
Abstract
Bladder exstrophy is a rare congenital abnormality where the urinary bladder, anterior pelvis, and genitalia fail to close in the midline, resulting in the bladder being located externally along the anterior pelvic wall. The incidence is 1 per 40 000 live births and has a male predominance. Common prenatal sonographic findings include an absent urinary bladder, normal amniotic fluid, and an inferior abdominal mass. The absence of the bladder in the second trimester with normal amniotic fluid volumes should prompt evaluation for this abnormality. Advances in ultrasound technology including the use of 3D and 4D imaging have led to an increase in prenatal diagnosis of this condition. The earlier diagnosis has aided in delivery at an appropriate center and timely surgical planning, allowing for a better outcome.
Keywords
Introduction
Bladder exstrophy is a rare congenital abnormality that can be difficult to diagnose prenatally and should be considered in the absence or nonvisualization of a urinary bladder on routine obstetrical sonographic examination. 1 This case study confirms the need for careful evaluation during routine obstetrical sonography when the bladder cannot be visualized. Detailed sonographic evaluation, 3D ultrasound, and magnetic resonance imaging (MRI) may all aid in prenatal diagnosis and postnatal surgical planning.
Case Report
A young woman, gravida 2, para 1, was referred through our genetics department at a gestational age of 20 weeks and 2 days following an anatomic survey at an outside location in an otherwise uncomplicated pregnancy. Outside sonographic findings suggested a thickened umbilical cord, absent urinary bladder, enlarged female genitalia, and echogenic bowel with normal amniotic fluid and appropriate growth. Prior sequential serum screening gave a risk of 1 in 10 000 for Trisomy 21 and a risk of 1 in 10 000 for Trisomy 18.
A detailed obstetric sonographic examination was performed using a GE Voluson 730 Expert (General Electric, Milwaukee, Wisconsin) imaging unit with a curvilinear 3D RAB 4-8P transducer. Sonographic findings included fetal biometry consistent with the patient’s last menstrual period dating, normal amniotic fluid, and normal fetal kidneys. An absent urinary bladder (Figure 1), an anterior abdominal wall mass inferior to the cord insertion, a low-set abdominal umbilical cord insertion, a small penis, and a widened scrotum (Figure 2) were all noted, consistent with bladder exstrophy. 3D imaging (Figures 3A and 3B) aided in the diagnosis as well as increased the patient’s understanding and conceptualization of the fetal condition. Findings and diagnosis were discussed with the patient, and she elected to undergo repeat sonography in 2 weeks as well as a pediatric urology consultation and referral to a center specializing in exstrophy care. Findings remained consistent at four subsequent sonograms. Fetal MRI for surgical planning at the exstrophy center confirmed the sonographic findings but was limited by fetal position.

