
Abstract
As the population ages, sonographers will be required to do increasing numbers of examinations for patients undergoing dialysis. The hemodynamic changes that result from the placement of an arteriovenous fistula (AVF) or a dialysis access graft in the upper extremity can significantly influence the final diagnosis of an extracranial carotid arterial sonographic evaluation. The case study presented demonstrates the importance of obtaining a complete patient history on the resulting differential diagnosis.
Keywords
While a checklist-type patient history may represent a good starting point, in many cases, it is not adequate to properly interpret the findings of a complex sonographic examination. 1 A detailed history enables the professional sonographer to complete a thorough, accurate evaluation. The interpreting physician can then develop a differential diagnosis from this study that enables the referring physician to initiate and plan the appropriate management and treatment for the patient. If the sonographer performing the initial examination has complete and accurate patient history information, an accurate diagnosis can be developed that will often alleviate unnecessary additional testing. Two case studies are presented below that will demonstrate the impact a thorough patient history has on the resulting diagnosis.
Case Reports
Methods
For both case studies, the carotid duplex ultrasound examination was done using a Philips IE-33 (Philips Ultrasound, Bothel, WA, USA) with a linear array transducer (bandwidth 3-9 MHz) as well as a curved linear array transducer (bandwidth 3–6 MHz). The vessels were examined in multiple planes from the subclavian artery throughout the extracranial extent of the carotid and vertebral arteries according to the Society for Vascular Ultrasound guidelines. 2
Case Report 1
A 67-year-old man had several near syncopal episodes over the preceding one month. The patient had a history of cardiac bypass surgery done five years ago. The patient also had a history of smoking one to two packs of cigarettes per day for 40 years and had been treated for hypertension and dyslipidemia over a period of 25 years. During the physical examination, auscultation of the right carotid artery revealed a bruit, and a carotid duplex ultrasound examination was ordered to evaluate for obstructive disease.
Cross-sectional imaging of the right side showed a mild heterogeneous atheromatous plaque in the right common carotid artery (RCCA), external carotid artery (RECA), and internal carotid artery (RICA) that did not reduce the diameter of the vessels significantly.3,4 Spectral Doppler waveforms taken from these segments showed minimal spectral broadening throughout and peak systolic velocities less than 120 cm/s, characteristic of a less than 50% stenosis in the RICA using our diagnostic crieria. 3 The right subclavian artery demonstrated a diffuse heterogeneous atherosclerotic plaque (Figure 1), a monophasic spectral Doppler waveform with spectral broadening, and elevated peak systolic velocities of 330 cm/s (Figure 2). Further investigation with the curved linear array transducer to improve depth penetration helped to better define the plaque seen as well as confirm the elevation in the peak systolic velocity (Figure 3). Evaluation of the left subclavian artery showed a significantly lower peak systolic velocity of 179 cm/s and a normal high-resistance multiphasic waveform without spectral broadening (Figure 4).3,5
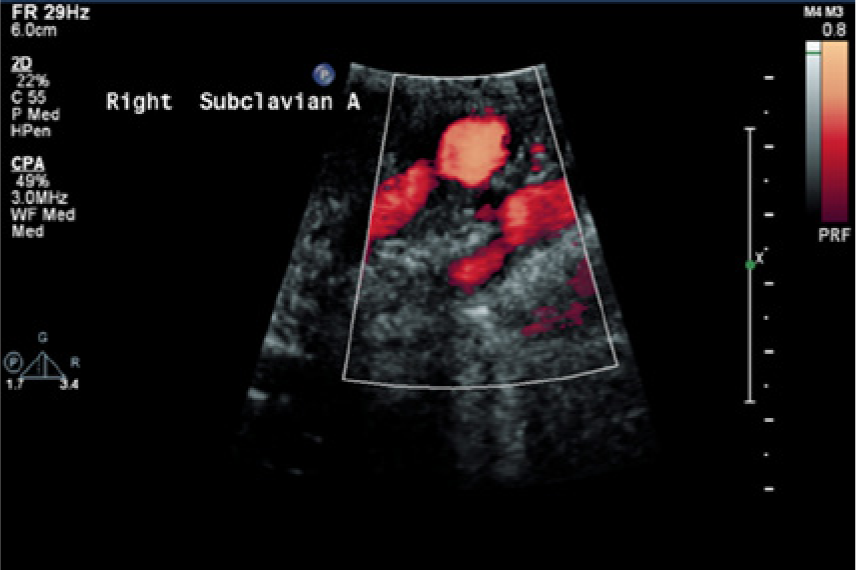
A sagittal power Doppler image of the right subclavian artery in case 1 showing a diffuse atherosclerotic plaque with narrowing seen in the proximal artery.
