
Abstract
To understand the mechanisms involved that lead to the high prevalence of work-related musculoskeletal disorders in sonographers, this motion capture study evaluated upper extremity kinematics during kidney scans. The purpose of this study was to provide an evaluation of joint ranges of motion during scanning, which could be helpful in assessing risk of injury. A Vicon MX motion capture system recorded reflective marker positions while four sonographers scanned a volunteer’s kidneys. The results indicated that sonographers were scanning with their shoulders in flexion, abduction, and external rotation. The elbows were in flexion and the wrists in extension in all cases with the exception of portions of one scan. Shoulder abduction and wrist extension angles exceeded acceptable published limits. These results could be used to improve patient and sonographer positioning, equipment adjustability, and transducer design.
Work-related musculoskeletal disorders are characterized by soft tissue discomfort caused or aggravated by workplace exposures, which can affect the muscles, joints, tendons, ligaments, or nerves. 1 Sonographers routinely suffer from work-related musculoskeletal disorders as a result of ergonomic hazards and working conditions. Ergonomic hazards that are a risk for strain injury include repetitive motions, forceful motions, static muscle loads, mechanical stresses, and awkward postures. 2 Conditions that have been reported to contribute to work-related musculoskeletal disorders are scanning durations more than 45 minutes, insufficient breaks between patients, and nonadjustable equipment.2–4
In a study published in 1997, 81% of sonographers in the United States reported scanning in pain. 1 A survey of sonographers in the United States and Canada published in 2009 found that this had increased, with 90% reporting scanning in pain. 4 Among other factors, productivity advancements in ultrasound equipment have contributed to an increase in sonographers reporting pain because ultrasound image processing time has decreased. This has resulted in shorter durations between patients and an increase in the number of patients scanned per day. 5 Current treatments for many musculoskeletal disorders are anti-inflammatory drugs, physical therapy, and occupational therapy. 4 However, the persistence of pain has resulted in 20% of sonographers prematurely retiring or leaving the profession. 6
During a sonographic examination, several factors have been identified as contributing to injury or discomfort to muscles or joints. 7 Miniscule fine motor control movements of the transducer and gripping the transducer tightly may injure the muscle fibers or tendons in the fingers, hand, and forearm. Twisting and bending of the wrist to the extreme ranges of motion while applying pressure with the probe can increase strain in the wrist. Shoulder abduction while applying pressure to the patient for long durations can strain shoulder, neck, and back muscles. Performing a sonogram in awkward positions will result in the sonographer continuously twisting his or her torso and neck to see the monitor. As a result of these movements, the reported musculoskeletal pain has been primarily experienced in the shoulders, neck, wrist, back, and hands.3,7,8
