
Abstract
Bladder exstrophy during adulthood is a rare deformity. A major surgical challenge encountered in bladder exstrophy cases is the repair of an anterior abdominal wall defect. The TopClosure® tension-relief system (TRS) is a simple and practical skin stretching and wound closure-secure system that can be useful in treating patients with bladder exstrophy. A 61-year-old man presented with a congenital bladder valgus and epispadias. The dorsal side of the penis was split. The patient underwent valgus cystectomy, bilateral ureteral skin stoma creation, and primary closure of the large defect of the anterior abdominal wall using the TopClosure® TRS. At the 1-year follow-up after surgery, the patient had recovered well, and there were no indications of major complications. Utilization of the TopClosure® TRS to repair the large abdominal defect is an innovative method for abdominal reconstruction. The TopClosure® TRS reduces operative time and the duration of hospital stay and improves wound aesthetics.
Keywords
Introduction
Bladder exstrophy is a rare congenital anomaly of the urinary system with an incidence of between one in 10,000 and one in 50,000, and this incidence is higher in men compared with women. 1 With the continuous advancement in the field of medicine, most patients with bladder exstrophy are treated in infancy, with rare reports of cases detected in adulthood.2,3 The malignant potential of bladder exstrophy increases with age if left untreated. 4 Bladder exstrophy is characterized by a soft tissue defect in the inferior abdominal wall, entire bladder mucosal eversion and exposure on the abdominal wall, separation of the bilateral rectus abdominis and pubic symphysis, and anterior wall division. The mucosa shows signs of inflammation, such as congestion and edema, and the bladder wall is thickened and hardened. The risk of bladder carcinoma in patients with bladder exstrophy is 700-fold higher than that in the age-matched general population. 5
TopClosure® tension-relief system (TRS) (IVT Medical Ltd., Ra’anana, Israel) is an innovative skin stretching and wound closure-secure system that uses both the mechanisms of stress-relaxation and mechanical creep for skin stretching, such that the skin surrounding the wound can undergo safe primary closure. TopClosure® TRS comprises two flexible polymer attachment plates and a flexible approximation strap. Its use has been previously reported to enable primary closure of medium to large skin defects.6–8 We herein report, for the first time, the application of this novel system for primary closure of an abdominal wall skin defect in a 61-year-old patient with bladder exstrophy.
Case report
A 61-year-old man with bladder exstrophy was referred to our hospital in April 2018 with no history of previous surgical intervention. The patient’s main complaints were bilateral lumbar pain accompanied by nausea, vomiting, chills, and fever, and complete inability to control urination. A rupture on the valgus bladder surface and minimal bleeding were detected. Since adolescence, the patient’s penis had shown a very limited degree of growth (Figure 1a,1b). The patient had low self-esteem and lack of social interaction. Further, the patient had never been able to ejaculate; however, the penis showed some degree of erection on sexual stimulation.
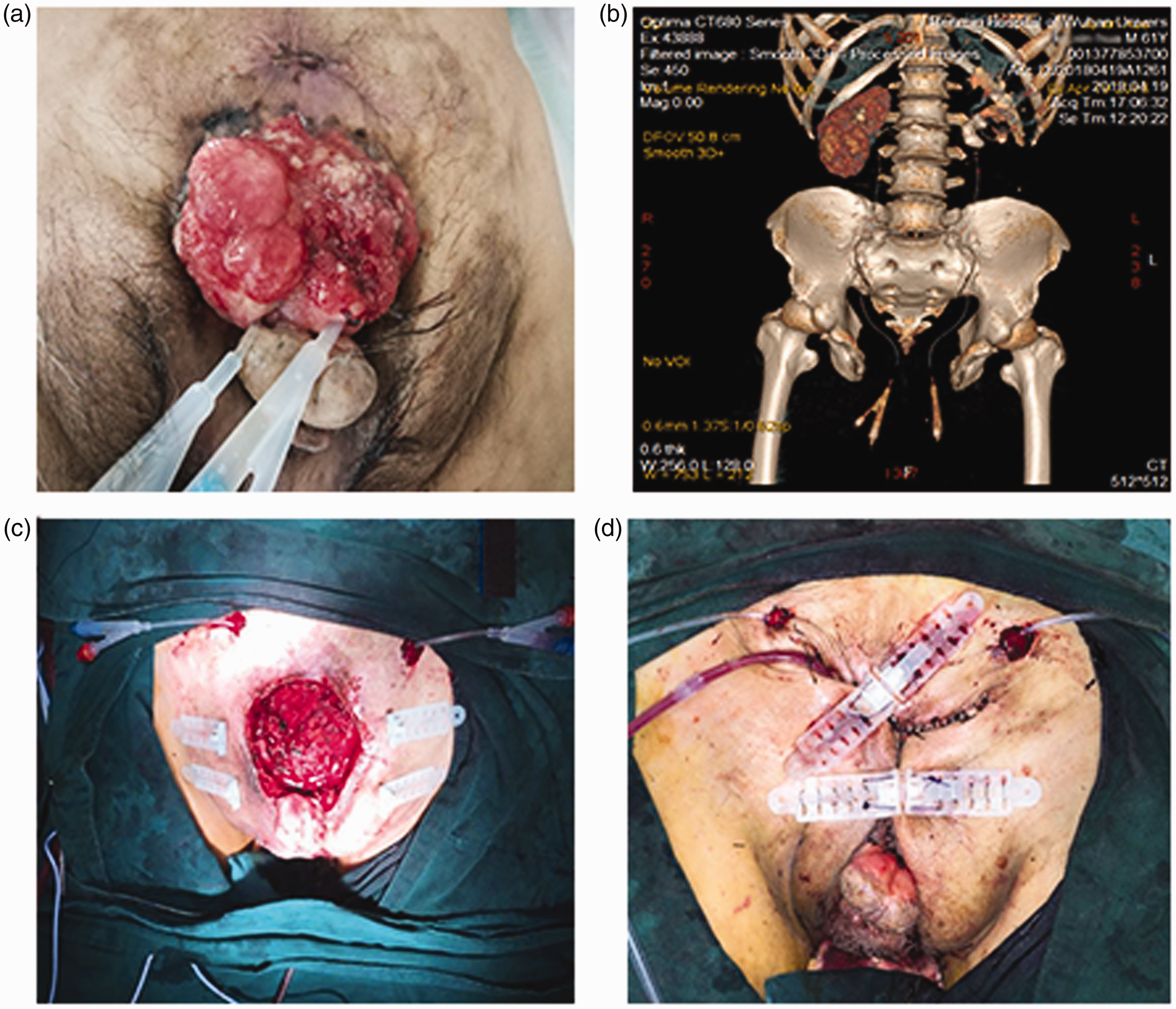
(a and b) Pre-surgical photograph of a patient with bladder exstrophy and the computed tomography-based three-dimensional reconstruction of the pelvis. The width of the pubic gap was 10.1 cm. (c) Intraoperative view of the abdominal skin defect (approximately 9 × 10 cm). (d) Immediate, direct primary closure was achieved by TopClosure® TRS.
