
Abstract
Objective
The incidence of thyroglossal duct diseases in the general population is about 7%. We aimed to demonstrate the clinical presentations and management of thyroglossal duct diseases.
Methods
We conducted a retrospective review of all patients who underwent surgery for histopathologically confirmed thyroglossal duct cyst, sinus, or fistula at a single center.
Results
A total of 151 cases were included in this study. There were more female patients (87, 58%) than male patients (64, 42%). The patients’ ages ranged from 1 to 63 years old. The most prevalent complaint was painless upper midline neck swelling (93.3%). Most cases were diagnosed as thyroglossal duct cysts (137, 90.7%). Six cases (4%) were associated with carcinoma. All the cases were managed using the modified Sistrunk procedure. There were no procedure-related complications, and five cases of recurrence.
Conclusions
Although thyroglossal duct cyst is the most common neck anomaly in children, it may also present with various characteristics later in life. This condition can be managed successfully without complications and with a low recurrence rate.
Keywords
Introduction
Thyroglossal duct (TGD) cysts (TGDCs) are atypical thyroid gland remnants that can occur anywhere along the thyroid migration route. 1 After its formation, the thyroid gland starts to descend into its final anatomical location during the first 6 weeks of gestation, and the TGD then undergoes total atrophy up to the tenth week. Failure of complete involution of the TGD results in TGDC.2,3 It is the most common type of congenital neck mass in children, and its incidence in the general population is about 7%. 4 In pediatric patients, TGDCs have been reported to mainly affect male patients, whereas adult cases are predominantly female. 5 The region below the hyoid bone is the most common origin of TGDCs. 6 The symptoms of this condition may differ, and cysts arising from the intralingual region may cause dysphagia, choking, and dysphonia. 7 This congenital anomaly might also be associated with various complications, such as severe infection, local inflammation inducing pain and swelling, malignancy, and fistula formation.7,8 A wide variety of presentations and complications of TGDC have been reported in the literature. 9 Its appropriate treatment requires a thorough understanding of the anatomy and embryology of the thyroid gland, hyoid bone, and tongue. The modified Sistrunk procedure is the main treatment for TGDC, but different outcomes have been reported in the literature.10,11
The current study aimed to demonstrate the clinical presentations and management of thyroglossal duct disease in a single center, and to compare them with the literature.
Methods
Study design
We conducted a retrospective review of all patients who underwent surgery for TGDC, thyroglossal duct sinus (TGDS), or thyroglossal duct fistula (TGDF) at a single center between December 2017 and June 2022. The study was approved by the ethics committee of the University of Sulaimani (reference number 117/2022). All patient details were de-identified to protect patient privacy. Verbal consent to participate was obtained from all patients and their families and written consent for publication was obtained from cases whose figures or images were used in this study. The reporting of this study conforms to the PROCESS guidelines. 12
All patients with confirmed histopathology of TGDC, TGDS, or TGDF were included in this study. Patients with suspicious histopathology for TGDC, TGDS, or TGDF, incomplete data, abnormal thyroid function tests, or neck swelling for other reasons were excluded.
Data collection
All the required data, including demographics, symptoms, physical examination, related investigations (thyroid-stimulating hormone, triiodothyronine, and thyroxine), ultrasonography findings, fine needle aspiration (FNAC) findings, histopathological diagnosis, operation type, operation time, complications, and recurrence, were collected by reviewing the patient’s clinical files extracted from the center’s electronic database. FNAC was conducted for cases with suspicious thyroid nodules or lesions on ultrasonographic examination.
Intervention
All procedures were performed under general anesthesia in a supine position with an extended neck, after skin preparation and disinfection. A subplatysmal skin flap was raised through a transverse upper neck incision over the most prominent part of the mass. The cyst plus surrounding tissues were dissected up to the hyoid bone, and the infrahyoid muscles (mostly sternohyoid and thyrohyoid muscles) were divided. The central part of the hyoid bone was resected along with the included intact tract. The suprahyoid muscles (mostly geniohyoid and mylohyoid muscles) were divided from the hyoid, and the tract with the surrounding tissues was dissected up to the foramen caecum (Figures 1 and 2). Adjacent tissues were also removed because of the possibility of multiple tracts, which might otherwise lead to recurrence or fistula formation (Figure 3). One of the assistant surgeons was asked to apply digital pressure over the base of the tongue near the foramen caecum to facilitate the dissection and to confirm the reach up to the foramen caecum. The tract was then ligated at the foramen caecum and removed.

Dissection of track with adjacent tissues up to the foramen caecum.

Specimen of thyroglossal duct cyst after the modified Sistrunk procedure.

Modified Sistrunk procedure for thyroglossal duct cyst.
Data interpretation
The data were recorded using Microsoft Excel (2019) and a descriptive analysis was carried out using SPSS version 25 (IBM Corp., Armonk, NY, USA).