To evaluate the mechanisms that lead to the high prevalence of work-related musculoskeletal disorders in sonographers, this study documented upper extremity kinematics during kidney scanning with a Vicon MX motion capture system with eight LED strobe cameras. No other studies have reported using 3D motion capture to document the upper extremity kinematics of sonographers while scanning. During the scans, the sonographers scanned both left and right kidneys using two ultrasound transducer designs. The kinematic measures investigated were shoulder, elbow, and wrist joint angles. The results were evaluated to determine the extent to which the joint angles exceeded acceptable published limits and how they compared to those measured with electrogoniometers as reported in a previous study by Burnett and Campbell-Kyureghyan. 9
Methods
Experimental Design
Four volunteer sonographers with at least 3 years of experience in diagnostic medical sonography were recruited to participate as subjects in this study. The participants were right-hand-dominant women, with a mean age of 40.8 ± 15.0 years. The same volunteer male patient was scanned by all four participants to reduce variation. He had an age of 23 years, height of 191.8 cm, mass of 115.2 kg, and a body mass index of 31. This study was conducted with approval from the local institutional human research review committee (the local institutional review board), which ensured that the rights of the participants were protected. Before initiation of the study, all participants signed the approved committee consent form after being informed about the aims and procedures of the study.
Participants 1 and 2 chose to sit in a backless, height-adjustable swivel chair while they were scanning. Participants 3 and 4 chose to stand while they were scanning. All four used the Philips iU22 ultrasound system with the curved array C5-1 and phased array S5-1 transducers (Philips Medical, Bothel, WA) to scan the patient’s left and right kidneys. The C5-1 transducer has a larger grip and scanning surface, approximately 4 and 7 cm in width, respectively, in comparison to the S5-1 transducer, which has an approximate 3-cm grip width and 3-cm surface width. More information on the two transducers can be found in a previously published study, which measured the pressure required to produce a quality scan via a capacitive sensor mat wrapped around the handle of the transducers. 10
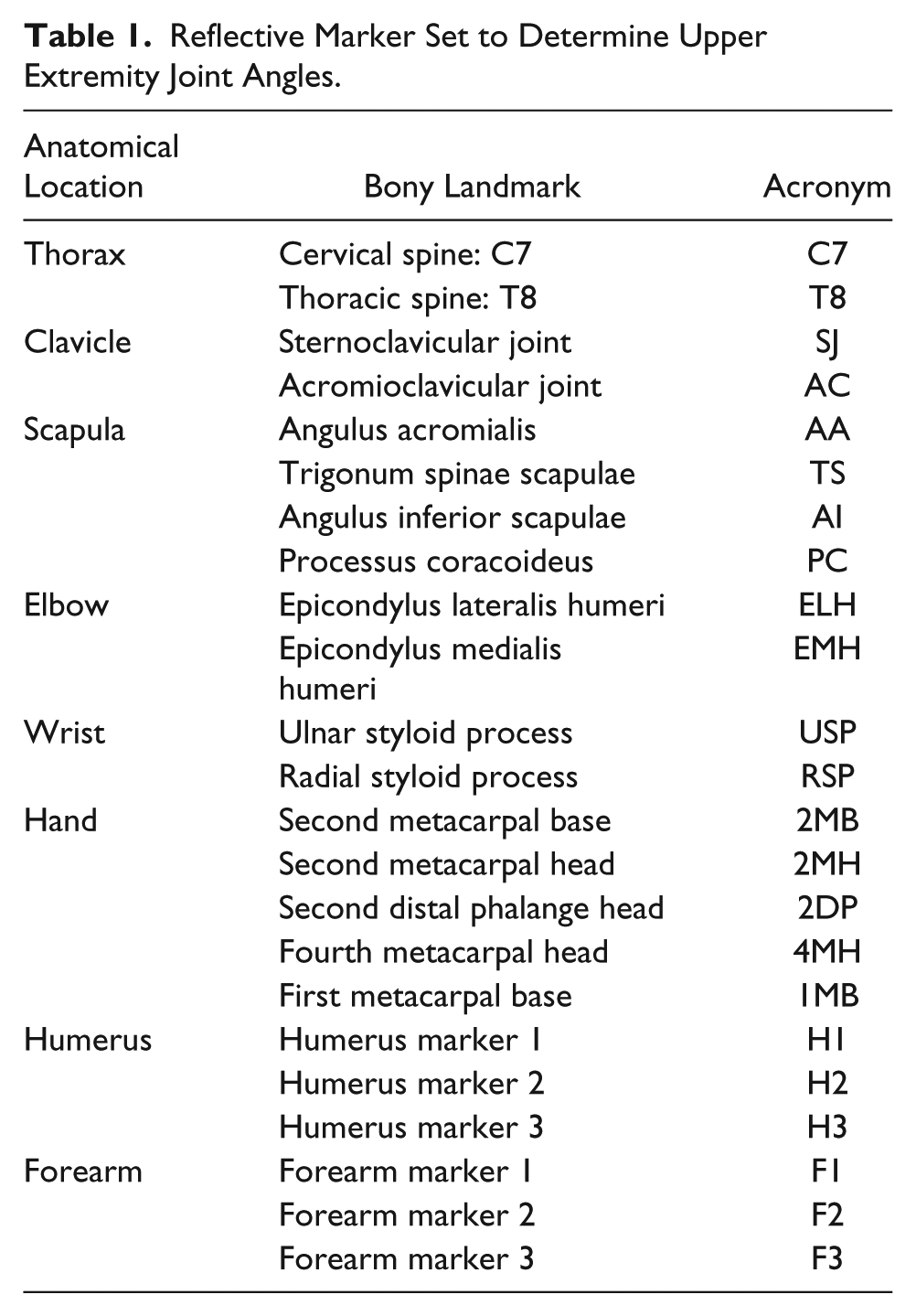
The Vicon MX motion capture system was used to collect the kinematic data of the sonographers during the kidney scans. The motion capture system recorded the 3D locations of reflective markers throughout each scanning trial using a sampling frequency of 100 Hz. The reflective markers were placed on each participant’s upper dominant extremity and torso (Figure 1 and Table 1). Each subject was then given the opportunity to adjust the bed, ultrasound machine, and chair (if it was being used). Then the sonographer instructed the patient to lie on his back on a standard examination bed with his abdomen exposed. The patient’s right side was located next to the sonographer so that his right kidney could be scanned. An alternative position used for the right kidney scan was the patient lying on his left side with his back to the sonographer. The sonographer was directed to take four longitudinal scans of the patient’s right kidney using the same procedures that she would in a clinical setting. Data collection for each trial ceased when the sonographer indicated that she was finished scanning.
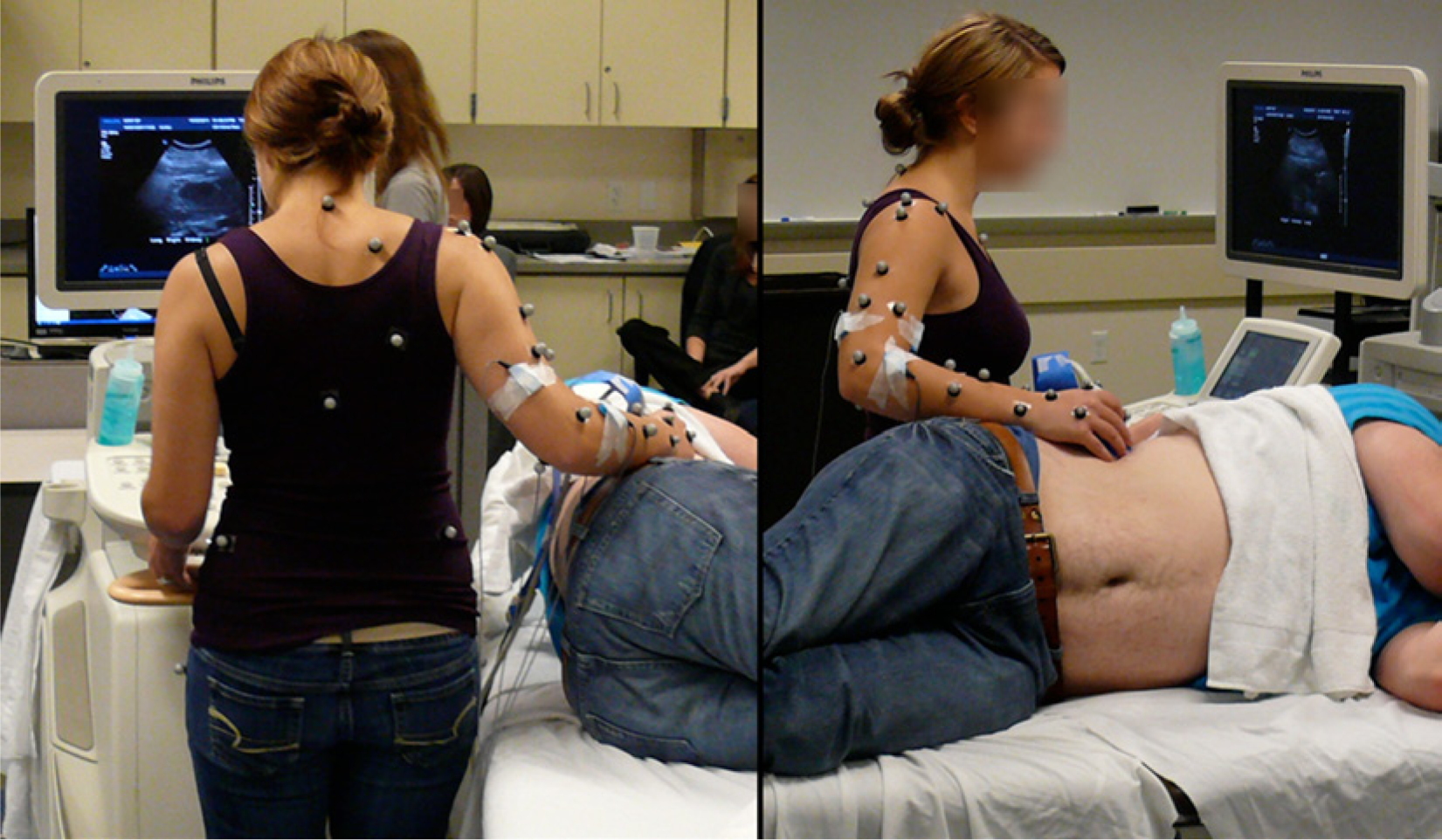
Photograph showing the position of the reflective markers on the sonographer while scanning the right kidney of the patient.
