
Abstract
Objectives:
Squamous cell carcinoma in a thyroglossal duct cyst is exceedingly rare with only 26 reported cases in the literature so far, which only account for 6% of the patients.
Methods:
We report a unique case of squamous cell carcinoma arising from a thyroglossal duct cyst in a 49-year-old male who was primarily diagnosed as a thyroglossal duct cyst with inflammation. The patient underwent Sistrunk procedure with wide local excision and radiation therapy as well as chemotherapy post-operatively and had no evidence of recurrence or metastasis for 24 months. In addition, we reviewed the relevant literatures.
Results:
Whether squamous cell carcinoma actually arises from thyroglossal duct cyst is still controversial; however, carcinoma originating from metaplasia of columnar and squamous epithelium in thyroglossal duct cyst has been well accepted. The gold-standard diagnostic method is fine needle aspiration biopsy with ultrasound guidance. Sistrunk procedure alone or with wide excision is likely to be beneficial. Neck dissection is necessary in patients with positive cervical lymphadenopathy. Radiation therapy and chemotherapy have not yet been clearly defined.
Conclusion:
Squamous cell carcinoma arising from thyroglossal duct cyst is really a rare disease, whose origin, treatments and prognosis still remain uncertain. These are solely based on case reports, case series and expert opinions. Hence, more investigations about squamous cell carcinoma will be conducted in the near future.
Introduction
Malignancy of the thyroglossal duct cyst (TGDC) is rarely seen, occurring only in approximately 1% of cases. To date, approximately 250 cases have been reported, among which a majority of these cases were diagnosed either as papillary carcinomas (PC) or follicular carcinomas (FC), while only around 5% were squamous cell carcinomas (SCC). 1 As far as we know, there have been 26 cases of SCC reported so far, including 21 cases of SCC, three cases of SCC with PC, and two cases of adenosquamous carcinoma (ASC) (Table 1).2–7 Here, we report a case in which the patient had SCC arising from the TGDC, and a review of the literature to shed light on the current SCC diagnosis and treatment.
Summary of detailed literature on patients with squamous cell carcinoma of thyroglossal duct cyst.
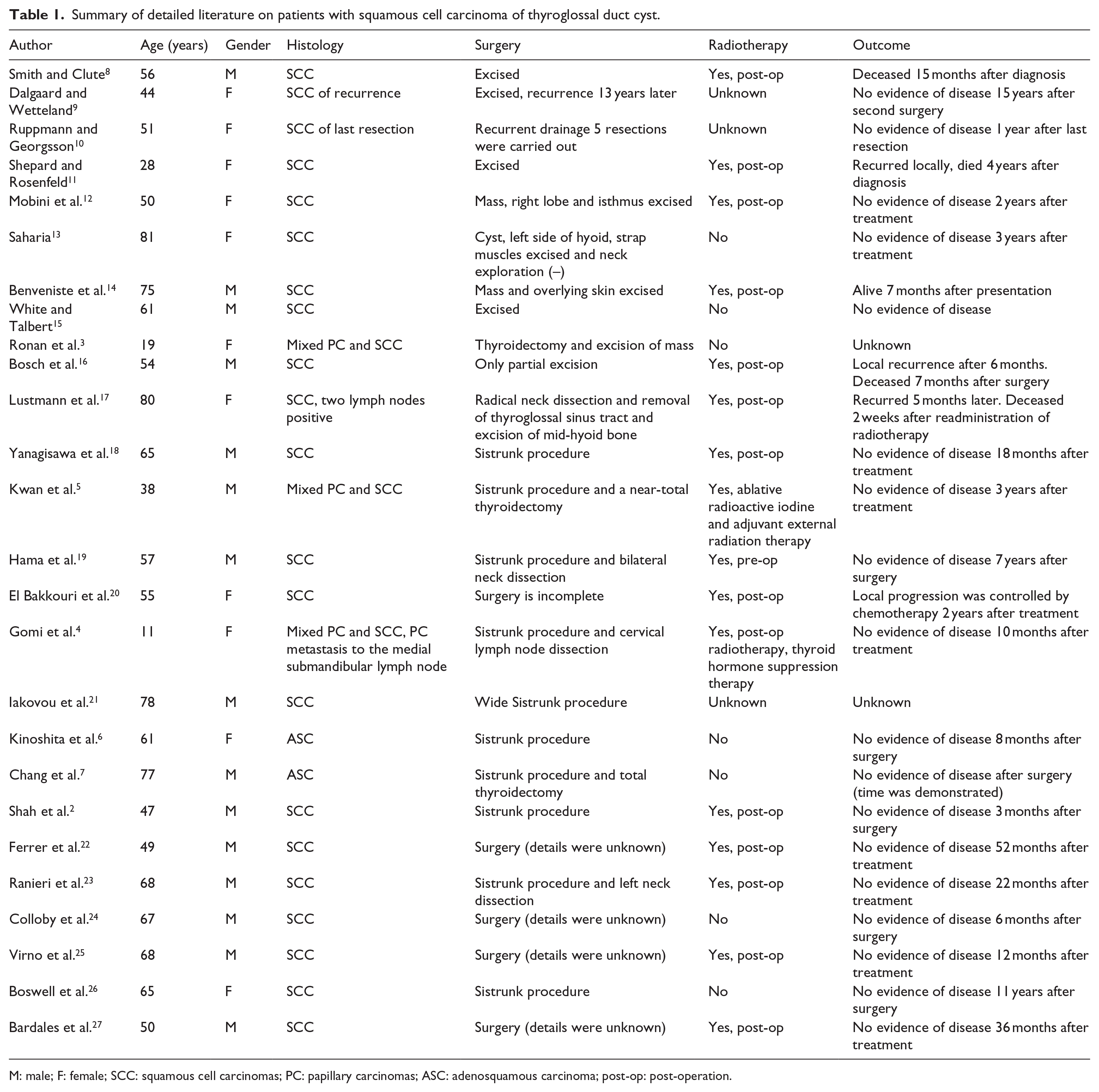
M: male; F: female; SCC: squamous cell carcinomas; PC: papillary carcinomas; ASC: adenosquamous carcinoma; post-op: post-operation.
Case report