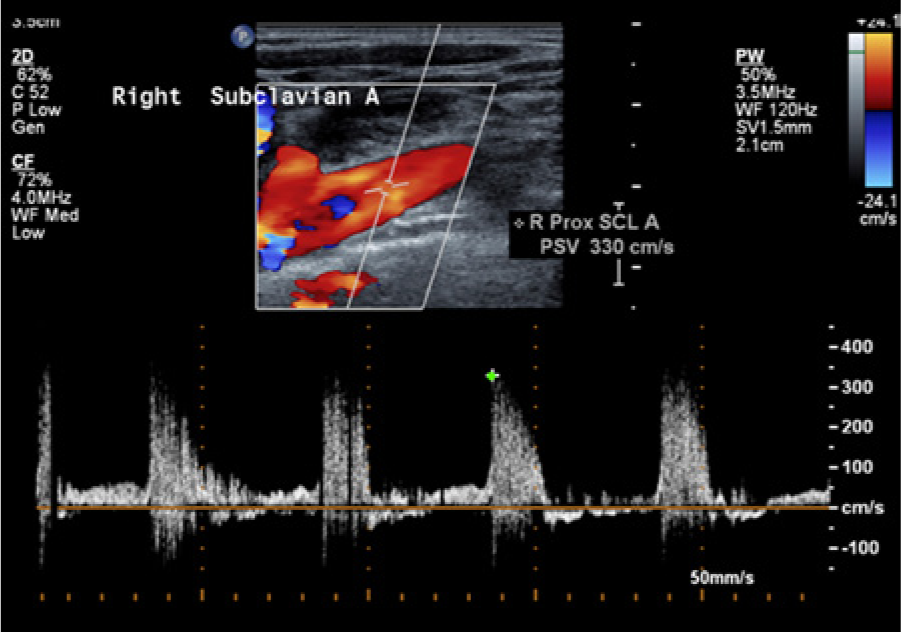
Color Doppler image with spectral Doppler waveform near the origin of the right subclavian artery in case 1 showing an elevated peak systolic velocity of 330 cm/s with accompanying spectral broadening throughout the systolic phase of the cardiac cycle.
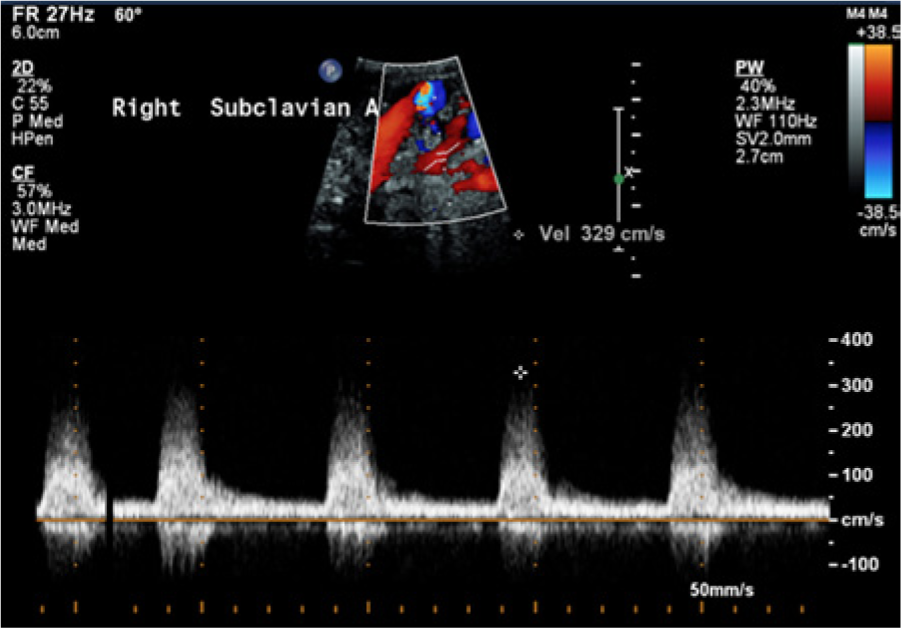
A similar image to Figure 2 but taken using a lower frequency curvilinear probe to improve depth penetration, confirming narrowing of the proximal right subclavian artery and an elevated peak systolic velocity with significant associated spectral broadening.