Reflective Marker Set to Determine Upper Extremity Joint Angles.
After completing the scan of the right kidney, the sonographer instructed the patient to lie on his right side facing the participant so that the ultrasound system would not have to be moved, and the same process was repeated for the left kidney scan. At the completion of these two scans, the C5-1 transducer was disconnected from the ultrasound system and the S5-1 transducer connected. While the researchers were setting this up, the sonographer was able to have a 15- to 30-minute rest period. After the recovery period, the sonographer, patient, and researchers repeated the same process for scanning the right and left kidneys of the patient with the S5-1 transducer. The duration of the scans ranged from 43 to 158 seconds, with an average duration of 74 seconds.
Analysis
Kinematic analysis was performed for each kidney scan to determine three shoulder angles (flexion/extension, abduction/adduction, and internal/external rotation), one elbow angle (flexion/extension), and one wrist angle (flexion/extension). The joint centers were established in the global coordinate system for every frame of data analyzed to determine the joint angles and to create local anatomical reference frames. The shoulder joint center was determined by finding the optimal pivot point, which is the point closest to the instantaneous helical axis determined for each frame analyzed. The instantaneous helical axis was determined with at least three landmarks on the scapula. The wrist and elbow joint centers were located at the midpoint between the markers located medially and laterally to the joints.
Local technical reference frames were established for the upper arm and forearm to determine the local and global positions of the joint centers (Table 2). The technical reference frames for the forearm varied because of the availability of visible markers on the forearm during each data collection. The shoulder and elbow joint centers were defined with respect to the upper arm technical reference frame. The wrist joint center was defined with respect to the forearm technical reference frame. The anatomical reference landmark locations and axial orientations used were those recommended by the International Society of Biomechanics. 11 Additional technical details for the determination of the upper extremity and thorax reference frames and shoulder, elbow, and wrist joint angles are available in the appendix.
Local Technical Reference Frames for the Upper Arm (Humerus) and Forearm.
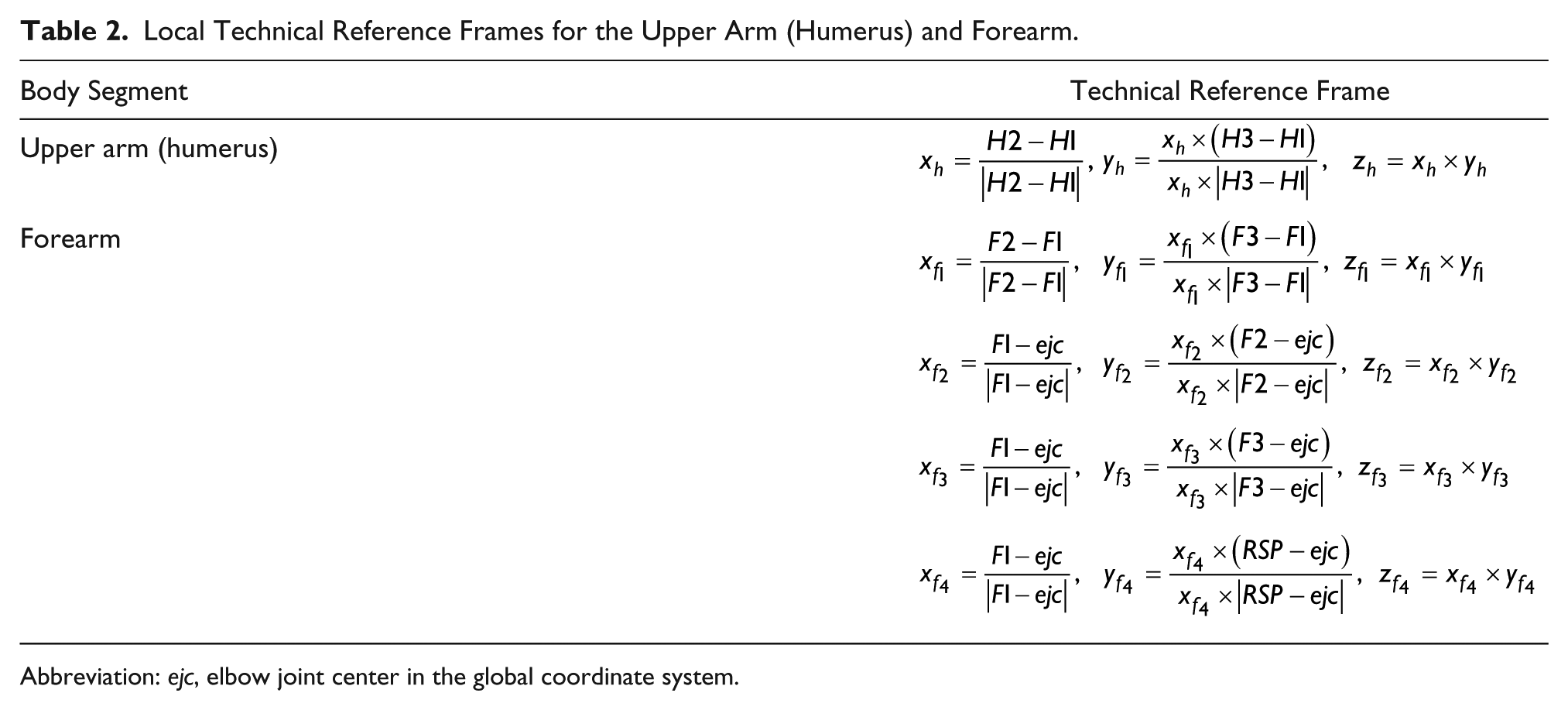
Abbreviation: ejc, elbow joint center in the global coordinate system.
Results
The shoulder joint was predominantly in flexion for all sonographers except for portions of scans with the C5-1 transducer by sonographer 4 (Figure 2). When sonographer 4 scanned with the C5-1 transducer, the shoulder was in extension 3% of the time for the left kidney and 49% of the time for the right kidney. The maximum shoulder flexion and extension angles were 91° and −12°, respectively. The shoulder flexion values were greater on average for seated scans (37°) than standing scans (16°) (Table 3).
