
Abstract
This case study describes a patient who underwent an upper extremity venous examination to evaluate for possible deep vein thrombosis (DVT). Sonography showed no evidence of thrombus in the veins of the deep or superficial system. Adjacent to the veins of the peripheral arm, however, an enlarged hypoechoic structure was visualized that had a very similar appearance to DVT. With further imaging, hyperechoic linear bands were visualized at the proximal end of the hypoechoic structure. The appearance suggested that this structure was related to the median nerve, but its normal appearance was altered by a large mass inside the nerve sheath. Given the patient’s history, the finding most likely represents a nerve hematoma.
Keywords
Sonographers must be able to recognize normal anatomical features and structures in the area of interest so that any abnormality is recognized and fully documented to prevent potential misdiagnosis. In the case described here, a possible misdiagnosis of upper extremity deep vein thrombosis was avoided by recognition of the characteristics of surrounding anatomic structures.
Case Report
A 60-year-old male presented with right upper extremity pain and swelling above the antecubital fossa, accompanied by numbness and tingling in his fingertips. The patient reported that intravenous access in the area of the antecubital fossa had been attempted but was not successful. The patient underwent an upper extremity venous examination to evaluate for possible deep vein thrombosis (DVT) in his right arm. The patient had no history of DVT.
Sonography showed no evidence of acute DVT in the central veins bilaterally. Gray-scale imaging showed normal compressibility at all accessible sites and anechoic vessels. Color Doppler imaging showed the veins filling normally, and spectral Doppler waveforms showed normal pulsatility and respiratory phasicity, all characteristics of a normal venous system. The peripheral veins were imaged only on the symptomatic right side. The right brachial and cephalic veins were compressible, showing no sign of thrombus. Medial to the normal basilic vein was an enlarged hypoechoic structure measuring 5.4 × 1.4 cm (Figure 1) that had the sonographic appearance of a DVT. In the transverse plane, the structure proved to be noncompressible. This structure was also imaged in the longitudinal plane, and color Doppler imaging was used. Color Doppler imaging showed an avascular structure with no evidence of color flow, so the possibility of DVT could not be ruled out. Alternating hyperechoic linear bands were visualized at the proximal end of the hypoechoic mass–like structure (Figure 2). The alternating hypoechoic and hyperechoic bands appeared to represent fascicles, typical of the sonographic appearance of a nerve. Given the sonographic findings and the visualization of normal upper extremity deep and superficial veins, the structure was identified as the median nerve, whose normal appearance was altered by a large mass located inside of the nerve sheath. Because of the patient’s history, the mass was believed to most likely represent a hematoma of the median nerve, although the possibility of a nerve sheath tumor could be excluded. Follow-up with sonography was recommended to evaluate for any progression of the lesion. Unfortunately, the patient was discharged shortly after the diagnosis was made, and he did not return to our facility for follow-up so no additional information could be obtained.
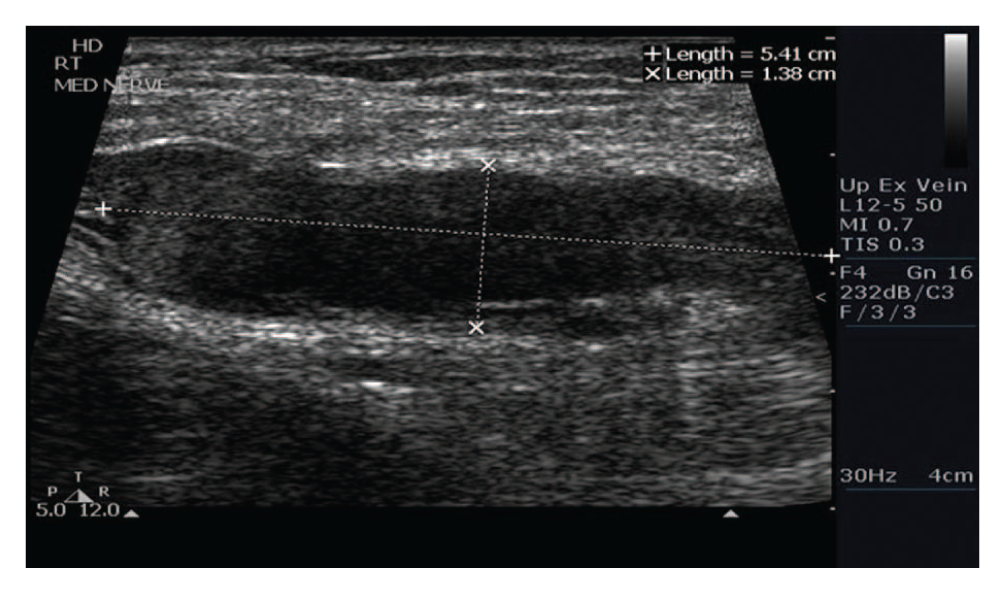
Longitudinal gray-scale image of the median nerve hematoma measuring 5.4 × 1.4 cm. The image demonstrates an enlarged hypoechoic appearance that is similar to the sonographic appearance of deep vein thrombosis.