A 49-year-old male with a background of infantile paralysis presented with a midline anterior neck mass with associated pain, inarticulacy and swallowing discomfort. Despite a 2-week course of oral antibiotics, there was no significant improvement in the clinical symptoms. The patient was originally diagnosed with TGDC 4 years prior, but he declined for surgery at that stage. On examination, he had a tender, hard midline anterior neck mass (6.0 × 4.0 × 4.0 cm) at the level of hyoid bone that elevated on swallowing (Figure 1). On nasal endoscopy, no abnormality was found in his nasal, oral, pharyngeal or laryngeal areas. Ultrasonography demonstrated a solid-cystic multilocular mass (5.8 × 3.6 cm) with irregular shape and well blood supply connecting with hyoid bone. Magnetic resonance imaging (MRI) without contrast was guided for inspection due to iodine allergy. MRI showed a 5.6 × 3.2 × 3.6 cm lesion with mixed signals and unclear margins. The lesion appeared to arise from notch thyroid and extend to midline tongue base (Figure 2). There was no evidence of abnormal thyroid gland and cervical lymphadenopathy. Based on these findings, a TGDC with inflammation was suspected, and Sistrunk procedure was consented. However, intra-operatively, the mass was found to adhere densely with surrounding tissues. Thus, Sistrunk procedure with additional wide local excision was performed. In view of the large open wound cavity in proximity to the floor of mouth and potential laryngemphraxis post-operatively, tracheotomy was performed following surgery, with nasogastric tube inserted. The tracheotomy and nasogastric tubes were removed 1 week after surgery without any complications. The mass specimen was sent for histopathological review. Grossly, the mass (6.0 × 4.0 × 4.0 cm) composed of chief solid lesion with partial cystic lesion adhering to hyoid bone and surrounding muscles (Figure 3). Microscopically, the mass presented numerous differentiated malignant squamous cells (Figure 4). Whole body positron emission tomography (PET) scanning did not reveal any regional or distant metastatic diseases (Figure 5). Based on these findings, this mass was diagnosed as SCC arising from a TGDC. The patient made an unremarkable post-operative recovery and underwent further chemotherapy (docetaxel, 75 mg/m2 (Day 1) and cis-platinum, 70 mg/m2 (average Days 1–3), every 3 weeks, total twice) and radiotherapy with 60 Gy of intensity dividing into 30 fractions. Following radiotherapy, the patient had no evidence of recurrence or metastasis for 24 months.