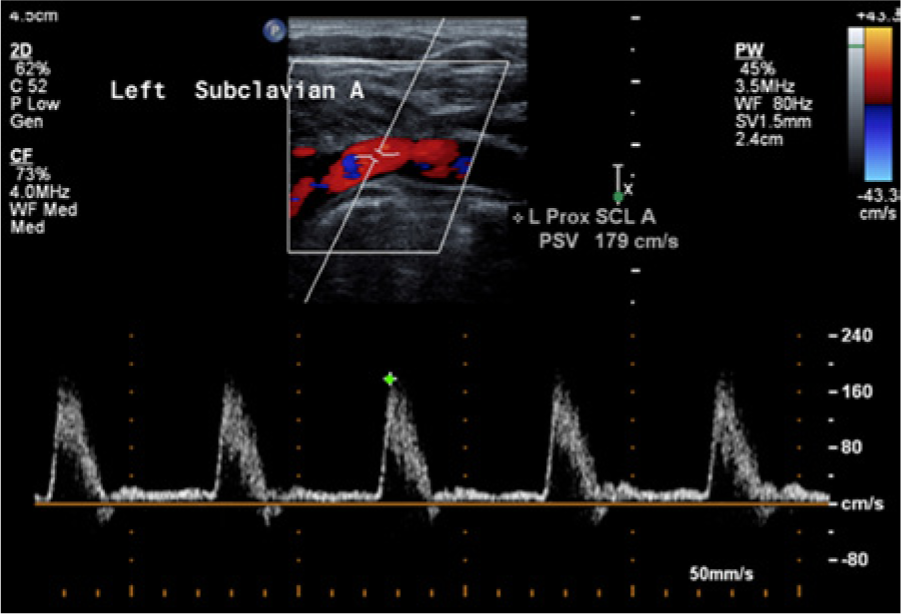
Color and spectral Doppler image of the contralateral normal left subclavian artery in case 1, showing a multiphasic flow signal and no spectral broadening.
On the basis of these findings, the patient was referred to an independent imaging center for a computed tomographic angiography (CTA). The results of the CTA showed a 70% stenosis at the origin of the right subclavian artery, which was considered the source of the right bruit auscultated during the initial physical examination.
Case Report 2
A 58-year-old female patient experienced headaches and two episodes of syncope over the previous month. Past history included smoking one pack of cigarettes a day for approximately 20 years, quitting at age 38 years. The patient had ongoing treatment for hypertension, dyslipidemia, and diabetes over a period of 25 years. The patient developed renal failure five years ago and had an arteriovenous fistula (AVF) placed in her right upper extremity for dialysis. During the physical examination, a right carotid bruit was auscultated and a carotid duplex ultrasound examination was ordered.
