
Abstract
Portal vein tumor thrombus (PVTT) is a complication of liver disease, specifically hepatocellular carcinoma (HCC). It occurs secondary to direct invasion of tumor into the portal venous system. PVTT is associated with a poor prognosis, therefore identification and differentiation of malignant from benign thrombus is very important in the treatment of the patient. Sonography can be a useful tool in the detection of malignant thrombus.
Keywords
Introduction
Cirrhosis and hepatitis C commonly predispose patients to end stage liver disease, and these patients have a greater chance than the general population of developing hepatocellular carcinoma (HCC) and portal vein tumor thrombus (PVTT).1–3 PVTT is a primary malignant tumor that directly invades the portal venous system. 1 This case report discusses presumed PVTT in a patient with extensive liver disease including cirrhosis, hepatitis C, and HCC. It also examines the use of sonography to diagnose PVTT and some technical parameters to be aware of when performing the examination.
Case Report
A patient in his 50s with a history of liver disease presented to the emergency department. Upon arrival, the patient’s chief complaint was severe abdominal distention, abdominal pain, and melena. The patient had an extensive past medical history, which included cirrhosis with end stage liver disease due to hepatitis C and alcohol abuse, HCC, upper gastrointestinal (GI) bleeding, hypertension, gastroesophageal reflux disease (GERD), and inferior vena cava (IVC) thrombus. The patient’s prior medical care took place at a different facility, but his available medical records showed his last drawn α-fetoprotein was 697 ng/mL.
While in the emergency department the patient developed an upper GI bleed with hematemesis. He was admitted to the medical intensive care unit for monitoring and treatment. The patient subsequently underwent an upper GI endoscopy and was found to have Grade 1 esophageal varices, a small hiatal hernia, and clotted blood in the gastric fundus. This was treated with 3 mL of a 1:10,000 solution of epinephrine for hemostasis.
An abdominal sonogram with Doppler was ordered to evaluate the liver cirrhosis and ascites. The sonogram was performed on a Philips iU22 ultrasound machine using a C5-1 curvilinear probe. The resulting images demonstrated IVC thrombus, portal hypertension with retrograde flow in the main portal vein, enlargement of the left portal vein with nonocclusive thrombus, and an abundant amount of ascites. While there were no discrete liver masses identified on the ultrasound images, the thrombus within the left portal vein contained arterial flow and was therefore presumed to be malignant thrombus (Figures 1-4). The remainder of the sonogram was normal, except for an incidentally noted gallbladder polyp.

Longitudinal image of left lobe of the liver showing an enlarged left portal vein containing thrombus within the lumen.
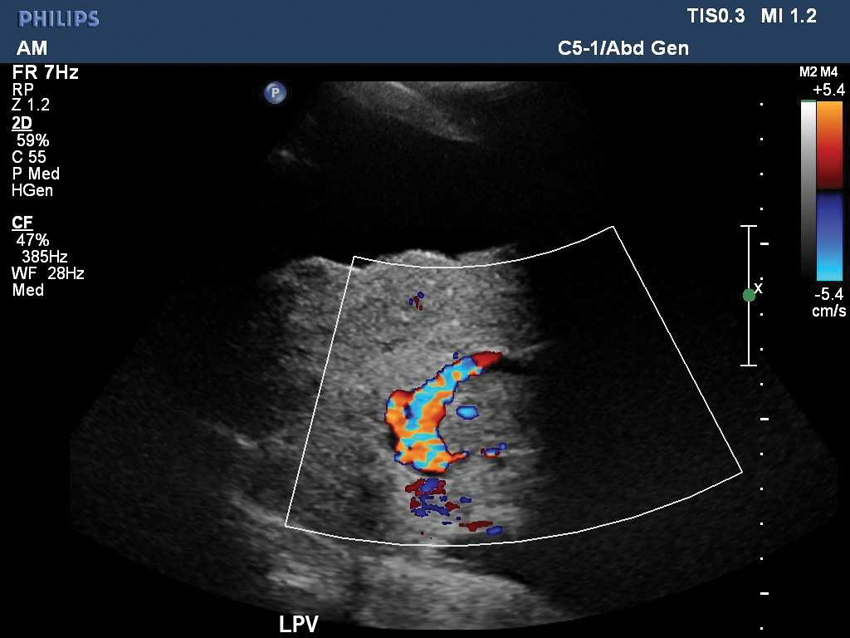
Color Doppler image of the left portal vein showing flow around and within the thrombus.
