
Abstract
Intramuscular myxoma is an uncommon benign soft tissue tumor that may arise from fibroblasts that produce an excessive amount of mucopolysacchrides. It is typically seen in adults in the large muscles of extremities and exhibits typical radiological features on sonography and magnetic resonance imaging. A case of intramuscular myxoma in the left Vastus intermedius is described in a 52-year-old man who presented with gradually increasing swelling in the thigh. The case illustrates characteristic radiologic “bright cap and rim” signs with pathologic correlation.
Introduction
Intramuscular myxoma is a mucopolysacchrides rich benign tumor arising from skeletal muscles in adults.1–3 Exudation of mucoid material from the lesion into the adjacent musculature due to the lack of a complete pseudo-capsule leads to muscle atrophy, increased fat deposition, and surrounding edema. On sonography and T1-weighted magnetic resonance imaging (MRI), the peri-lesional fat rind manifests as “bright rim” and “bright cap” signs on the periphery and at either pole, respectively. The associated edema appears as increased signal intensity in the adjacent muscles on T2-weighted MRI.4,5 This report presents a case of intramuscular myxoma in the Vastus intermedius of the left thigh with characteristic imaging findings and signs on sonography and MRI and presents the pathologic correlation.
Case Report
A 52-year-old man presented with a history of gradually increasing swelling over the past 5 years involving the anterior aspect of the left upper thigh. There were no complaints of associated pain or fever. On palpation there was an ill-defined area of swelling in the left upper thigh, which was only tender to deep palpation; the overlying skin was unremarkable. The remainder of the physical examination did not reveal any similar swelling elsewhere, and the systemic examination was unremarkable. Laboratory investigations including a complete blood count, prothrombin time, and erythrocyte sedimentation rate were normal.