Results
A total of 151 cases were included in this study. The patient characteristics are presented in Table 1. Female patients predominated over male patients for both children and adults. Sixty-seven patients (45%) were considered to be children (<14 years old). The most common presenting symptom was painless upper midline neck swelling, and the most common preoperative ultrasonographic findings indicated TGDC, TGDS, and TGDF. Most TGDCs measured between 1 and 10 cm3. Most cases were diagnosed postoperatively by histopathology as TGDC, followed by TGDF and TGDS. Six cases (4%) of TGDCs were associated with papillary thyroid carcinoma (PTC), as suspected by preoperative ultrasonography and confirmed by FNAC or histopathology. All patients were treated using the modified Sistrunk procedure, and the six cases with carcinoma underwent additional total thyroidectomy. The operation time ranged from 30 to 180 minutes (mean 51 minutes). There were no procedure-related complications, and five cases (3.3%) had recurrence.
Baseline characteristics, operations, and outcomes.
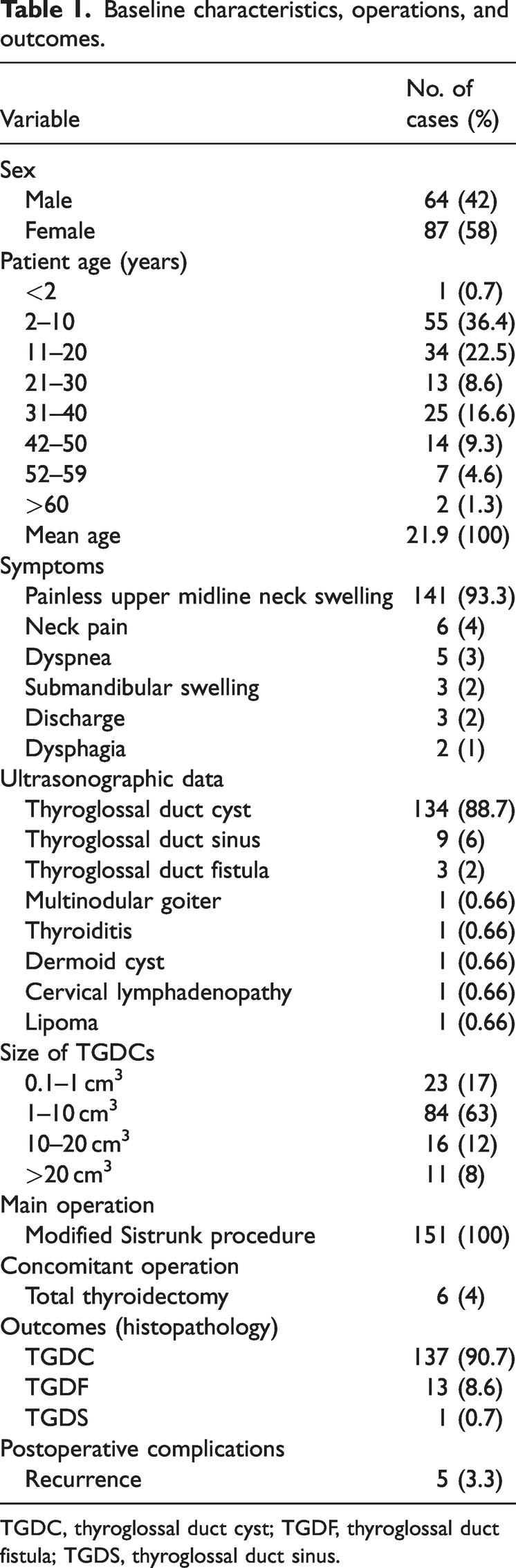
TGDC, thyroglossal duct cyst; TGDF, thyroglossal duct fistula; TGDS, thyroglossal duct sinus.
Discussion
As a thyroid gland remnant, TGDCs can form at any site along the thyroid gland migratory route. 13 This condition usually presents in children, but can also occur in adults. 14 However, it is difficult to determine an accurate age distribution for TGDC because of the different time intervals of reporting; it may be reported as the time of initial diagnosis or the onset of symptoms, while some authors may report the decade of life, instead of the exact age of the patient. There is thus a lack of consensus regarding the demographic distribution of TGDCs among the reported studies. The mean age of patients in the current study was 21.9 years and most were in their first and second decades of life, in accordance with previous studies.11,15,16 However, around 1.6% of patients were older than 60 years, in contrast to the literature, which rarely mentioned the occurrence of this anomaly in elderly patients and estimated its incidence as 0.6% in patients over the sixth decade of life.11,17 In addition, our findings also contradicted previous findings in terms of the sex distribution, with most studies reporting an equal sex distribution,11,13 while female patients outnumbered male among both children and adults in the present study.
Various symptoms are associated with TGDC, including neck swelling, dyspnea, dysphagia, and dysphonia, while a painless anterior neck mass is the most common presentation during physical examination.9,13 Several factors have been reported as indications for the excision of TGDC, such as globus sensation, dyspnea, dysphagia, pain due to mass effect, malignancy, and cosmetic defects. 18 In this study, painless upper midline neck swelling was the most common symptom at the time of presentation, followed by neck pain.