A tender, hard, midline anterior neck mass (circle) at the level of the hyoid bone.

(a) MRI T2-weighted sections in axial plane and (b) sagittal plane shows a lesion with mixed signals and no clear margins arising from notch thyroid and extend to midline tongue base.
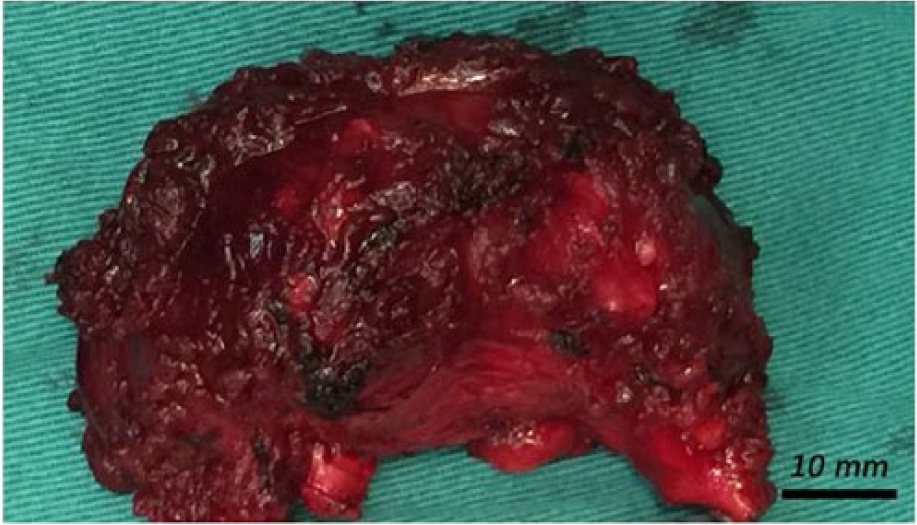
The excised mass that was found to adhere to the hyoid bone and surrounding muscles.

(a) Histopathological image of the mass specimen demonstrating the fibrous stroma with invasive nests of atypical squamous cells (H&E, ×20). Immunohistochemically, positivity for (b) CKpan, (c) 34bE12 and (d) p40 was observed in the invasive tumor nests confirming squamous cell carcinoma (×20).

No regional or distant metastasis was revealed by PET scan.
Discussion
During the third week of fetal life, thyroid gland arises embryologically from a midline endodermal invagination of the foregut at the level of the foramen cecum. Its tract of descent from the base of the tongue to the final resting place in the anterior neck involutes in the ninth week of gestation. However, when the tract fails to involute, thyroglossal duct remnant forms and mainly presents as a cyst named TGDC which accounts for over 70% of anterior neck masses in children and 7% in adults.28,29 However, carcinoma arising within TGDC is exceedingly rare, with a low morbidity of 1% and only approximately 250 cases reported. 1 A majority (over 50%) of these TGDCs contain ectopic functional thyroid tissue.29,30 Hence, more than 90% of these patients have been described as well-differentiated PC, 1 and only 6% have been indicated as SCC. 31
More than 50% of TGDCs have normal thyroid cells, thus PC arise de novo from the TGDC rather than metastatic spread from the main gland. The lack of parafollicular cells in ectopic thyroid tissue of these malignancies provides further evidence for this theory.32,33 However, whether the SCC actually arise from TGDC is still controversial. Thus far, two theories have been put forward. Numerous reports have revealed that SCC combining with PC arises from TGDC.3–5 Ronan et al. 3 even reported a transition between the two components. Therefore, one theory indicates that SCC is possibly a metaplastic component of PC. 5 In contrast, another theory states that metaplasia of columnar and squamous epithelium in TGDCs plays a key role in carcinogenesis since TGDCs consist of columnar and squamous epithelial cells and previous reports indicated only SCC in TGDCs. 19 It is most likely that tumor originated from metaplasia of columnar and squamous epithelium rather than metaplasia of PC. 6
Generally, TGDC presents as an asymptomatic midline neck lump in the region of hyoid bone. Symptoms predominantly include dyspnoea, dysphagia or dyspepsia, especially when the mass becomes larger in size although extremely rare. When a patient has a history of hoarseness, weight loss or airway compromise, he or she should be suspected for malignancy. In addition, if the lump is hard, fixed, irregular or associated with lymphadenopathy, there should be a high index of suspicion for malignancy. 28 SCC arising from TGDC is best evaluated by cross-sectional imaging modalities such as computed tomography (CT) and MRI. The gold-standard diagnostic method is fine needle aspiration biopsy (FNAB) with ultrasound guidance. Moreover, intra-operative frozen section is beneficial to minimize the necessity for neck re-exploration and to determine the diagnosis during initial surgery. 28 Although reports in the literature are rare, strict criteria for primary diagnosis of SCC in TGDC have been defined as follow: (1) the carcinoma locates in the wall of TGDC, (2) a transition between epithelium of the cyst and the carcinoma and (3) excluding diseases which could mimic diagnosis such as carcinoma in tongue base and mouth floor.2,12