The sonographic examination demonstrated a well-marginated, oval-shaped hypoechoic intramuscular lesion with posterior acoustic enhancement. No echogenic foci or anechoic component were evident. The lesion showed a bright rim along the anterior aspect (bright rim sign) and a hyperechoic triangular area along the inferior pole of the lesion (bright cap sign) (Figures 1a and 1b). The adjacent muscles of the thigh were grossly unremarkable. On color Doppler flow interrogation, no obvious color filling could be seen in the lesion.

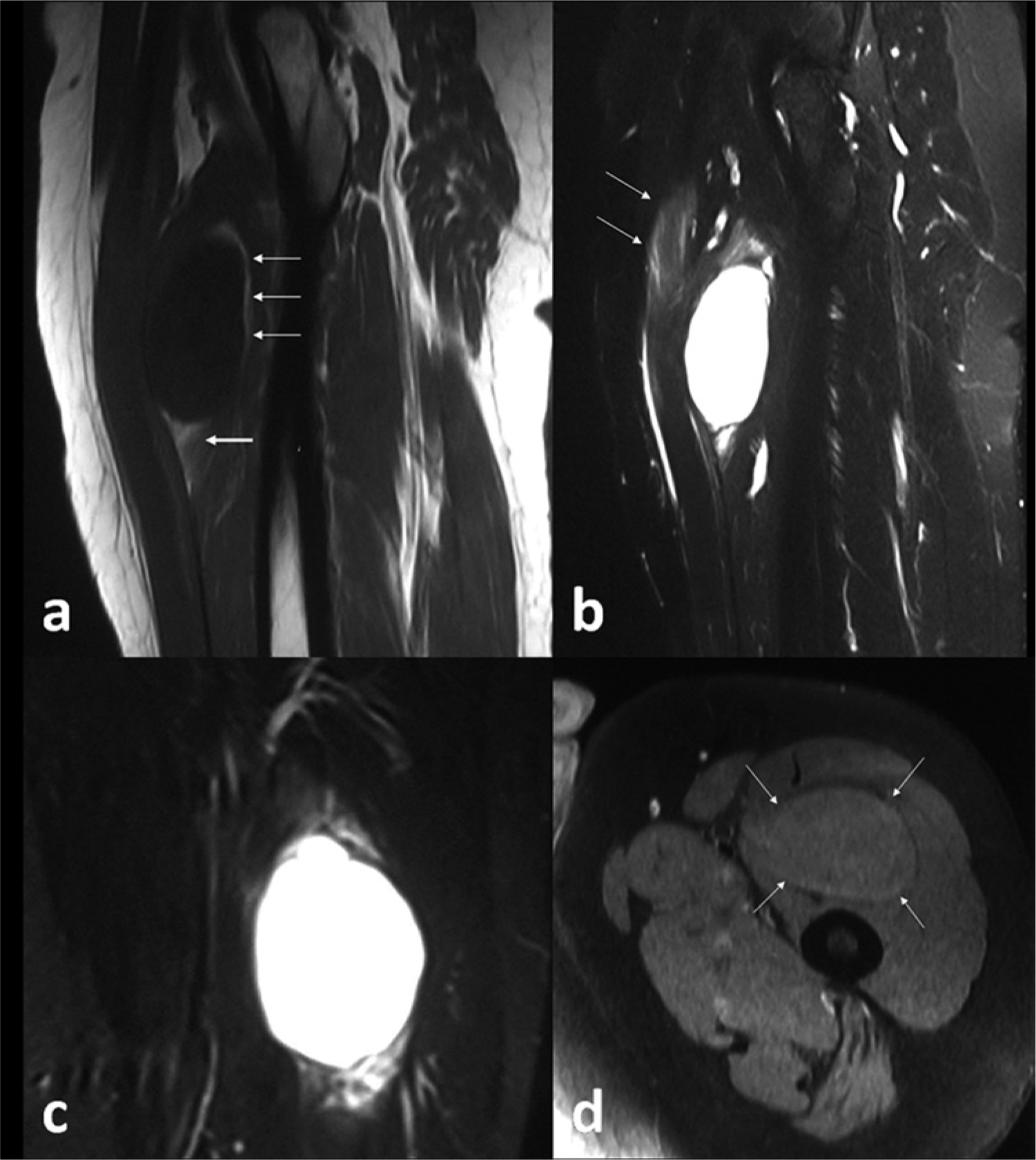
On MRI the lesion was intramuscular in location in the Vastus intermedius. The lesion appeared homogenously hypointense on T1-weighted imaging and homogenously hyperintense (similar to fluid) on T2-weighted imaging and fluid sensitive short tau inversion recovery imaging (Figures 2a, 2b, and 2c). The superior and inferior aspects of the lesion demonstrated increased T1 signal (the equivalent of the bright rim and cap signs seen in Figure 1a). The adjacent muscles of the thigh (Rectus femoris, Vastus medialis, and Vastus lateralis) revealed mild interstitial increased signal on T2-weighted imaging (Figure 2b). On contrast enhancement the lesion showed moderate, relatively homogenous contrast enhancement (Figure 2d).
Percutaneous sonographically guided fine needle aspiration showed stellate shaped tumor cells with bland nuclear chromatin and long wispy cytoplasmic processes in a myxoid background consistent with myxoma (Figure 3). The lesion was surgically excised and histopathological examination further substantiated the diagnosis of myxoma. The patient has remained on regular follow-up for the past 18 months without any complaints.
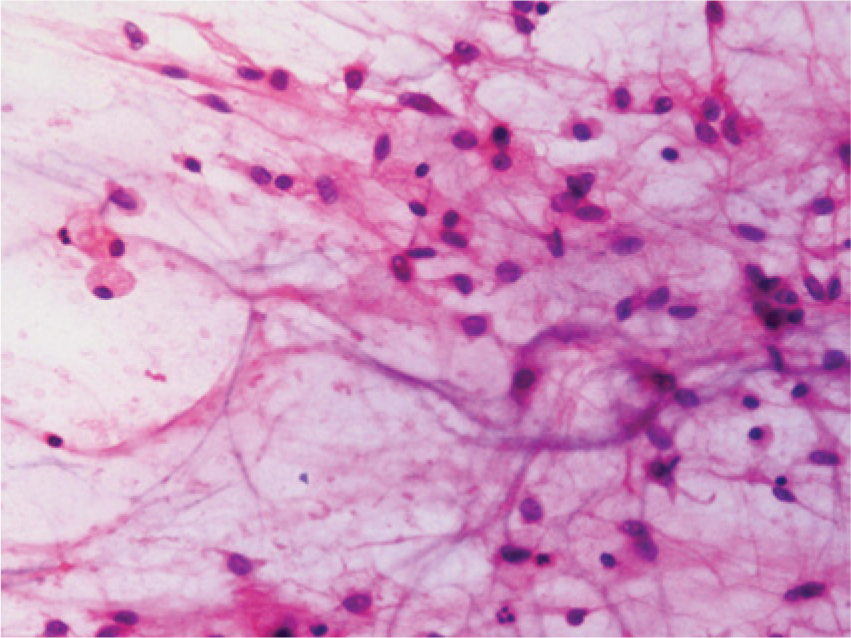
Microphotograph of percutaneous ultrasound-guided fine needle biopsy material showing stellate shaped tumor cells with bland nuclear chromatin and long wispy cytoplasmic processes in a myxoid background. (Hematoxylin and eosin stain; original magnification, ×40.)