Transverse cross-sectional image of the fetal pelvis showing an absent urinary bladder and two umbilical arteries, as well as a wide-set umbilical cord.

Mid-sagittal image of the fetal abdomen and pelvis showing a low-set umbilical cord insertion and an anterior abdominal wall mass.
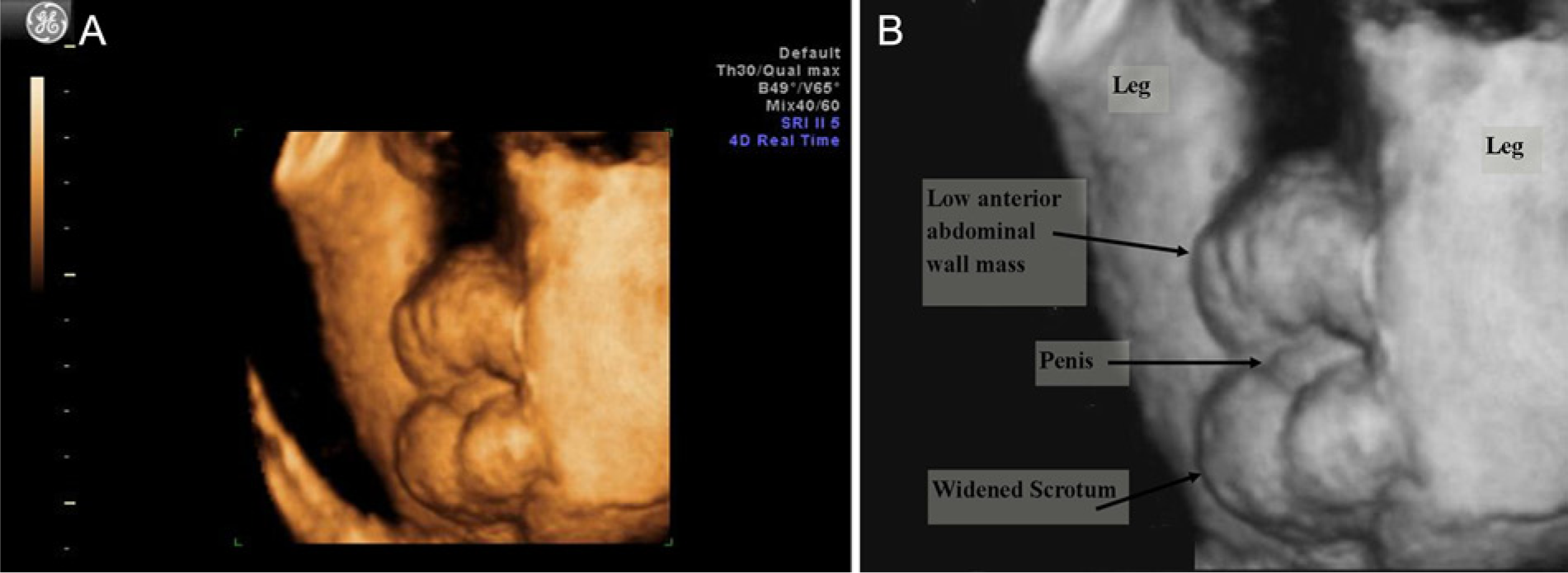
(A) 3D colorized image of the scrotal region. (B) Gray-scale rendering of the same 3D image with the widened scrotum, small penis, and abdominal wall mass labeled.
The patient underwent induction of labor at 41 weeks gestation, delivering a male neonate weighing approximately 4100 grams. Findings at birth confirmed the prenatal diagnosis, including an external urinary bladder inferior to the umbilicus and a bifid penis (Figure 4). The neonate underwent his first reconstructive surgery 2 days post-delivery and received an additional 5 weeks of hip traction. Epispadias, a malformation in which the urethra ends in an opening on the dorsum of the penis, was also noted at the time of delivery and a staged surgical correction will be done after 1 year of age.
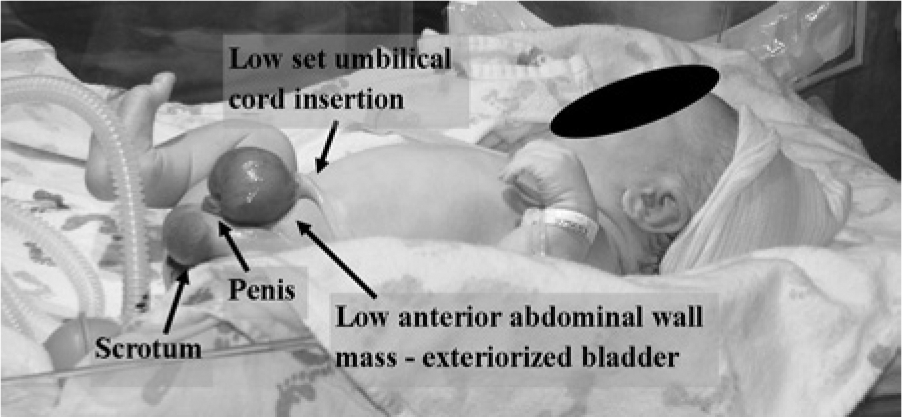
Photograph of the neonate showing the findings (labeled) consistent with the 3D sonographic imaging shown in Figure 3.
Discussion
Bladder exstrophy (also known as ectopia vesicae) is a congenital abnormality where the urinary bladder is everted and located on the outside of the body instead of within the fetal pelvis, due to incomplete closure of the abdominal wall. 2 It appears as a nondistended solid mass on the fetal abdomen versus the cystic appearance that it normally has within the pelvis. This occurs because the ureters empty directly into the amniotic cavity, preventing the bladder from filling. Sonographic diagnosis may be limited by fetal position but should be suspected in a fetus when a urinary bladder is not visualized in the presence of normal appearing kidneys and amniotic fluid volume. Other findings common with classic bladder exstrophy include a low-set umbilical cord, epispadias, and a widened or bifid scrotum in males or a bifid clitoris in females. In late gestation, the pubic symphysis will also be widely spaced or absent. In some instances, MRI may aid in diagnosis and surgical planning.