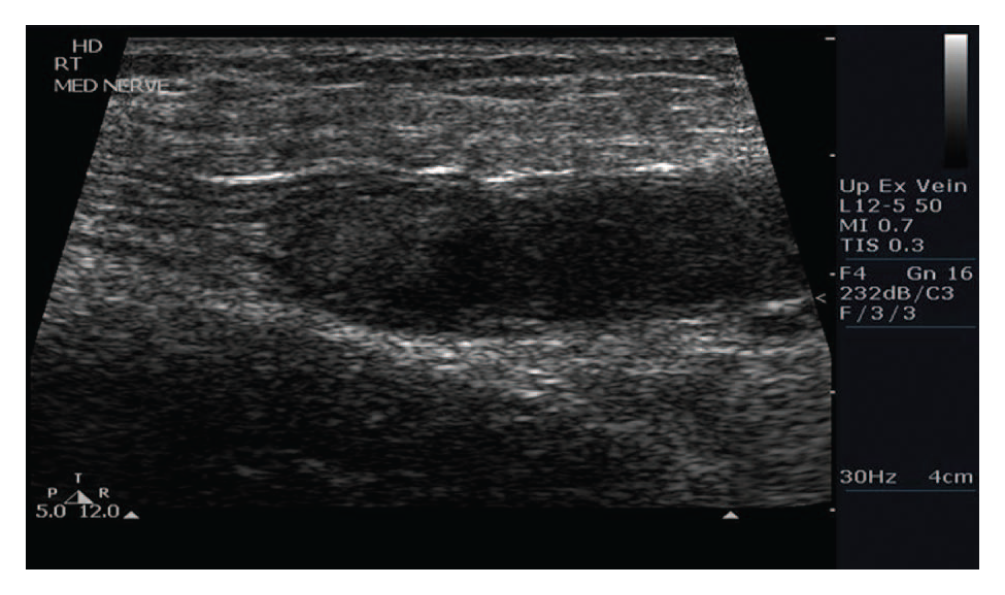
Longitudinal gray-scale image of the median nerve hematoma, showing alternating hyperechoic linear bands that represent fascicles visualized at the proximal end of the hypoechoic mass–like structure. This is a typical nerve appearance and indicates the involvement of the median nerve as opposed to deep vein thrombosis.
Discussion
Sonography of the peripheral nerves is well documented in the literature, but this is the first known documentation of a nerve hematoma mimicking deep venous thrombosis. While previous authors have commented on the different abnormalities found in the peripheral nerves, this is the first to describe an upper extremity mass mimicking DVT. Sonography, being a relatively low-cost and noninvasive examination, is the preferred study for ruling out DVT and therefore is typically the first study performed for pain and/or swelling of the upper extremity. The current gold standard for nerve evaluation is electromyography, although it has many limitations and many of its tests are invasive. The use of high-frequency ultrasound allows for direct evaluation of the nerve and tendons during active and passive flexion and therefore is ideal for looking at these structures. 1 Nerves are soft, flexible structures, and their shape may vary from round to oval depending on the width of the anatomic passageways through which they pass. Anatomically small nerves may be difficult to distinguish from small vessels; therefore, image characteristics as well as spectral and color Doppler analysis all play a critical role in distinguishing a blood vessel from a nerve so that a nerve is not mistaken for DVT. 2 The sonographic appearance of nerves is that of parallel lines separated by hyperechoic bands on a long axis (Figure 3). With finger flexion, the associated tendons shift ventrally and then dorsally, but the median nerve remains in place with minimal movement. 1
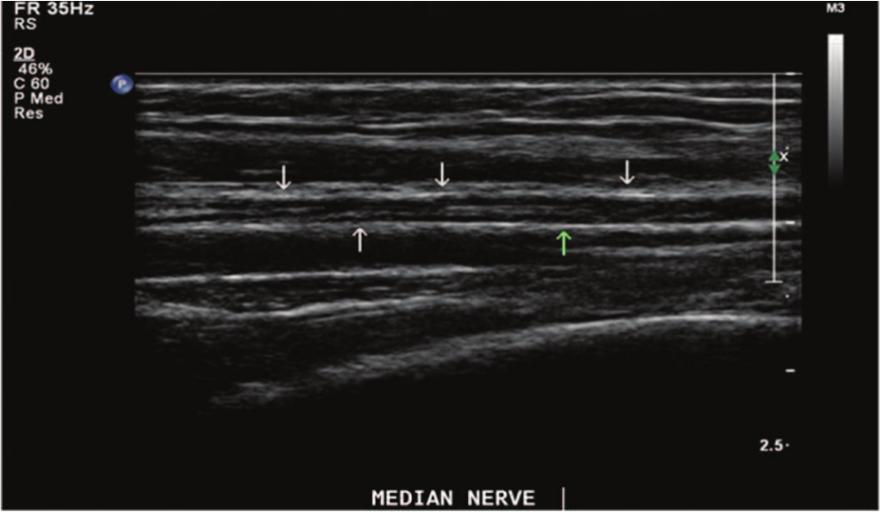
A longitudinal gray-scale image of a normal median nerve. The median nerve shows multiple hypoechoic bands representing fascicles and parallel, discontinuous lines separated by echogenic bands that correspond to the outermost layer of the nerve (arrows).