B-mode imaging of the right side showed minimal atherosclerotic plaque in the RCCA, RECA, and RICA and an anatomically normal-appearing right subclavian artery (Figure 5). Spectral Doppler evaluation of the right subclavian artery showed an elevated peak systolic velocity of 210 cm/s, spectral broadening, and a monophasic-appearing waveform characteristic of a focal stenosis. Color Doppler imaging did not show any turbulence in the vessel, however. It was felt in this case that the presence of the AVF in the right upper arm was the probable cause for the alteration of the normal hemodynamics of the right subclavian artery that mimicked stenosis, and the origin of the right carotid bruit was attributed to the hyperdynamic flow state (Figure 6). 6
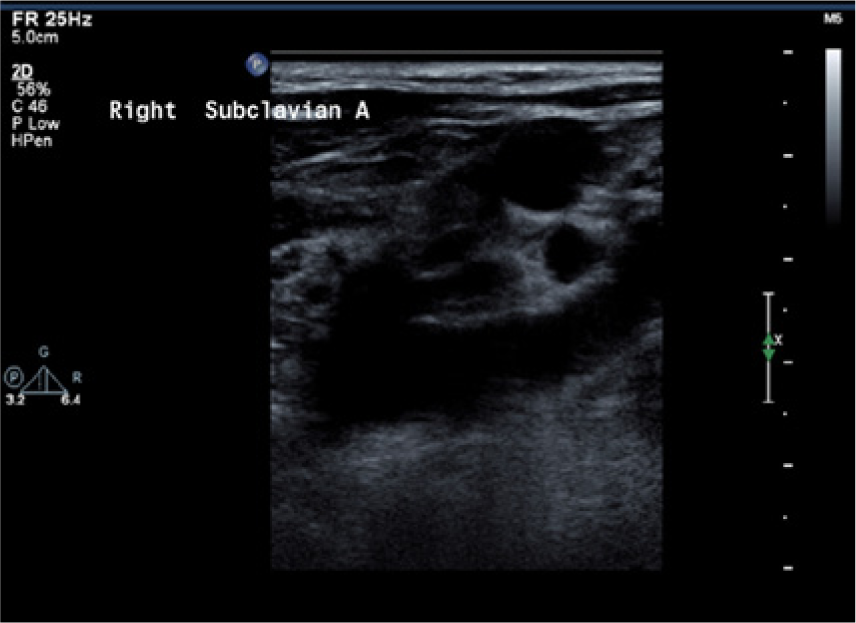
Sagittal B-mode image of the right subclavian artery in case 2 with no evidence of any significant atherosclerotic disease, kinking, or narrowing.
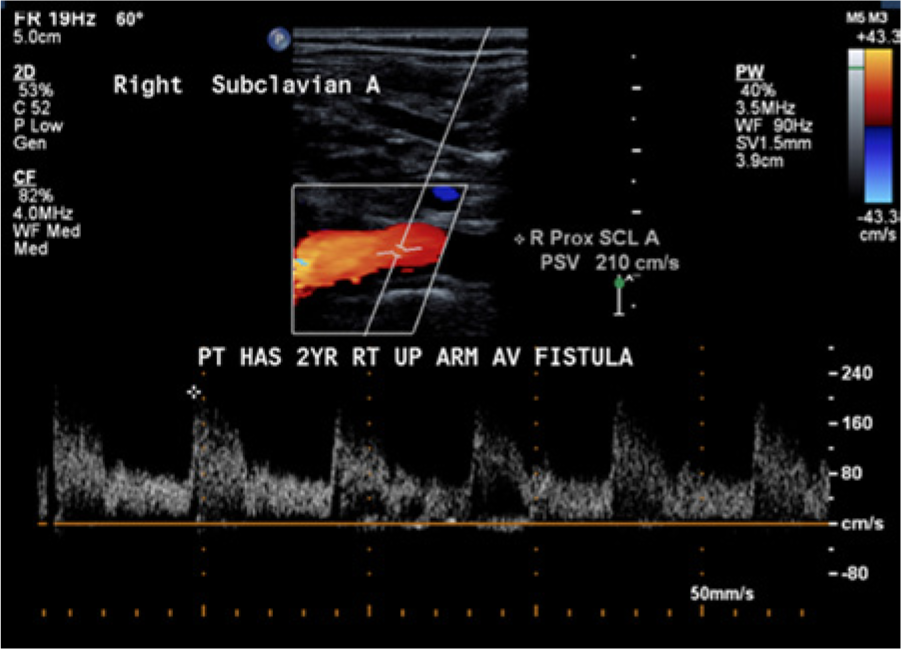
Color and spectral Doppler image of the right subclavian artery in case 2 showing the presence of an elevated peak systolic velocity with associated spectral broadening secondary to hyperdynamic flows related to a right upper arm arteriovenous fistula.
Discussion
The Society for Vascular Ultrasound has published the “Vascular Technology Professional Performance Guidelines: Extracranial Cerebrovascular Duplex Ultrasound Evaluation.” 2 Guideline 2 of this document recommends that patient assessment be done prior to the performance of the examination. A complete, relevant history should be obtained from the patient, the patient’s representative, or medical record.