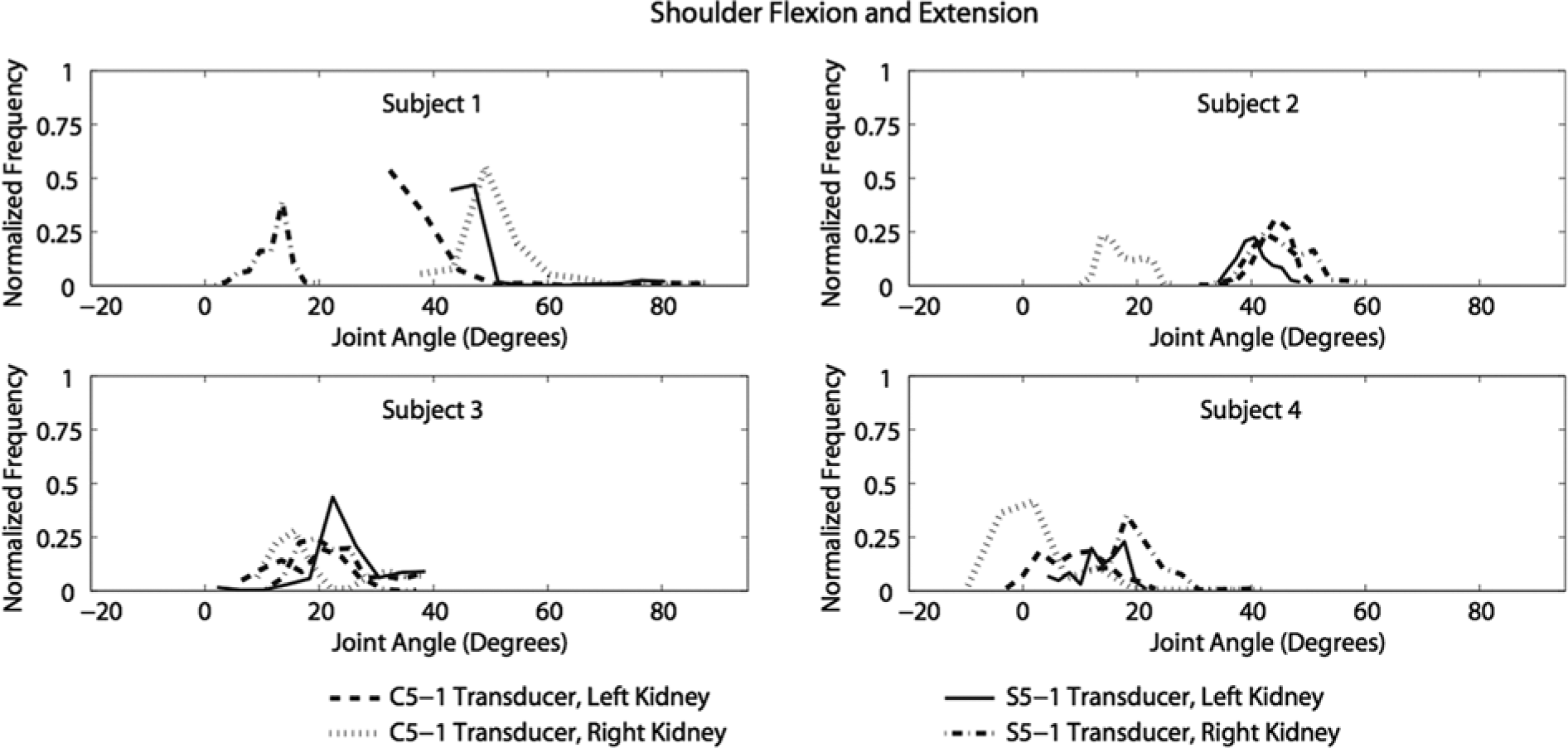
Normalized histogram of shoulder joint flexion (+) / extension (–) angles recorded during scanning.
Minimum, Maximum, and Average Joint Angles Achieved for All the Scans Based on the Different Scanning Factors.
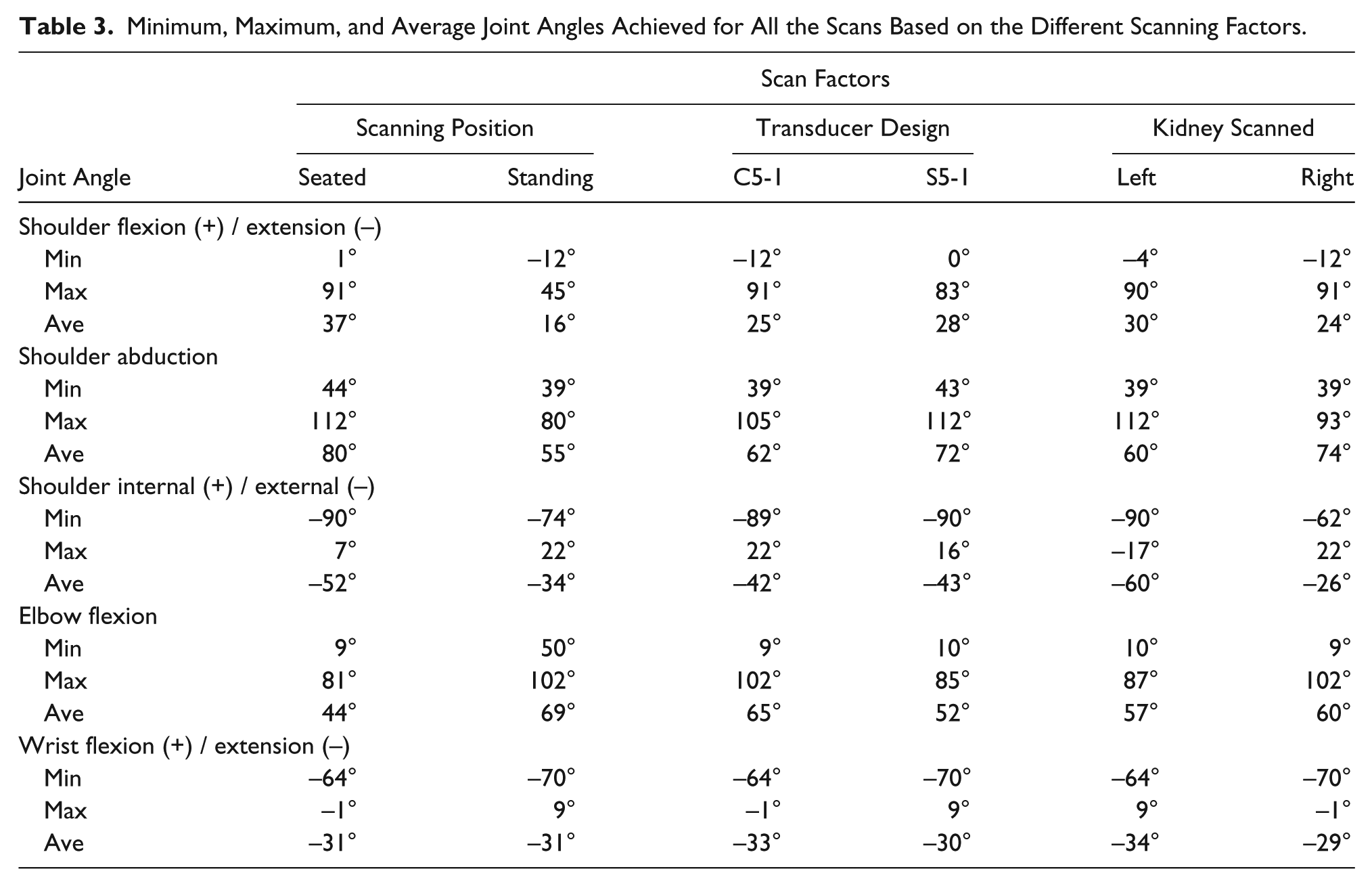
Only shoulder abduction occurred during scanning with maximum and minimum angles of 113° and 39°, respectively (Figure 3). The abduction angles were greater on average when the sonographers were seated and using the S5-1 transducer to scan the patient’s right kidney (Table 3).