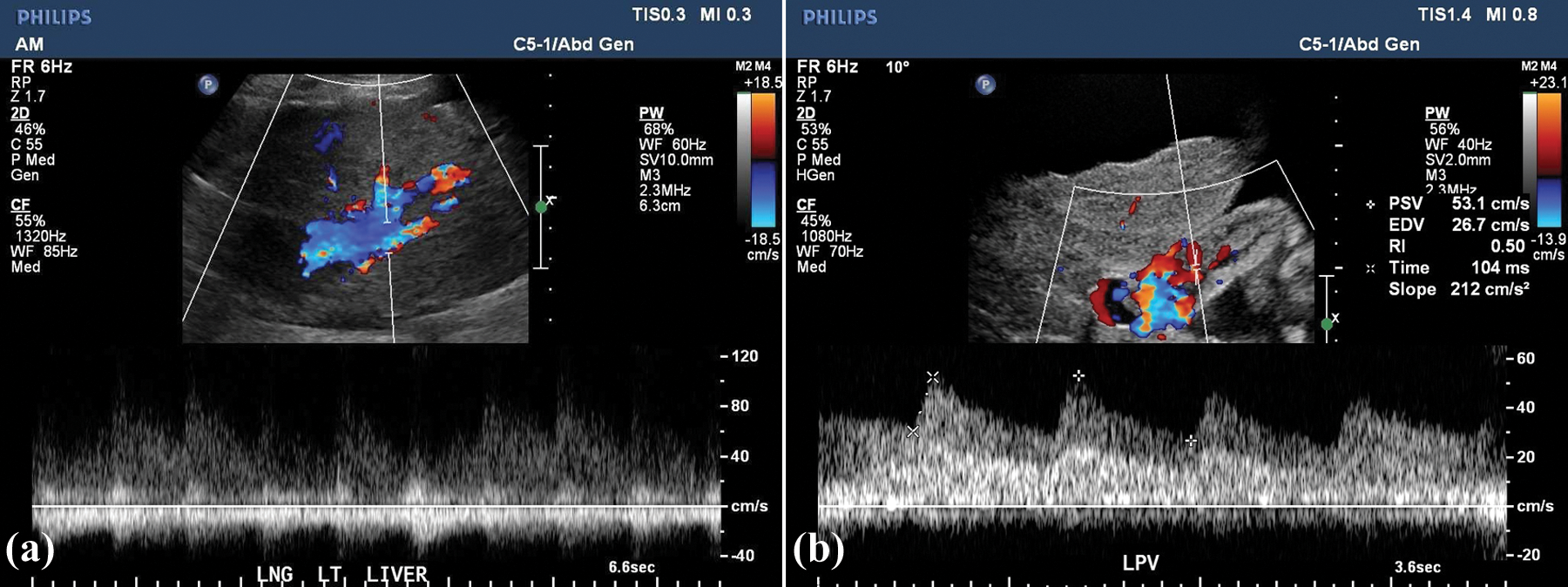
Spectral Doppler of the left portal vein from two sites (a, b) confirming pulsatile flow within the thrombus. (Note the smaller sample volume and reduction in Doppler gain in 3b compared to 3a.)
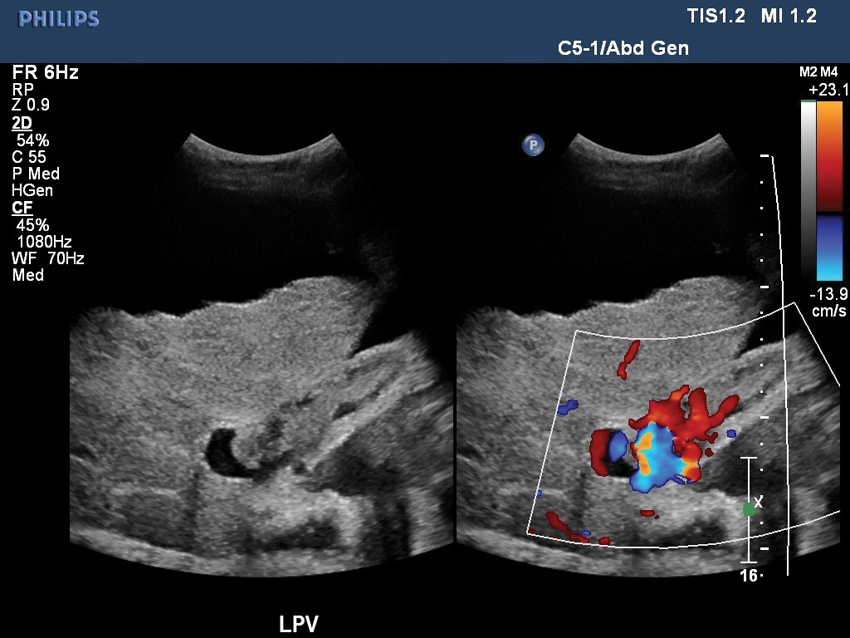
A dual image taken simultaneously of a longitudinal left portal vein with and without color Doppler showing flow around and within the thrombus.