When evaluating the fetus with an absent bladder, the first step should be to reassess later in the sonogram. In many cases, a temporarily absent bladder is a normal variant and will be visualized if given adequate time to fill. A bladder should fill within a 30-minute timeframe. Differential diagnoses for an absent bladder may include a wide spectrum of urogenital malformations affecting renal function such as bilateral renal agenesis, infantile polycystic kidney disease, and multicystic dysplastic kidneys. However, for these diagnoses, the kidneys will be either absent or abnormal, and the amniotic fluid will generally be low or absent, especially in the third trimester. Confirmation of the presence of kidneys using color and spectral Doppler, as well as assessment of kidney morphology, will help to eliminate these possibilities.
Absent bladder when seen in the presence of fetal growth restriction and oligohydramnios can also be suggestive of early onset placental insufficiency. Spectral Doppler assessment of the umbilical artery resistance, as well as middle cerebral artery pulsatility index, can help to distinguish this. When there is absence of a fetal bladder in conjunction with an anterior abdominal mass and normal kidneys, differential diagnoses include bladder exstrophy as well as cloacal exstrophy, and omphalocele and/or gastroschisis with a bladder that is extracelomic in position. Evaluation of the fetal genitalia as well as the cord insertion can help to distinguish these possibilities. Fetal MRI may be helpful in exceptionally complex cases.
Bladder exstrophy predominately occurs in males with an overall incidence of 1 in 40 000 births.3,4 It is not strongly associated with aneuploidy and has a low recurrence risk. Bladder exstrophy occurs when there is incomplete median closure of the inferior portion of the anterior abdominal wall. This happens due to failure of the mesenchymal cells to migrate between the ectoderm of the abdomen and cloaca during the fourth week of development. This results in the absence of the rectus muscles, leading to a deficiency in the external and internal oblique and transverse muscles. 3
Bladder exstrophy is a treatable fetal anomaly but requires detailed surgical planning for optimal long-term results. Advances in diagnostic imaging, specifically sonography, have increased the rate of prenatal diagnosis. Prenatal diagnosis allows the medical team to prepare a multispecialty approach. It also gives the parents time to prepare and adjust expectations associated with delivery and the neonatal period, as well as potential long-term complications and prognosis. Bladder exstrophy requires surgical repair to be done in multiple stages throughout early childhood beginning as a neonate, and this is typically done at one or two specialized centers with extensive experience.
Diagnosis prior to birth allows delivery at an appropriate center, which can prevent postnatal transfer and allow for maternal bonding. At a later date, bladder sufficiency tests are performed to evaluate the bladder capacity as bladder neck surgery may be warranted. Initial complications associated with bladder exstrophy repair include the need for early re-implantation of the ureters due to recurrent bladder infections or strictures. In addition, sometimes the remaining urethral plate will be insufficient to reach the end of the glans and the patient will be rendered hypospadiac with the urethra ending before the end of the glans. This can require multiple surgeries and expansions to repair and normalize the penile anatomy.
Multiple closures may be necessary and long-term complications include bladder prolapse, recurrent urinary tract infections, bladder calculi, and incontinence. 1 Some adult men with prior repair of exstrophy experience psychosexual development issues associated with a relatively smaller penile length (but widened girth), and the majority have retrograde ejaculation and infertility, which typically requires assisted reproductive technologies to conceive. Most adult women report no fertility issues and normal psychosexual development. 5
As evidenced by our case, gender determination prior to birth can be difficult, where the infant was inappropriately labeled as female on outside sonography. Being able to make the prenatal diagnosis can allow for families to become educated in birth appearance as well as the treatment and management of bladder exstrophy. This may help with normalization of psychosexual development. Because of the complexity of the disruption, the number of systems involved, and the complexity of the repair, prenatal diagnosis is critical. Prenatal diagnosis allows the patient and family to develop prenatal understanding, as well as plan for delivery, staged repair, and long-term care and support development for childhood.
Conclusion
Prenatal diagnosis of bladder exstrophy can be difficult and may be missed if the sonographer does not give the bladder adequate time to fill and therefore assumes the absence is physiologic. In the presence of an absent bladder, other features may include a low-set umbilical cord and small external genitalia with a lower abdominal external mass and widening of the pubic ramus. Early diagnosis of bladder exstrophy is helpful for surgical planning and a positive neonatal outcome. Magnetic resonance imaging may be a useful tool in the diagnosis of bladder exstrophy, but in this case sonography was the imaging modality of choice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.