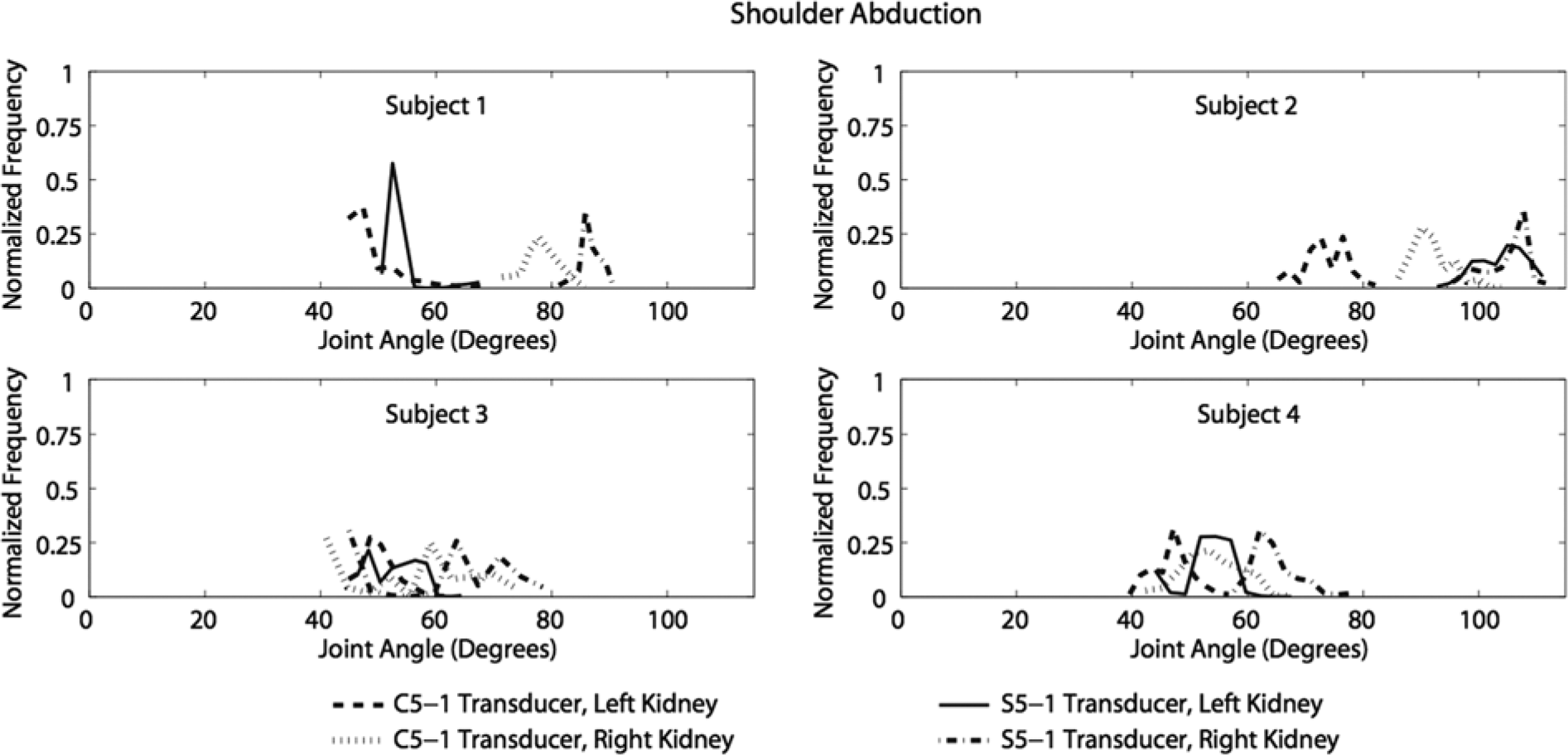
Normalized histogram of shoulder joint abduction angles recorded during scanning.
External shoulder rotation was experienced by all the sonographers (Figure 4). Internal shoulder rotation was experienced by sonographers 1 and 3 only. The maximum shoulder internal rotation angle generated was 22° and the maximum external rotation angle was 90°. The external rotation angles were greater on average for seated scans of the left kidney (Table 3).