Discussion
Intramuscular myxoma is an uncommon benign soft tissue tumor occurring in adults aged 40 to 70 years, with a slight female preponderance. Its typical location is in the large muscles of the thigh, buttocks, and upper limbs.1,6,7 However, it can also be found in the masseter muscle, the cervical muscles, and other locations as well.2,3 These are benign neoplasms that may arise from fibroblasts that produce an excessive amount of mucopolysacchrides. 1
Myxomas usually lack a capsule and often have an incomplete pseudocapsule. 1 It has been postulated that because of this incomplete pseudocapsule, there may be exudation of mucoid material from the lesion into the adjacent musculature that leads to muscle atrophy, subsequent increased fat deposition, and surrounding edema. This peri-lesional fat rind and the increased signal intensity in the adjacent muscles seen on T2-weighted MRI are imaging features strongly suggestive of intramuscular myxoma.4,6,7 The same pathologic sequence can explain the sonographic bright rim sign of echogenecity around the myxoma as explained by Girish et al. 5 In their retrospective study they reported that 83% (5/6) of the patients with myxoma showed this bright rim sign, which is defined as hyperechogenecity involving at least one fourth of the circumference of the lesion. Similarly, the “bright cap sign” was defined as the presence of a triangular hyperechoic area adjacent to at least one of the poles of the mass. This bright cap sign was also seen in 83% (5/6) of the patients in their study.
Intramuscular myxoma may be associated with fibrous dysplasia, and they may be multiple, an association that is termed Mazabraud’s syndrome.8,9 In a series of 24 patients with intramuscular myxoma reported by Aoki et al., 10 six patients had McCune-Albright syndrome where pigmentation of the skin and endocrine abnormalities were also present.
The differential diagnosis of a lesion in the thigh with imaging findings of a mass with high water content (mimicking a cyst) include synovial cyst, ganglion, bursa, neurogenic tumor, myxoid liposarcoma, and malignant fibrous histiocytoma.1,7 The majority of synovial cysts, bursae, and ganglia occur at typical locations such as the popliteal fossa and dorsal aspect of wrist. These lesions typically are seen in intermuscular planes, whereas most soft tissue myxomas are intramuscular in location. Also, as compared to intramuscular myxoma, these lesions show a cystic nature with peripheral rim enhancement and delicate septae only seen on postcontrast computed tomography and MR images. Sonographically, these lesions show an anechoic component as compared to intramuscular myxoma, which are hypoechoic in echotexture, with posterior acoustic enhancement and no anechoic component.
Neurogenic tumors are also typically located in the intermuscular compartment. A nerve entering and exiting the lesion is usually appreciated at the margins of the lesion. These imaging findings are not seen in intramuscular myxomas. Similarly myxoid liposarcomas are usually intermuscular lesions developing in the subcutaneous fatty tissue, unlike soft tissue myxomas. In addition, myxoid liposarcomas usually contain small amounts of intrinsic fat. In this respect, the intramuscular myxoma may have some imaging features similar to myxoid liposarcoma.
Myxoid malignant fibrous histiocytomae are intramuscular lesions similar to myxomas, however these lesions show far more heterogenous appearance on imaging, with areas of hemorrhage. These lesions also show some solid nodular component with prominent contrast enhancement, whereas the myxomas show moderate, relatively homogenous enhancement.1,4,6,7
Though the radiological features of intramuscular myxoma are quite typical, the lesion can be confirmed by fine needle aspiration cytology (FNAC) or open biopsy. Histologically the tumor shows low cellularity with bland appearing spindle cells having no mitotic figures, with absent to very low vascularity in the myxoid background.6,7 Intramuscular myxomae are typically treated with marginal excision when they become symptomatic, with almost no recurrence. In a case of recurrence, the histopathogical diagnosis should be reviewed. 11
In summary, in a middle-aged patient when an intramuscular mass that is slowly increasing in size is seen with characteristic sonographic features of bright rim and bright cap signs, intramuscular myxoma is the most likely diagnosis. Correlative MRI images will show fluid intensity signals of the lesion with increased signal in the adjacent muscles on T2-weighted and fluid sensitive sequences, a peri-lesional fat rind on T1-weighted sequences, and intense but heterogeneous enhancement. The diagnosis can be further proved on histopathological (FNAC) evaluation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.