
Abstract
Skin perfusion pressure (SPP) is a noninvasive diagnostic test that quantitatively analyzes the local blood flow in an area of interest. SPP is measured using a laser Doppler sensor that is placed under an inflated/deflated blood pressure cuff and is able to detect red blood cell motion in the microcirculation as the cuff pressure passes through systole. The SPP results can be used in conjunction with physiological arterial testing to aid in the diagnosis of critical limb ischemia. The examination also can be a guide in determining the most advantageous level for amputation in patients with critical limb ischemia. SPP provides a measure of the potential for healing or progression of a wound without revascularization.
Keywords
Skin perfusion pressure (SPP) is a noninvasive diagnostic test that quantitatively analyzes the local blood flow in an area of interest by measuring the systolic pressure in the microcirculation. Knowledge of the blood flow characteristics in the microcirculatory system can assist in the assessment of peripheral arterial disease (PAD), critical limb ischemia, and determination of an appropriate level of amputation. It provides quantitative data on the need for lower limb revascularization and the potential for healing of lower extremity ischemic ulcers and skin incisions following arterial reconstructive surgery or amputation.1–4 Typically, once critical limb ischemia is diagnosed, 20% of cases result in tissue loss or unresolved pain in the first year, 30% of patients are at risk for a major (below-knee or above-knee) amputation, and there is a 25% one-year mortality rate.5,6 To avoid these complications, examination of both the macrocirculatory and microcirculatory systems is crucial.7–9 This is particularly true in diabetic patients; there are approximately 16 million diabetic patients in the United States with PAD, of whom 15% will develop foot ulcers leading to limb amputation.8,10
There is a specific technique for the use of the SPP system. 11 SPP uses a laser Doppler sensor that is placed in close proximity to the area of concern (often a nonhealing wound) with a temporary adhesive (Figure 1). Unlike photoplethysmography, which detects the intensity of light scattered from red blood cells, the laser Doppler sensor determines the presence of a Doppler frequency shift generated by the motion of the red cells. With the patient in a supine position, a blood pressure cuff is wrapped over the laser sensor on the patient’s leg, digit, or foot (Figure 2). The cuff is inflated to a pressure above systolic in the microcirculation (typically 90 mm Hg); the pressure is held for 10 seconds or longer, until the volume flow indicator reads below 0.1%. At this point, cuff pressure is slowly reduced at a rate of 10 mm Hg every 5 seconds. The return of microcirculatory flow is indicated by a doubling of the volume, a measure of the percentage of moving red blood cells, over the occlusion baseline. The corresponding cuff pressure is used to indicate SPP. A graphical recording is supplied that shows the cuff pressure (x-axis) versus the detected red blood cell motion or perfusion (y-axis) (Figure 3).

Placement of the laser Doppler sensor and pressure cuff to measure skin perfusion pressure.

A skin perfusion pressure test being performed on the plantar aspect of the foot.
