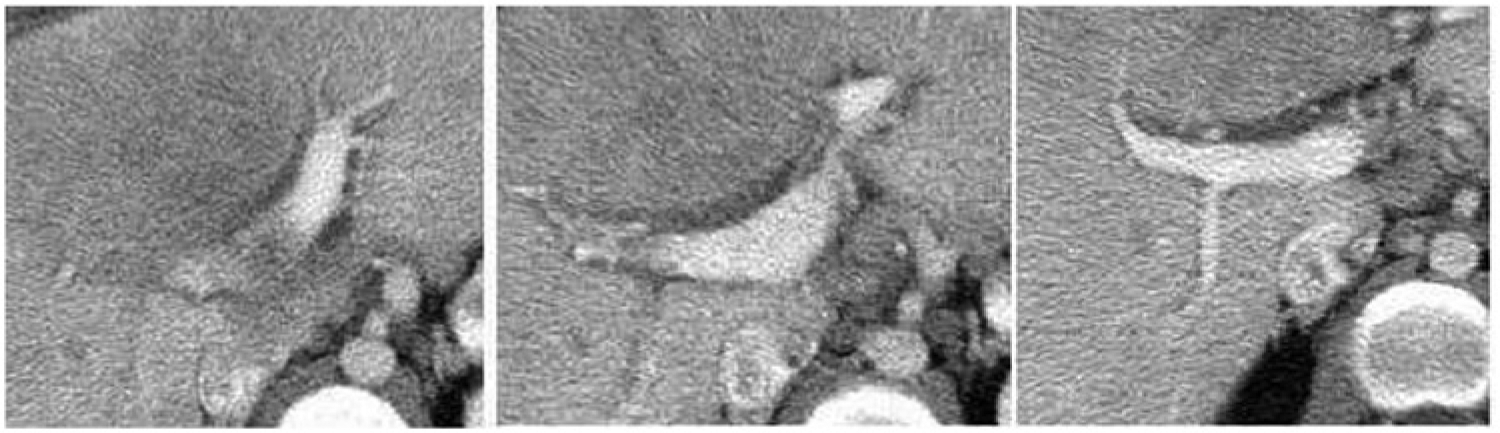
Isolated computed tomographic images of the portal vein following contrast injection showing a widely patent vein with some degree of displacement by the mass but with no evidence of thrombus or tumor invasion.
Discussion
Pathology
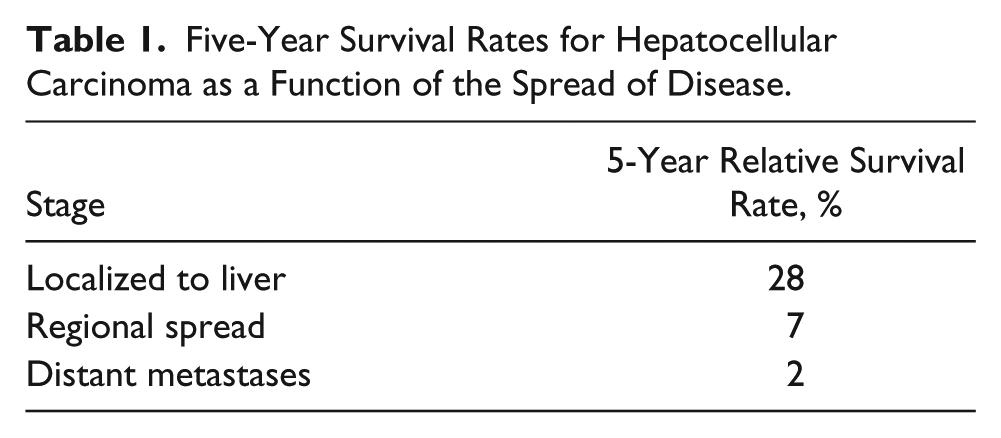
Hepatocellular carcinoma, sometimes referred to as malignant hepatoma, is the most common primary hepatic malignancy.1,2 It is usually associated with chronic viral hepatitis B or C, as well as hepatic fibrosis/cirrhosis (typically secondary to alcoholism). Other risk factors include hemochromatosis, nonalcoholic steatohepatitis, and type 2 diabetes.3,4 HCC affects men more than women and is most common after 50 years of age, although children with biliary atresia, cholestasis, and glycogen storage disease have been shown to be at a higher risk for developing HCC.4–6 Typical signs and symptoms of HCC include abdominal pain, bloating (secondary to ascites), anorexia, weight loss, jaundice, nausea, emesis, and fatigue. 2 The overall 5-year survival rate is approximately 15%, 7 ranging from less than 5% when distant metastases are present to nearly 30% when disease is localized to the liver (Table 1).
Five-Year Survival Rates for Hepatocellular Carcinoma as a Function of the Spread of Disease.
The tumor presentation may include the following:
A single mass
Multifocal masses with or without a tumor capsule
Poorly defined tumor with an infiltrative growth pattern
Treatment options depend on tumor size and number, vascularity, involvement of hepatic vessels, the presence of a tumor capsule, and the presence of metastatic disease.2,6,8 These treatment options include the following:
For early-stage disease localized to the liver with preserved liver functions
2
:
Surgical resection (partial hepatectomy) Percutaneous ethanol injection Radiofrequency ablation Cryoablation Liver transplantation
For mid-stage disease in patients who are not candidates for partial hepatectomy
2
:
Cryoablation Arterial chemoembolization Liver transplantation
For late-stage disease with distant metastases
2
:
Chemotherapy
Imaging Features
HCC can be a challenging disease to identify and image in its earliest stages. It may present as a single mass or multiple small masses. The early lesions in particular can appear similar to small hemangiomas, early metastatic disease, or focal nodular hyperplasia. Historically, the most commonly used imaging modality to follow high-risk patients has been CT. However, with increasing concerns regarding radiation exposure, sonography is becoming more prevalent as the primary imaging modality.7,9,10 While magnetic resonance imaging (MRI) has demonstrated high-contrast resolution and may detect lesions less than 1 cm in diameter, the associated high costs have limited the use of this modality.11,12
Sonographically, HCC has varied image characteristics depending on the individual lesion, its size, and background liver echogenicity; if the lesion is diffuse throughout the liver, it may be difficult to identify or distinguish from cirrhosis. A focal HCC typically will appear somewhat hypoechoic compared with normal liver; as lesions become larger, they tend to become more hyperechoic and heterogeneous due to fibrosis, fatty changes, necrosis, and calcification. A peripheral halo of hypoechogenicity, or pseudocapsule, may be seen.13,14 With technologic advances in sonography providing improved resolution and gray-scale image quality, small lesions can be more effectively identified. Furthermore, it can evaluate vascular invasion of the portal and hepatic veins with standard imaging as well as color and power Doppler imaging. Sonography can also be very helpful in providing frequent serial imaging for surveillance and evaluation of treatment efficacy, as well as guidance for needle biopsy and percutaneous treatment procedures.9,10,15–17
Conclusion
This case report demonstrates a rare presentation of hepatocellular carcinoma in an essentially asymptomatic young woman without any of the typical risk factors usually associated with this disease. Given the advanced stage of the tumor when discovered, unfortunately few treatment options were available. As image quality and system capabilities of sonography continue to improve, sonography may achieve equal footing with CT and MRI as the initial imaging modality for HCC given the increasing attention to the radiation risks of CT and the relatively high cost of MRI. Sonography has already demonstrated its value and usefulness in serial imaging for the evaluation of treatment efficacy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.