Nerves have a very distinct appearance when they are normal, but with injury or disease their appearance can be altered and they can be confused with other anatomic structures. Pino et al 3 described a tibial nerve schwannoma, a benign nerve sheath tumor, that was found during an examination for DVT. Chuang et al 4 described iatrogenic median nerve hematomas caused by catheterization of the brachial artery, noting that serpiginous brachial arteries or anticoagulation therapy increases the risk for traumatic nerve injury during catheterization procedures. Auyong et al 5 described sonographic guidance for nerve blocks and reported 2 cases of non-nerve-related incidental findings noted during the procedures—an incidental mass and an abscess. Other related articles have described the wide variety of nerve masses that are readily evaluated with sonography, including neurofibromas, ganglia, and other neurogenic lesions.2,6-8
Iatrogenic nerve injuries can be caused by routine procedures such as venipuncture or insertion of peripheral intravenous (IV) catheters. Nerve injury can be caused when too steep an angle of insertion is used for peripheral access devices or when repeated probing actions are performed with the needle. Once the nerve is injured, the patient frequently complains of radiating numbness and tingling near the site of injury or an immediate “electric shock” sensation that runs down the arm. 9 In the upper extremities there are numerous nerves, with the largest being the median nerve, typically found in the central portion of the antecubital fossa and terminating where it branches in the palm. During phlebotomy procedures or when peripheral access devices are inserted, it is frequently the median nerve that is injured.
Another potential cause of nerve injury is compartment syndrome. Compartment syndrome occurs when there is increased pressure extrinsic to the blood vessels and nerves within a limb compartment that is enclosed and constrained by fascia. This increase in extrinsic pressure can be caused by the collection of blood, IV fluids, or medications in the closed space or by increased intracompartmental muscle edema secondary to trauma, which then leads to elevated tissue pressure and ultimately tissue ischemia and nerve compression. Iatrogenic compartment syndrome occurs when adequate pressure is not applied to an arterial or venous puncture site, which can lead to the formation of a hematoma, causing a delayed nerve compression injury after the blood collection procedure once the blood in the tissue coagulates. 9
Traction injuries also may change the sonographic appearance of a nerve and may mimic DVT. Significant traction injury can cause the outer nerve sheath to be disrupted, which can create a partial nerve tear and result in a spindle neuroma. Neuromas appear as an irregular fusiform hypoechoic swelling along the course of the nerve, very much like the appearance of an acute DVT. Contusion injuries can occur when a nerve impinges against a bony surface or a fracture fragment, leading to the development of a segmental fusiform thickening of a nerve at the site of contusion. Contusions may further lead to nerve swelling and hypoechoic changes related to friction neuritis.