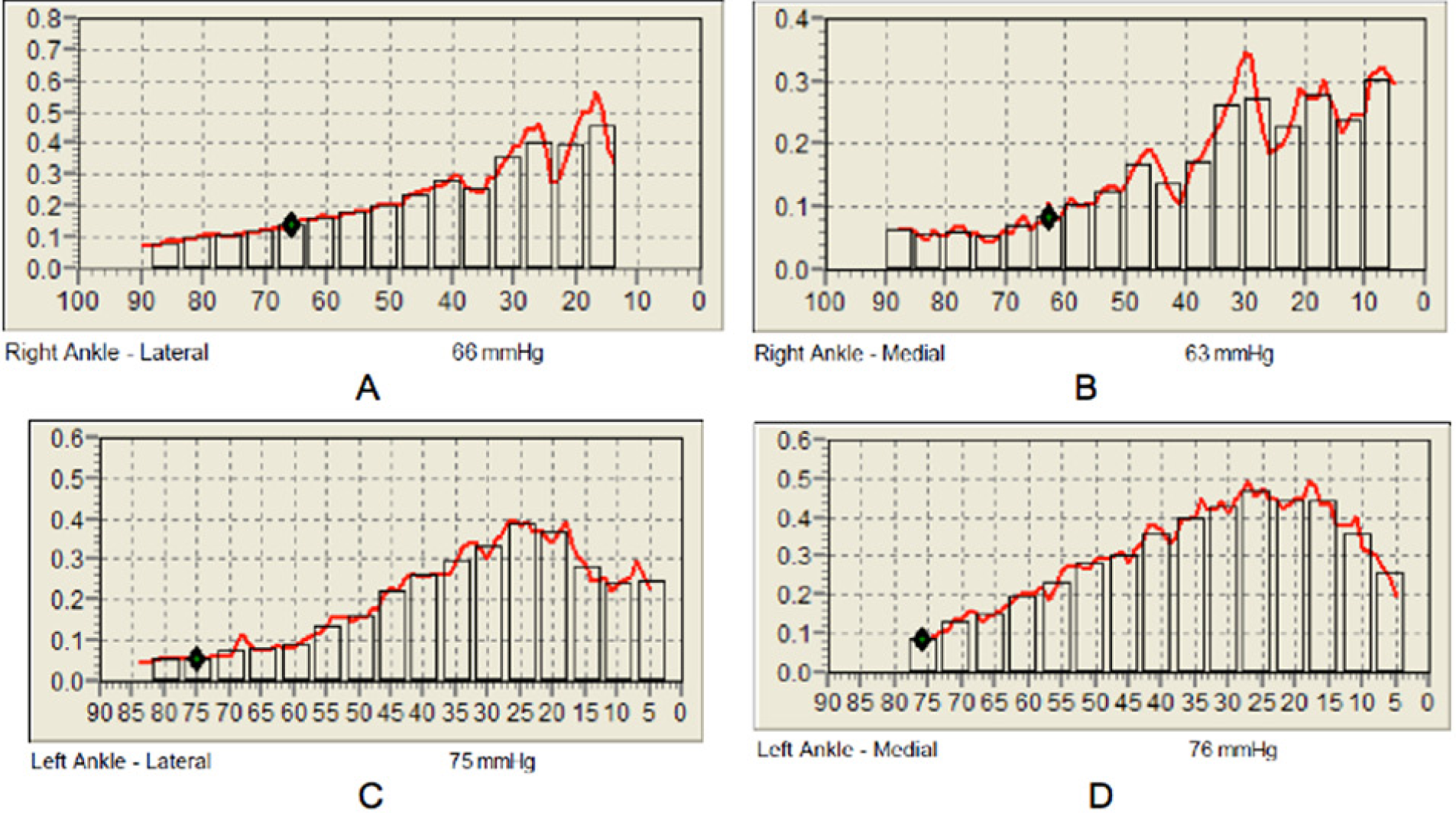
Results of a skin perfusion pressure test. (A) Right lateral ankle measuring 66 mm Hg. (B) Right medial ankle measuring 63 mm Hg. (C) Left lateral ankle measuring 75 mm Hg. (D) Left medial ankle measuring 76 mm Hg.
Normal SPP for a healthy adult indicates no compromise to perfusion and will range between 50 and 100 mm Hg.1–3 Marginal ischemia, with limited potential for wound healing, will range between 30 and 50 mm Hg. Such a patient may also experience symptoms of PAD such as limiting claudication. In patients with critical limb ischemia, the pressure will measure less than 30 mm Hg, and the prognosis for wound healing and limb salvage is poor without arterial revascularization.