The findings on the abdominal sonogram prompted the radiologist to recommend an abdominal computed tomography (CT) scan for further evaluation of the liver. Since the patient’s prior outside imaging had already deemed him not to be a suitable liver transplant or surgical candidate, he and his family decided not to undergo any further imaging. Palliative care was initiated and the patient was transitioned to comfort care with hospice. Further follow-up was not available on this patient.
Discussion
Liver disease consists of a broad spectrum of clinical symptoms and the sonographic findings are often varied. Portal vein tumor thrombus is defined as the invasion of primary malignant tumor into the portal venous system. 1 PVTT is typically associated with patients who have liver disease, and it is more common in people with cirrhosis, hepatitis C, and hepatocellular carcinoma.1–3
The World Health Organization defines cirrhosis as a diffuse process characterized by fibrosis and the conversion of normal liver architecture into structurally abnormal nodules. 4 The risk of HCC rises markedly in the setting of hepatitis C and cirrhosis.5–7 This increased risk of malignancy may depend on the etiology and the duration of the cirrhotic process. 4 Cirrhosis therefore is often considered a premalignant condition. 7 Clinical findings, such as an α-fetoprotein level greater than 400 ng/ml, is generally considered diagnostic of HCC. 8 Imaging studies such as CT, magnetic resonance imaging (MRI), and sonography are often used in combination with clinical information to confirm the diagnosis of HCC.1,3,9,10
Hepatitis is a general term for inflammation of the liver. Hepatitis C is caused by infection with the hepatitis C virus (HCV) and affects millions of people worldwide. HCV infects the hepatocytes and causes inflammation of the liver, often with long-term complications. According to the World Health Organization, about 40% of people exposed to HCV will recover, with the remainder becoming chronic carriers. Chronic hepatitis is defined as continuation of the disease without improvement for at least six months. 11 Of those diagnosed as chronic carriers, 20% develop cirrhosis. Of those with cirrhosis, up to 20% will develop liver cancer, as was the case with this patient.
Portal vein thrombosis (PVT) may be benign or malignant. Benign PVT usually results from portal hypertension and venous stasis, whereas malignant PVT occurs by direct invasion of HCC into the portal venous system. 1 PVTT often leads to tumor spread throughout the liver. It may also result in increased portal venous pressure and decreased portal flow, which in return may cause ascites, jaundice, hepatic encephalopathy, and ultimately liver failure. 12 PVTT is associated with a poor prognosis. Treatment of these patients is not curative, but may extend their life expectancy by about two years. Without treatment the average survival is approximately two to four months.12,13 The treatment of patients with HCC and PVTT is complicated. Many patients are not surgical candidates due to the cirrhotic changes and dissemination of the tumor throughout the liver. 13
Imaging studies such as CT, MRI, and sonography are able to differentiate between benign and malignant thrombus by identifying an underlying malignancy.1,10 There have been multiple studies performed to determine the accuracy of use of ultrasound Doppler on malignant thrombus.1,3 Sonography may be an important screening tool for PVTT, with the use of additional imaging modalities to confirm the diagnosis. 14
A study by Dodd and colleagues found that the detection of pulsatile flow within portal thrombus had a specificity of diagnosing malignant PVT approaching 100%. 1 While diagnosing PVTT with only one imaging modality is limited, a Japanese study by Ishida et al., performed on patients with gastrosintestinal cancer, diagnosed all seven of their patients successfully only with color Doppler sonography. 15 Demonstration of direct invasion of the tumor thrombus into the portal vein along with intrathrombus neovascularity are both characteristics used to differentiate benign from malignant thrombus. 10 However, it is really the identification of an underlying hepatic tumor, specifically HCC, or an invasive procedure leading to a tissue diagnosis that will confirm the findings of malignancy.
While color Doppler sonography can be useful in diagnosing PVTT, it is important that the sonographer use appropriate technical parameters to obtain the images. The use of a small spectral Doppler sample volume will ensure that the waveform is only representing the area of interest and not including surrounding vessels, such as the adjacent hepatic artery, while trying to document portal tumor flow, as in this case. (Note the difference between Figure 3a and 3b.) The use of low Doppler gain will reduce artifact on the image, which may be mistaken as true flow. The ability of the patient to cooperate during the procedure is also very important. While not always possible in this patient population, it is ideal if the patient is alert and able to hold their breath for the spectral and color Doppler sample to prevent motion and sampling of adjacent structures.
Conclusion
Liver disease complicated by portal vein tumor thrombus has a very poor prognosis. Sonography is a useful modality in differentiating benign from malignant thrombus. Correct diagnosis will determine treatment options as well as prognosis.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.