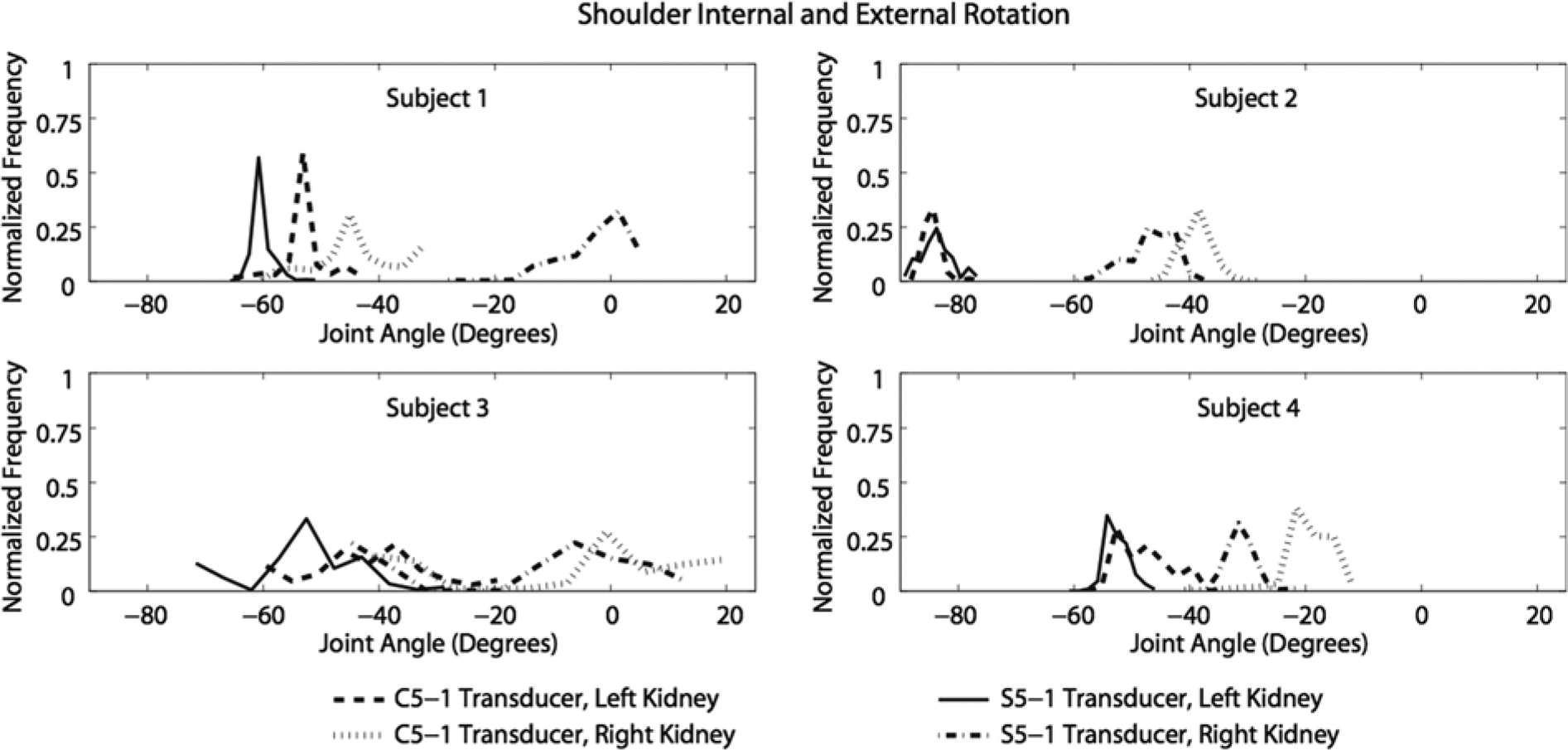
Normalized histogram of shoulder joint internal (+) / external (–) rotation angles recorded during scanning.
The elbow joint was in flexion during this study for all sonographers (Figure 5). The maximum and minimum elbow flexion angles generated were 102° and 9°, respectively. There were no similarities of note among the sonographers for elbow flexion. The elbow flexion angles were greater on average when they were standing and using the C5-1 transducer (Table 3).
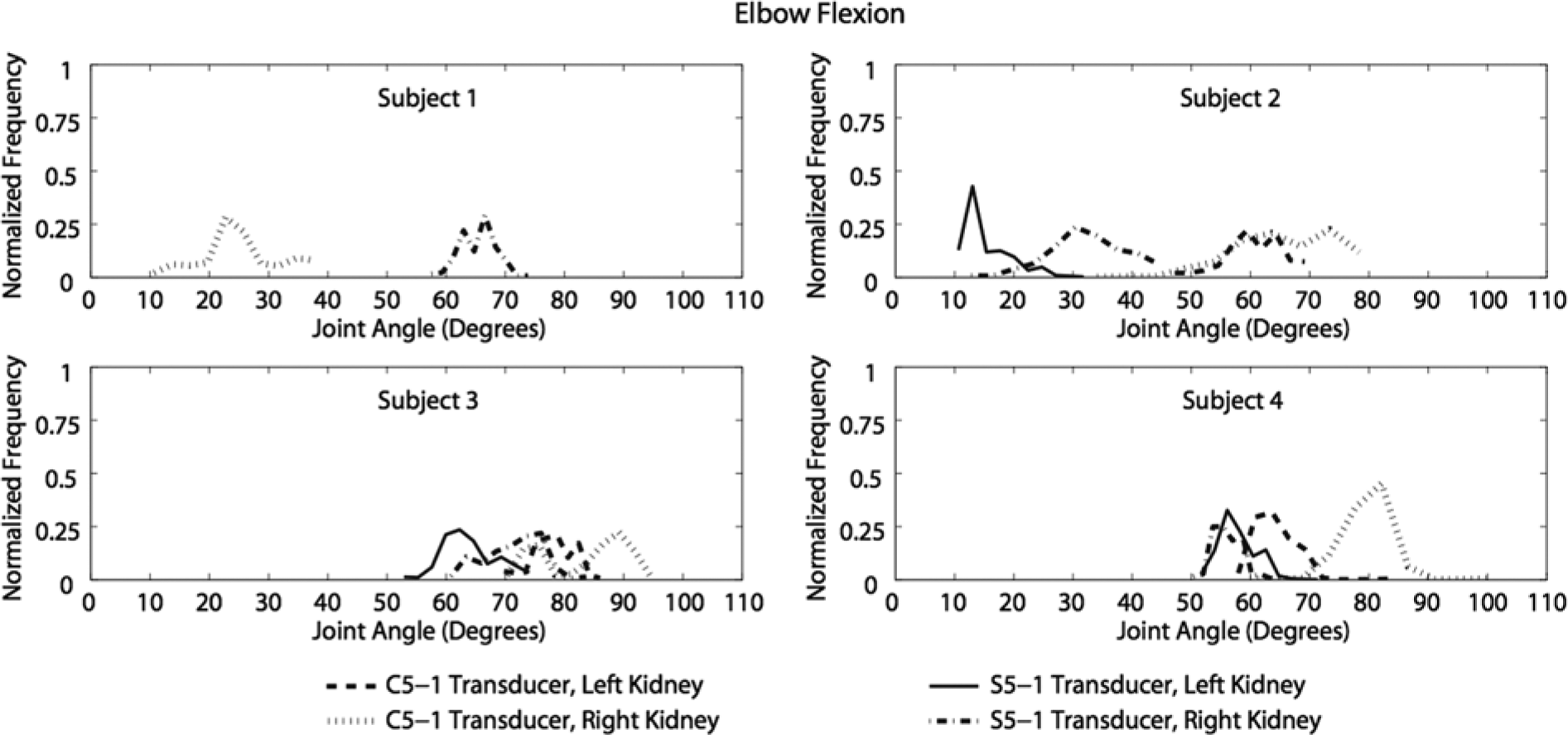
Normalized histogram of elbow joint flexion angles recorded during scanning.