Sonographers frequently encounter patients who are not capable of giving an accurate history. It is not uncommon that even the representative accompanying the patient is unaware of many important health issues. In these cases, detailed examination of the patient’s general appearance may reveal valuable insight. Is the patient ambulatory? Does the patient exhibit any weakness or paralysis of the extremities? Is the patient aphasic? Are there scars from a previous carotid endarterectomy or other vascular procedure? When documenting upper extremity blood pressures, do the systolic pressures differ between the right and left arms? Is there an AVF or dialysis access shunt present? These preliminary observations and assessments in conjunction with all the available patient history, both from the patients themselves and from any available medical records, allow for a determination that the test ordered is the appropriate one and to focus the examination for optimal quality.
In the two cases above, important risk factors for carotid stenosis were present, including smoking, male sex (in case 1), hypertension, and dyslipidemia.3,5,6 Based on these patient histories and the bruits found during the physical examinations, a carotid duplex ultrasound was the examination indicated to evaluate for obstructive disease in the effort to prevent a transient ischemic attack or stroke. 6 An incomplete history might have hindered the ability of the interpreting physician to evaluate the examination data accurately. A sonographer in “picture-taking mode” may simply breeze through the examination and not identify the key details that will lead the physician to the correct diagnosis without additional testing, time, and expense that is critical to patient care.
The sonographer must have a thorough knowledge and understanding of hemodynamics and pathophysiology to be able to adapt to a variety of clinical conditions and presentations. Bruits over the carotid artery are a graphic case in point. They could originate anywhere from a cardiac source in the chest, for example, secondary to an aortic stenosis, to a narrowing of the distal internal carotid artery high in the neck as would be found in fibromuscular dysplasia. They might also arise from non–carotid artery sources in the neck, such as secondary to the turbulent flows created in the subclavian artery by an upper extremity AVF. Duplex ultrasound examinations have become the first test ordered in such cases and provide a reliable, noninvasive method of evaluating patients who may not be able to tolerate radiographic examinations requiring contrast because of other health issues.
In case 1, the B-mode visual documentation of significant atherosclerotic plaque, the narrowing of the vessel noted with color Doppler imaging, and the elevated peak systolic velocity with associated spectral broadening caused by the turbulence of the blood flow through the area of narrowing met criteria indicating the need for additional testing to confirm the presence of a right subclavian stenosis.3,5,7 In case 2, a right upper arm AVF was documented during the initial physical examination in addition to the presence of a right carotid bruit. The B-mode examination of the right subclavian artery did not document any significant plaque, kinking, or narrowing. There were, however, elevated velocities and a monophasic-appearing waveform with spectral broadening that typically are indications of the presence of stenosis.2,5 In this situation, the right carotid bruit auscultated during the physical examination was the hemodynamic result of hyperdynamic flows caused by the AVF in the right upper arm; the bruit was transmitted through the neck from its origin within the subclavian artery to the right carotid artery. The thorough history taken at the onset of the carotid ultrasound examination enabled the correct diagnosis to be determined without additional testing, time, and expense to the patient.
Conclusion
A sonographer who uses a superficial or nonsystematic approach toward the process of obtaining a patient history can cause diagnostic inaccuracies when the interpreting physician does not have all the information necessary to determine the cause of abnormalities. This, in turn, may lead to the ordering of unnecessary additional testing or delays in vital therapeutic decisions. In the cases presented, case 1 demonstrated a true stenosis of the proximal portion of the right subclavian artery, with an appropriate follow-up procedure (CTA) to confirm the presence and severity of the stenosis. Prior knowledge of the presence of an AVF in the right upper extremity in case 2 was used to explain the hemodynamic abnormalities and eliminated the need for any follow-up angiography. Case 2 presents an example of a “pseudo-stenosis” of the subclavian artery caused by increased flows related to an upper arm AVF. Although the subclavian artery spectral waveforms were similar in these two cases, the cause of the increased velocities, spectral broadening, and monophasic flow waveform were significantly different. The thorough history taken prior to the performance of the carotid duplex ultrasound examination in case 2 alleviated the need for any additional testing.
The significance of compiling a thorough patient history prior to beginning any diagnostic sonographic procedure cannot be overstated. A misdiagnosis and the performance of unnecessary, costly, potentially painful, and possibly dangerous additional procedures can be averted. The ability to systematically evaluate each facet of the examination and to arrive at the diagnosis sometimes requires thinking “out of the box.” Critical thinking and evaluation of the entire clinical picture are essential skills that are characteristic of professional sonographers, not “picture takers.”
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.