There are 2 benign forms of peripheral nerve sheath tumors, the schwannoma and neurofibroma, which usually originate from neural or Schwann cells. 2 These nerve sheath tumors can have a very similar appearance to DVT, as seen in Figure 4. 10 Other masses that may be related to the nerve include paragangliomas, lymphomas, and hemangiomas. 2
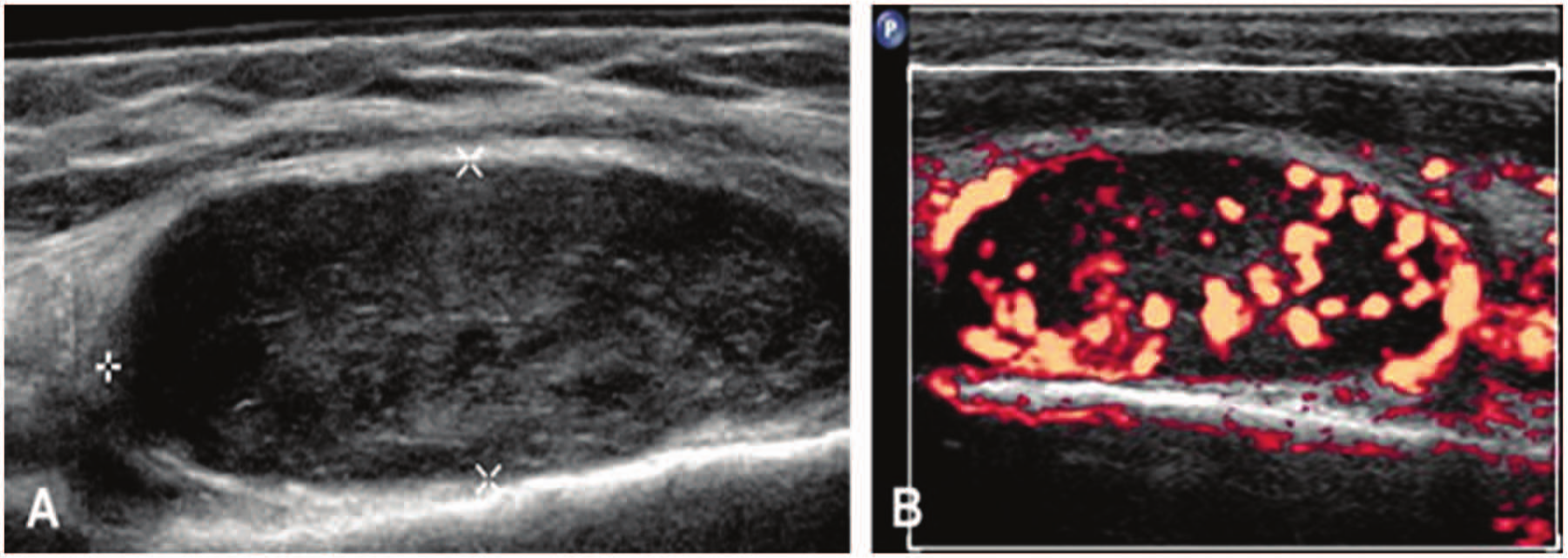
(A) A longitudinal gray-scale image of a hypoechoic mass–like structure. (B) The mass is imaged with power Doppler, and significant vascularity is apparent. The mass was a biopsy-proven benign nerve sheath tumor, very similar appearance to DVT. Reprinted with permission from Masoorli. 9
Due to their sonographic similarities, in this particular case a nerve hematoma could have been easily mistaken for DVT. Both may appear “spongy” 11 and have internal echoes. The incidence of upper extremity DVT (UEDVT) has significantly increased in recent years with the increasing use of central venous catheters. 12 Patients with UEDVT typically present with arm swelling, pain, redness, and/or venous enlargement and may complain of a feeling of tightness that worsens on exertion. 13 Patients with secondary UEDVT may have risk factors such as indwelling central venous catheters, pacemakers, or active malignancy or may be undergoing chemotherapy. This is not a benign finding, as the incidence of pulmonary embolus with UEDVT is 12% to 16%, 14 and there is a high incidence of postthrombotic syndrome. 13 There is significant overlap in UEDVT symptoms and nerve hematoma symptoms, such as pain and swelling, although UEDVT would be less likely to present with tingling and numbness. Color and spectral Doppler can be used to look for internal flow, as might be seen with a solid mass like a nerve tumor, or to look for flow around a nonocclusive DVT.5,14 When a patient is evaluated for suspected DVT, the upper extremity vessels should be followed with gray-scale graded compression and spectral and color Doppler to evaluate for intraluminal thrombus. Extrinsic compression resulting from a mass impinging on the vein can both cause DVT and mimic the continuous spectral Doppler flow pattern seen with more central DVT, so if abnormal flow is detected it is important to evaluate for both intraluminal and extraluminal causes. 15 Other potential differential diagnoses for an upper extremity mass include pseudoaneurysm, adenopathy, soft-tissue tumors, and muscle tears. 16 In this particular case study, the sonographer, who was trained in musculoskeletal ultrasound and has experience with nerve imaging, recognized that the mass was extrinsic to the basilic vein and was related to the nerve.
Conclusion
In the case presented here, the sonographer recognized normal and abnormal nonvascular structures and documented a nerve injury that could easily have been mistaken for UEDVT. Over the coming years, sonography will continue to be the primary diagnostic technique for peripheral DVT and will likely gain ground as the preferred test for muscle and nerve-related disorders. Sonographers will be called upon to document these disorders and certainly will benefit from knowledge of the vascular and nonvascular structures of the extremities; sonographic results will help clinicians arrive at the correct differential diagnosis and determine appropriate patient management. Having an accurate clinical history is also important in reaching the proper sonographic diagnosis, and this needs to be a routine part of all examinations. The sonographer is an important member of a patient’s health care team and shares responsibility for assessing patients so that adverse events or iatrogenic injuries are recognized and treated appropriately.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.