All sonographers experienced extension at the wrist joint except during a portion of one scan performed by sonographer 3 (Figure 6). During the left kidney scan with the S5-1 transducer, sonographer 3 was in flexion during 14% of the scan. The maximum wrist flexion generated was 9°, and the maximum extension was 70°. There were minimal differences in the average wrist flexion angles for the following scans, respectively: seated versus standing (31° vs. 31°), C5-1 versus S5-1 (33° vs. 30°), and left versus right kidney (34° vs. 29°) (Table 3).
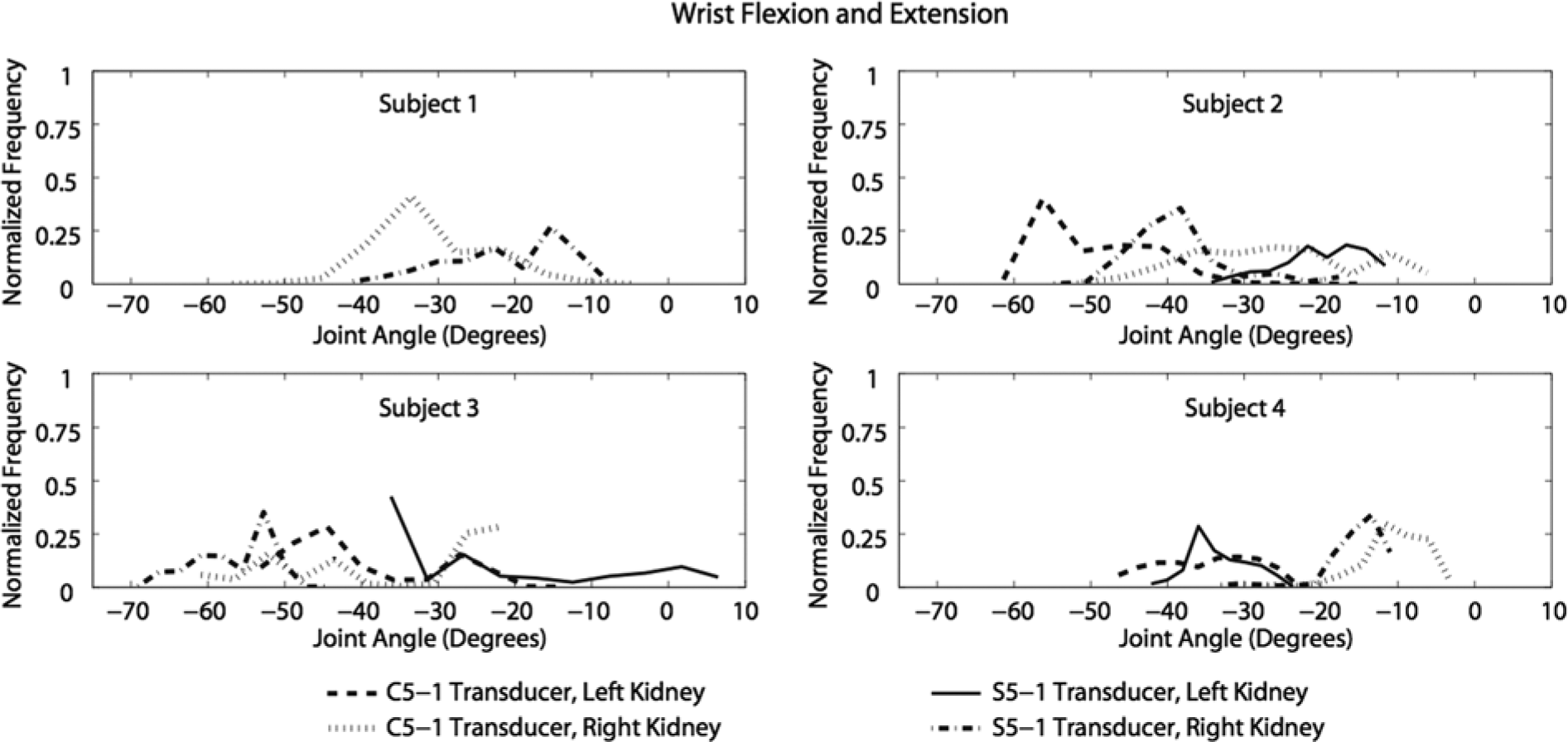
Normalized histogram of wrist joint flexion (+) / extension (–) angles recorded during scanning.
The sonographer’s scanning position (seated or standing) had the greatest difference (46°) for maximum shoulder flexion/extension and the least difference (5°) for minimum shoulder abduction (Table 3). Ultrasound transducer design had the greatest (17°) and least (<1°) differences for maximum and minimum elbow flexion, respectively. The kidney that was scanned (right vs. left) had the greatest difference (40°) for maximum internal/external shoulder rotation and the least difference (<1°) for minimum elbow flexion.
Discussion
Sonographer 1 generated larger shoulder flexion angles because she tilted her torso forward when she needed to use the keyboard on the ultrasound machine (Figure 2). Additionally, sonographer 1 maintained a smaller shoulder flexion angle range for a longer duration when compared to the other sonographers; in other words, she was not flexing and extending her shoulder as much as the other sonographers. Sonographer 2 had a similar flexion angle range for all scans except when she scanned the patient’s right kidney using the C5-1 transducer. For that scan, the angle range was offset about 20° less than the other scans because the sonographer decreased the distance between her torso and the patient’s kidneys. In the scans performed by sonographer 3, shoulder flexion was within the same angle range regardless of the transducer used or the kidney scanned. Higher shoulder flexion angles were achieved by sonographers 1 and 2, who were seated during the scanning procedures.
Shoulder abduction angles that were generated by sonographers 1, 3, and 4 were similar during left kidney scans (Figure 3). Sonographer 2 had larger abduction angles than the other three sonographers because she rested her arm on the patient while she scanned. The acceptable range for shoulder abduction has been reported to be between 0° and 20°. 12 When the shoulder is elevated more than 30° of abduction, it can cause fatigue and a reduction in blood flow to shoulder muscles and tendons, leading to injury or pain.13,14 Shoulder abduction exceeded these acceptable limits for all trials of all sonographers. During this study, the sonographers’ shoulders were never abducted less than 38°.
Shoulder internal and external rotation angles varied for each sonographer (Figure 4). When sonographer 1 scanned the patient’s left kidney, she maintained a smaller angle range. Greater external rotation angles were maintained for longer durations by sonographers 1 and 2, who were seated. Sonographer 3 experienced larger ranges of motion because she shifted her weight from one foot to the other when she needed to use the keyboard, resulting in her twisting her torso. Additionally, external rotation was greater when the sonographers were scanning the patient’s left kidney because of the position of the patient.