Physical examination showed that a scarlet-colored bladder plate of 6.0 × 6.5 cm with partially thickening and mucosal erosion was located at the centre of the lower abdomen. The urethral opening was located at the dorsal side of the penis and clear urine was released intermittently from it. The epispadias penis with a splayed glans, which was approximately 2.5 cm long, was located beneath the bladder plate. Both testicles were normal. The anus was located behind the scrotum. Laboratory analyses showed the following results: white blood cell count, 19.55 × 109/L; neutrophils, 86.1%; hemoglobin, 107.0 g/L; urea 14.84, mmol/L; creatinine, 227.0 µmol/L; and estimated glomerular filtration rate, 25.86 mL/minute. Liver function was normal. Computed tomography examination of the urinary tract showed multiple calculi in both kidneys, with the largest of them being approximately 2.2 × 1.5 cm, and cysts could be seen in the left kidney. Bilateral ureteral catheter changes were observed after surgery. The bladder cavity was not observed. Multiple enlarged lymph nodes were noted in the retroperitoneum and the larger transverse diameter was approximately 1.0 cm. The pubic symphysis was separated, with a 10.1 cm gap, and the rectal anal canal was advanced. The penis was short, a hydrocele was noted in both testes, and some abdominal contents were dislocated into the bilateral inguinal canal. No other deformities or tumors were detected.
Under general anaesthesia, an F8 catheter was placed into the bilateral ureteral opening, and the bladder tissue near the bilateral ureteral opening was excised to the muscular layer. Pathological analysis of a rapid-frozen section of the surgically resected tissue showed intestinal epithelial metaplasia, which can provide better guidance when developing a surgical plan. All the skin tissue was excised at approximately 1 cm beyond the border of the bladder tissue, and the bladder was completely resected along the peritoneal surface. Simultaneously, the distal end of the bilateral ureters were placed in a double J tube-like papillary shape and sutured to the abdominal wall. After the peritoneal suturing had been completed, the full-thickness skin defect of the abdominal wall was approximately 9 × 10 cm (Figure 1c). The TopClosure® TRS, which has been widely used in clinical practice by Topaz and associates,6–8 was applied for wound closure. Two pairs of flexible polymer attachment plates (TopClosure®, 8-mm sets) were attached to the skin 2 cm away from the wound edges using adhesive and secured to the skin by skin staples (Weck Visistat® 35 W, 6.5 × 4.7 mm, Teleflex Medical, Morrisville, NC, USA). Based on our previous clinical application method,6–8 a pair of tension sutures (Ethicon 0, MO-2 PDS* II, 40 mm 1/2C, Johnson & Johnson International, New Brunswick, NJ, USA) was inserted through one attachment plate and deep into the subcutaneous tissue of the abdominal wall across the tissue gap, and then out through the contralateral attachment plate on the other side of the abdominal wall skin defect. The suture was then passed through the designated holes in the front part of the attachment plate and over to the first plate. Cyclical intermittent stress-relaxation forces were applied across the abdominal wall wound with these devices, and the highest tension was applied at the center of the wound (pull and tension for 30 seconds, and relaxation for 40–80 seconds). Intermittent absorbable subcutaneous sutures (Ethicon 3-0, VICRYL® Plus Antibacterial, 22 mm 1/2C, Johnson & Johnson International) were applied and locked in stages following the locking of the tension sutures to obliterate dead space. Wound margins were sutured using silk braided non-absorbable sutures (Ethicon MERSILK® 1, Johnson & Johnson International). The approximation strap was linked to the opposing attachment plates, enabling approximation and advancement of the attachment plates by an incremental pull on the approximation strap. Finally, the abdominal skin defect wound was tightly contacted with practically no dead space (Figure 1d). A high-vacuum wound drainage system (Redon bottle 200 mL, PFM Medical Ad, Nonnweiler-Otzenhausen, Germany) was placed in the wound. The entire surgical procedure lasted for approximately 3.5 hours, and the estimated blood loss was 70 mL. The patient’s condition was stable throughout the operation.