Case Study
A male in his seventh decade presented to the vascular laboratory with a nonhealing wound on his medial right ankle. His history was significant for smoking (previous) and hypertension. Initially, the patient had a physiologic arterial examination that included an ankle brachial index and segmental pressures. These test results were consistent with peripheral arterial blood flow (macrocirculatory) within normal limits. Because of the presence of the ulceration, a skin pressure perfusion examination was done in conjunction with physiologic arterial testing to evaluate blood flow in the microcirculatory system. The sonographer performed the SPP examination on the right ankle and a comparative study on the left ankle. The test was performed using a Sensilase Skin Perfusion Pressure System (Väsamed Incorporated, Eden Prairie, Minnesota).
The examination showed normal flow at the level of the ankles bilaterally. The lateral right ankle measured 66 mm Hg and the medial right ankle measured 63 mm Hg. The left lateral ankle measured 75 mm Hg and the left medial ankle measured 76 mm Hg (Figure 3). Based on this range of pressures, the patient’s ability to heal should not be limited by ischemia secondary to PAD.
Discussion
Skin perfusion pressure has been shown to be an important measurement in making clinical decisions for the patient with PAD and a predictive tool to identify the likelihood of wound healing.12–14 The examination allows for the measurement of any site with viable tissue: the digits, dorsum and plantar aspects of the foot, ankle, calf, lower thigh, over calcified arteries, and near sites of necrotic or edematous tissue. If the toe pressure cannot be measured, Tsai et al 14 have shown that the SPP of the foot has a strong correlation and can be substituted.
SPP can be correlated with other tests commonly used to assess for PAD, such as the noninvasive ankle-brachial index and pulse volume recordings, or with more invasive tests such as computed tomographic angiography, magnetic resonance angiography, and digital subtraction angiography. The addition of SPP to any of these tests, all of which evaluate macrocirculatory obstructive disease, provides a very site-specific measure of the impact of macrocirculatory obstruction on microcirculatory flow. 15 Clinically, Castronuovo et al 3 showed that SPP can accurately diagnose critical limb ischemia in 80% of patients. For the assessment of wound-healing potential, SPP has been shown to be an accurate screening tool.4,12
There are some limitations to the application and efficacy of the measurement of SPP, which may be due to the patient, vascular sonographer, equipment, or the environment. Patient voluntary or involuntary movement and pressure tubing movement will cause significant artifacts in the recorded data. Although the total time for the examination is typically less than 20 minutes, patients with critical ischemia may find it difficult to hold completely still for that amount of time. It is necessary for the test that a blood pressure cuff be wrapped around their limb, and patients must be able to tolerate this procedure. Care also must be taken to avoid any bony prominences, major veins, or varicosities when placing the cuff since any of these may induce artifacts. Careful attention to technique must be given for reliable and reproducible measurements. When repeated measurements are taken, the sensor position must be precisely duplicated to the original measurement site. The testing environment must also be as controlled as possible to get an accurate reading. In particular, the room must be quiet with a comfortable temperature to avoid any stressors that might induce vasoconstriction. Since the laser Doppler sensor uses transmission of light for red blood cell detection, the ambient light in the room should be reduced. In addition, the patient should prepare for the examination by avoiding caffeine, alcohol, smoking, vigorous exercise, and salty foods at least 24 hours before the examination.
Conclusion
This case study demonstrates the use of SPP as an effective and practical way of evaluating the potential for healing of a chronic wound. When testing patients with suspected critical lower extremity ischemia, more vascular laboratories may want to consider incorporating this physiologic study into their protocols.
Footnotes
Acknowledgements
I would like to dedicate this article to my parents and friends, who have supported me during my journey through the Diagnostic Medical Sonography program. A special thanks is directed to Hal Pitts, MBIS, who has been a dedicated dad and physics instructor during the DMS program. I would like to thank the sonographers at Heart and Vascular at Texas Health Presbyterian Hospital Dallas for obtaining the clinical images presented in this article. Special thanks to Lynn Schluns, RDMS, RVT, the Coordinator of Diagnostic Medical Sonography at El Centro Community College in Dallas, Texas, for providing outstanding instruction, assisting in the preparation of the article, and encouraging me to submit this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.