Elbow angles were not obtained for sonographer 1 when she scanned the patient’s left kidney, because of insufficient forearm marker detection by the cameras. When sonographer 2 scanned the patient’s right kidney, she had a larger elbow joint range of motion because she moved her chair or tilted her torso more often (Figure 5). Sonographer 4 had larger elbow flexion angles than the other sonographers, perhaps because of the location of the patient’s kidneys in relation to the sonographer’s shoulder joint, which was at a higher elevation in comparison to the other sonographers such that she did not need to extend her elbow as much while scanning. In comparison of the scans with the larger C5-1 ultrasound transducer design with those of the smaller S5-1 transducer, the sonographers demonstrated the greatest maximum differences in elbow flexion (17°). The sonographers tended to hold the C5-1 transducer closer to their bodies during scanning, which possibly resulted in a less awkward posture for the larger transducer.
Wrist angles were not obtained for sonographer 1 during the scanning of the patient’s left kidney for the same reason why elbow flexion angles were not obtained, as described above. Sonographer 3 had greater wrist extension angles when she scanned the patient’s right kidney. When sonographer 4 scanned the patient’s left kidney, she had a similar angle range with both transducer designs and obtained larger extension angles than when she scanned the right kidney. Sonographers 1, 2, and 3 had larger ranges of motion than sonographer 4. Acceptable wrist extension has been reported to be between 0° and 15° during scanning. 15 This near neutral position is recommended during repetitive activities to decrease strain on the wrist and decrease pressure on the median nerve.2–8,15 When the wrist angle is within this range, carpal tunnel pressure typically remains below 30 mm Hg. A substantial increase in carpal tunnel pressure over 30 mm Hg can cause detrimental effects to the median nerve. In previous studies when carpal tunnel pressure ranged from 40 to 50 mm Hg for 8 hours, it resulted in nerve signals being completely blocked. 15 The average wrist angles in this study for all scans were approximately 30° of extension, twice the acceptable upper limit.
The study of Burnett and Campbell-Kyureghyan determined joint angles for the scanning arm of seven sonographers using electrogoniometers for the following scans: thyroid, right abdominal, left abdominal, right deep venous thrombosis, and left deep venous thrombosis. 9 The joint angles evaluated were wrist flexion and extension, wrist radial and ulnar deviation, elbow flexion and extension, forearm pronation and supination, and shoulder abduction. The ranges of shoulder abduction and elbow flexion angles calculated during left and right kidney scans during the present study were comparable to those measured during left and right abdominal scans in the Burnett and Campbell-Kyureghyan study. During left abdominal scans, Burnett and Campbell-Kyureghyan reported shoulder abduction angles of 36.8° to 99.2° (compared to 39° to 112° during left kidney scans in this study), and a peak elbow flexion angle of 85.6° (compared to a range of 10° to 87° during left kidney scans in this study). During right abdominal scans, the authors reported shoulder abduction angles of 39.6° to 99.1° (compared to 39° to 93° during right kidney scans in this study) and peak elbow flexion angles of 98.1° (compared to a range of 9° to 102° during right kidney scans in this study).
The wrist flexion angles obtained in the Burnett and Campbell-Kyureghyan study were substantially different from those determined in this study. During this study, the average wrist angles for all scans were in extension. In the Burnett and Campbell-Kyureghyan study, the average wrist angles for the left and right abdominal scans were in flexion. 9 The differences for the wrist angles could be a result of the anatomy scanned, the position of the patient, or the self-selected position of the sonographer. Another explanation of the differences could be the presence of the pressure mat wrapped around the transducers as part of the partner study measuring pressure on the transducers. 10 The sonographers were instructed to scan without repositioning their fingers on the pressure mat during the scan. The participants may have scanned with more extreme wrist extension angles than they otherwise would have if they had been able to reposition their hands on the transducers during the scan.
A limitation of the present study was the participant sample size. Further research with a larger number of participants would provide the ability to draw statistically significant conclusions regarding the kinematic differences due to scanning factors, such as scanning seated or standing, transducer design, patient positioning, and right or left kidney scanned. Another difficulty involved the inability of the cameras to detect the forearm markers at times during the scans due to the posture assumed by the sonographers. Experience in diagnostic medical sonography was a variable not addressed that also could have had an influence on the kinematics in this study.
Conclusion
The present kinematic evaluation concluded that the sonographers were scanning with their shoulders in flexion, abduction, and external rotation; with their elbows in flexion; and with their wrists in extension for most of the scanning procedures. Shoulder abduction and wrist extension exceeded published acceptable limits during all the scans.12,15 The shoulder and elbow joint angles determined for this study with a 3D motion capture system were similar to the joint angles determined by other researchers in a previous study using electrogoniometers. 9 These kinematic results could be used to improve the working environment and transducer design, which could minimize therisk of musculoskeletal work-related disorders in sonographers.
Footnotes
Appendix
This appendix contains additional technical details regarding the determination of the reference frames and joint angles. Anatomical reference frames were determined for the thorax and upper arm to create a shoulder joint transformation matrix:
where
where
The dot product was used to calculate the elbow joint angle:
where
The equation used to determine the flexion/extension angles at the wrist was
where
A proximal plane was defined as the plane that passes through the elbow joint center and the medial and lateral wrist markers, thus dividing the forearm into anterior and posterior sections (Appendix figure). The normal vector to the proximal plane can point in either the posterior direction (up in Appendix figure) or the anterior direction (down in Appendix figure). The normal vector was calculated as the result of the cross product of two vectors lying in the proximal plane,
If the resulting normal vector was pointing posteriorly, the wrist was in extension. If it was pointing anteriorly, the wrist was in flexion. To determine whether the normal vector was pointing posteriorly or anteriorly, it was compared to a vector known to be pointing in the posterior direction,
The direction of the normal vector to the proximal plane was determined with the following equation:
If d was negative, then the normal vector pointed anteriorly, the wrist was in flexion, and the sign was 1. If d was positive, then the normal vector pointed posteriorly, the wrist was in extension, and the sign was −1.
A continuity test was applied to the wrist joint angles because, in some instances, it would suddenly change from extension to flexion or vice versa in a single frame of data collection. The sudden changes were investigated with the hand and forearm markers in Vicon Nexus software, in which the wrist did not transition between extension and flexion. The continuity test applied prevented the wrist joint angle from transitioning between flexion and extension if it acquired an angular velocity of more than 500° per second.
Acknowledgements
The following individuals provided invaluable assistance with this project: Lauren Vetter, Hannah Bullock, Chad Conroy, Lynn Carlton, and Rick Carlton.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially funded by a fellowship awarded under the National Science Foundation American Recovery and Reinvestment Act of 2009 (Public Law 111-5), grant No. ARRA 1011221, to Samhita Rhodes, PhD, and John Farris, PhD.