Follow-up and outcome
The TopClosure® TRS was applied for 14 days following the surgery to ensure wound closure. No obvious ischemia or necrosis of the wound edges was noted (Figure 2a). Two days later, the high-vacuum wound drainage system was removed. During the entire treatment process with TopClosure® TRS, the patient experienced mild pain. At approximately 12 months of follow-up, the wound had completely closed, with an aesthetically acceptable, minimally depressed scar (Figure 2b). Moreover, the patient could engage in outdoor activities.

(a) Fourteen-day postoperative photograph demonstrating wound closure with no obvious ischemia or necrosis of the wound edges. (b) Image taken approximately 12 months after surgery. The wound is fully healed with minimal scarring.
The patient and his family signed an informed consent form and gave permission for the publication of this case report and the accompanying images.
Discussion
Congenital bladder eversion impacts a patient’s quality of life, and it may also cause urinary tract infections leading to death; it is also associated with adenocarcinoma in the advanced stage. 9 Most patients with bladder eversion are treated during infancy, and thus, adult cases of bladder eversion are rarely reported. For adult patients, improving the overall physical appearance to improve the quality of life has become a top priority, especially in cases of anterior abdominal wall closure in bladder exstrophy patients. Abdominal skin and soft tissue defects caused by valgus surgery are common; however, repairing a large anterior abdominal wall defect is challenging. The traditional methods for repairing such defects mainly involve the use of various skin flaps alone or in combination with peripheral muscle tissue flaps.9–12 These surgical procedures are relatively complex and may lead to complications, resulting in large wounds and significantly prolonging hospitalization time. Another approach is to perform an osteotomy, which can facilitate easier repair of the anterior abdominal wall defect. However, an osteotomy reduces the stability of the pelvis and the surgical technique is complicated.9,11
The TopClosure® TRS is an innovative and practical approach. In the present case, after the resection of the bladder eversion and bilateral ureterocutaneous ostomy, the abdominal wall skin defect was approximately 9 × 10 cm. Direct suturing of the skin defect is considered to be difficult, and the use of a flap and osteotomy would have been complex and could have led to secondary complications. Thus, TopClosure® TRS was applied. The procedure was relatively simple and it greatly reduced the difficulty associated with this surgery. After surgery, the wounds healed well, which helped to shorten the hospitalization time and reduce the economic burden on the patient compared with that seen with traditional treatment methods.
Conclusion
Based on the findings of previous reports and the present case, the clinical application of the TopClosure® TRS can be considered to be feasible and effective to repair skin defects. Further laboratory and clinical investigations are warranted to better understand the viscoelastic properties of the skin and skin preconditioning under these extreme conditions, and when to couple tension sutures with the TopClosure® TRS for further optimization of wound closure. However, the clinical application of this new technology has definite advantages over traditional approaches for the closure of large skin defects and it may be considered in a wide range of surgical cases.
Supplemental Material
IMR891266 Supplemental Material - Supplemental material for TopClosure® tension-relief system for immediate primary abdominal defect repair in an adult patient with bladder exstrophy
Supplemental material, IMR891266 Supplemental Material for TopClosure® tension-relief system for immediate primary abdominal defect repair in an adult patient with bladder exstrophy by Zhanyong Zhu, Yilan Tong, Tianpeng Wu, Yueqiang Zhao, Mosheng Yu and Moris Topaz in Journal of International Medical Research
Footnotes
Acknowledgements
The authors thank all the hospital workers who participated in the surgery.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
This clinical case report (application of TopClosure® TRS in a 61-year-old male who presented with a congenital bladder valgus and epispadias since birth) has been reviewed by the Renmin Hospital of Wuhan University Ethics Committee. Because this article is a case report and does not involve human or animal testing, no formal ethics review was required.
Funding
This work was partially supported by research grants from the National Natural Science Foundation of China (no. 81601691) and the Key Project of Hubei Provincial National Science Fund (no. 2016CFA018).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.