To date, there have been only several cases reported with varied operative procedures. Therefore, evidence-based management protocol is difficult to be established. Management for patients with TGDC SCCs is Grade C, since it is solely based on case reports, case series and expert opinion. 34 Thus, the standard management protocol for SCC from TGDC is still not yet clear. However, Sistrunk procedure alone or together with wide excision is likely to be beneficial. Patients with clinically positive cervical lymphadenopathy may require neck dissection intra-operative, while the strategy of dealing with thyroid gland is controversial. Since Kwan and colleagues’ review, there have been 12 published cases summarized in Table 1 (the present case is the 13th). In brief, eight patients underwent Sistrunk procedure alone, and three patients experienced Sistrunk procedure with wide excision. Two patients underwent partial excision, four patients experienced Sistrunk procedure with cervical lymph node dissection, one patient had Sistrunk procedure with lobe and isthmus excised, one patient had Sistrunk procedure with thyroidectomy and four patients’ details of their surgeries were unknown. SCCs involving PC in TGDCs have been reported by three cases (Table 1), and thyroidectomy or near-total thyroidectomy of thyroid gland is carried out in two cases except the 11-year-old child who has no obvious pathology in thyroid gland.
In literatures, it has been indicated that staging systems for the differentiated thyroid cancer of the main gland can be applied to TGDC carcinomas. Moreover, the TNM (tumor, nodes, metastasis) staging system is recommended for uniformity. 28 Furthermore, the adjuvant therapies have been introduced including total or near-total thyroidectomy, radioactive iodine (RAI) and thyroid-stimulating hormone (TSH) suppression. 35 Nevertheless, these treatments may be unsuitable for the treatment of TGDCs with SCC specifically. Post-operative radiotherapy has been indicated for larger lesions, but this treatment has not yet been clearly defined. Several reports have demonstrated recommendations of radiation for patients who have not had an oncologic resection and for those with positive margins. 2 No clear guidelines exist regarding criteria for post-operative chemotherapy when surgery and radiotherapy are both not effective. 20 In the literatures, 15 patients of SCC in TGDC underwent post-operative radiotherapy, while one patient was treated by radiotherapy preoperatively. By contrast, seven patients have no radiotherapy, and another three patients lack the relevant records. Only one patient underwent post-operative chemotherapy attributing to the failure of surgery and post-operative radiotherapy.
The prognosis of TGDC malignancy is based on several factors, including extent of surgery, tumor stage and histology. The more common PC has a good prognosis owing to complete excision, RAI and TSH suppression. In comparison, the prognosis of SCC is harder than PC and remains uncertain due to its small case number. In the literature, the best outcome reported is of a patient without evidence of recurrence over 15 years post surgery. While the worst outcome reported is that of a patient with TGDC SCC recurred 5 months post-operatively, and passed away 2 weeks after radiotherapy. Hence, clinicians should be aware of these issues, and long-term follow-up is paramount for patients with TGDC SCC. 19
Conclusion
SCC arising from TGDC is really a rare disease, whose origin, treatments and prognosis still remain uncertain. These are solely based on case reports, case series and expert opinions. Hence, further researches are required to better delineate management guidelines for this rare and controversial malignancy.
Footnotes
Acknowledgements
Q.H. and Y.S. contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the institutional review board and ethics committee of Ningbo Medical Center Lihuili Eastern Hospital (approval number: 2017-33)*.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.