TGDC is the most prevalent type of congenital abnormality of thyroid development, but it is rarely associated with carcinoma. 19 In this study, the incidence of carcinoma within TGDC was 4%, and all carcinomas were PTC, in line with a previous study that also noted PTC as the most frequent carcinoma found in TGDC, followed by squamous cell carcinoma and some others like Hürthle cell carcinoma, follicular, and anaplastic thyroid carcinoma. 20 The frequency of primary carcinoma within TGDCs in all cases undergoing TGDC removal was reported to range from 0.7% to 1.6%, although another study reported a higher rate of >6%.20,21 Two major theories have been proposed for the origin of TGDC-related carcinomas. The de novo theory states that ectopic thyroid tissue may be identified histopathologically in >60% of TGDCs, and carcinomas may thus originate from the ectopic thyroid tissue rather than from the TGDC.19,22 In contrast, the metastatic theory suggests that TGDC-related carcinomas represent metastatic events from an occult primary thyroid gland. Furthermore, the TGD is thought to provide a natural pathway for the spread of thyroid carcinoma.23,24 There are controversies regarding the management of TGDCs associated with carcinomas: some authors support total thyroidectomy immediately after the diagnosis, while others do not recommend this course of action.20,25 The current study supported total thyroidectomy, and all patients with TGDC with carcinoma underwent this procedure because of the suspicion of metastasis.
A better understanding of the anatomy of the TGD anatomy makes surgical removal of the cysts much easier, and extensive work has accordingly been carried out, notably by Schlange and Sistrunk. Shlange initially proposed a technique to remove the middle third of the hyoid bone, and succeeded in decreasing the rate of recurrence from 50% to 20% in comparison with simple cyst drainage. Sistrunk subsequently developed the technique by extending the dissection to the foramen caecum, and the recurrence rate was reduced further to about 5%. The Sistrunk procedure consists of three major steps: excision of the cyst, excision of the hyoid bone body, and excision of the core tissue surrounding the thyroglossal tract from the tongue muscles close to the foramen caecum.26,27
The modified Sistrunk procedure has been reported to be a safe technique with minimal complication rates. In a study that included pediatric patients, the total rate of minor complications was about 29%, with seroma being the main complication, followed by wound infection and stitch abscess. 28 Another study, mostly involving adults, reported only seroma (3.8%) as a complication, and the recurrence rate in adults was 5.8%. 29 A recurrence rate of 3.4% following the modified Sistrunk procedure has also been reported. 30 Local wound infection and seroma were the most common complications of the modified Sistrunk procedure. 4 Galluzzi et al. 31 found a 10.7% recurrence rate in children who underwent TGDC surgery. Some authors reported that preoperative infection could increase the risk of recurrence,4,31 and several other factors have also been shown to affect the recurrence rate, including previous surgery, inadequate excision, age <2 years, absence of preoperative imaging, and an inexperienced surgeon.4,10,18 No specific complications were encountered in the current study and the total recurrence rate was 3.3%. These results may be due to all the procedures being carried out by specialized and experienced surgeons in the field, the lack of cases with preoperative infection, appropriate preoperative imaging, and the fact that only one case was <2 years old.
Dermoid cysts and TGDCs have similar appearances and can thus often be misdiagnosed preoperatively. For this reason, some surgeons prefer to perform cystectomy instead of the modified Sistrunk procedure. Despite this, Geller et al. reported that one case of lingual TGDC was initially misdiagnosed as a vallecular cyst in their study, 9 and one case in the current study was initially suspected as a dermoid cyst.
The major limitations of this study were the small sample size, short-term study, lack of proper design, and limited data analysis to identify any significant patterns.
Conclusion
Although TGDC is the most common neck anomaly in children, it may also present with various characteristics much later in life. However, this condition can be managed successfully, with no complications and a low recurrence rate.
Research Data
Research Data for Thyroglossal duct diseases: presentation and outcomes
Research Data for Thyroglossal duct diseases: presentation and outcomes by Aso S. Muhialdeen, Abdulwahid M. Salih, Mohsin M. Ahmed, Yadgar A. Saeed, Aras J. Qaradakhy, Hiwa O. Baba, Ari M. Abdullah, Fahmi H. Kakamad, Shvan H. Mohammed, Dilan Sarmad Hiwa, Mohammed Subhan Mohammed and Zana Baqi Najmadden in Journal of International Medical Research
Footnotes
Author contributions
Aso S. Muhialdeen, Abdulwahid M. Salih, Mohsin M. Ahmed, Yadgar A. Saeed, and Hiwa O. Baba all made major contributions to the study conception, performed the operations, followed up the patients, and provided final approval of the manuscript. Aras J. Qaradakhy (radiologist) performed the assessments and provided final approval of the manuscript. Ari M. Abdullah (pathologist) examined the specimens and provided final approval of the manuscript. Fahmi H. Kakamad, Shvan H. Mohammed, Dilan Sarmad Hiwa, Mohammed Subhan Mohammed, and Zana Baqi Najmadden performed the literature review, wrote the manuscript, and provided final approval of the manuscript.
Data availability statement
All data and materials are kept by the first and corresponding authors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.