
Abstract
Internal iliac artery aneurysms are rare and seldom imaged with sonography in an acute situation. This case study illustrates a ruptured internal iliac artery aneurysm and shows the correlation of sonographic images with computed tomographic images in an emergent setting.
Introduction
Internal iliac artery aneurysms are rare and are not commonly imaged with ultrasound because most patients reporting acute symptoms are imaged primarily with computed tomography. In the case reported here, the patient presented first to the ultrasound department from the emergency department. As described in the following, sonography showed findings consistent with an iliac artery aneurysm, which prompted further emergent imaging.
Case Report
A 78-year-old male presented to a rural emergency department with acute onset of persistent left lower quadrant and hip pain, made worse by walking and relieved by rest. The patient was alert, oriented, and suffering moderate nausea at the time of the visit, but showed no other visible symptoms. Although the patient height and weight were not taken due to the acuity of his symptoms, he was noted to be of large body habitus. The patient history was notable for an abdominal aortic aneurysm repair 16 years prior, though the exact type of surgical repair was not known. Other pertinent medical history included chronic atrial fibrillation, hypertension, hyperlipidemia, and well-controlled type II diabetes mellitus. The patient had been a smoker with cessation 12 years prior. His daily medications included warfarin and aspirin. Distal pulses in the legs were reported as normal during the physical examination and his blood pressure was noted to be 120/75 mmHg. Laboratory results were remarkable for a positive d-dimer, elevated serum blood urea nitrogen and creatinine levels, and normal hemoglobin but slightly low hematocrit as well as red blood cell and platelet counts. Urinalysis was normal.
Sonographic Findings
The patient was referred to the ultrasound department for an aorto-iliac examination to evaluate for possible recurrence of an abdominal aortic aneurysm. The examination was performed on a Philips iu22 using a 5 MHz curvilinear transducer. Sonography showed a normal distal aorta, a poorly visualized common left iliac artery ending in a 7.5 cm complex cystic structure with internal blood flow (Figures 1 and 2), and a normal left external iliac artery distal to this with a normal, triphasic pulsed-wave Doppler flow pattern (Figures 3 and 4). Findings were reported by the radiologist as suspicious for common iliac artery aneurysm.

Transverse view of the left iliac region of the pelvis with calipers indicating the margins of the complex mass.
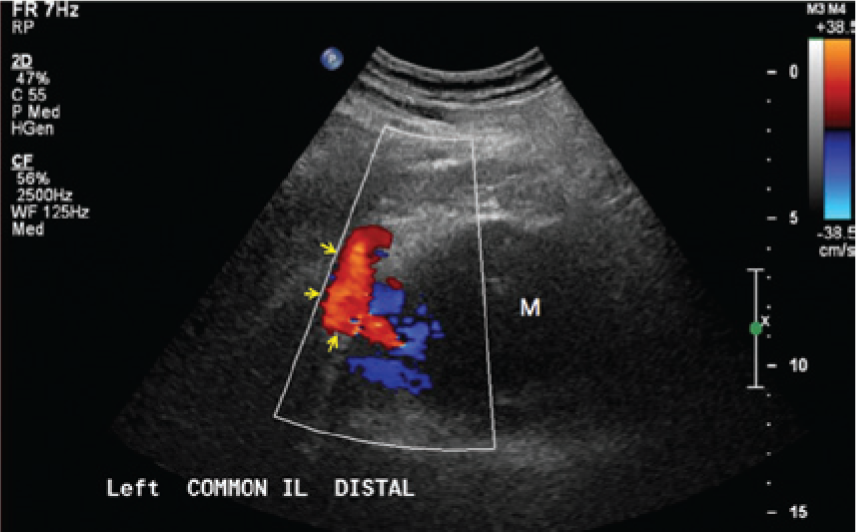
Sagittal color Doppler image of the common iliac artery leading into the area of the pelvic mass (M).
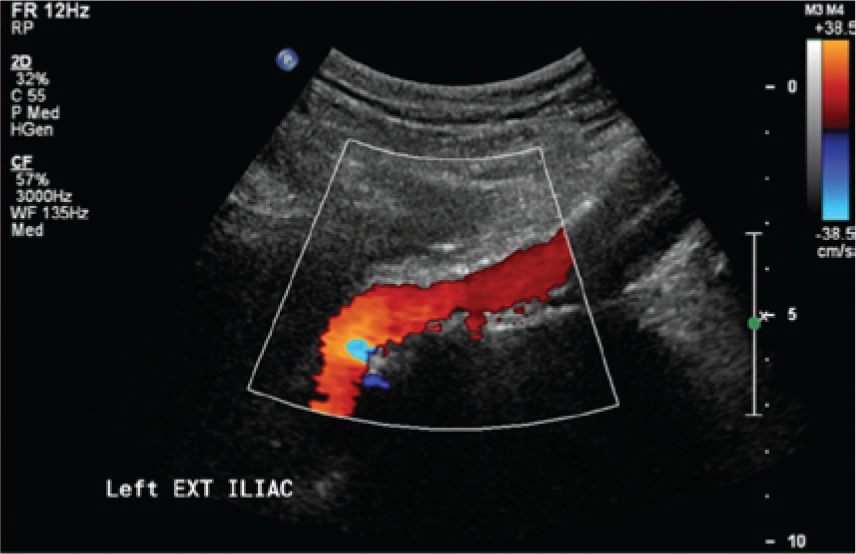
Sagittal color Doppler image of the left external iliac artery distal to the mass.
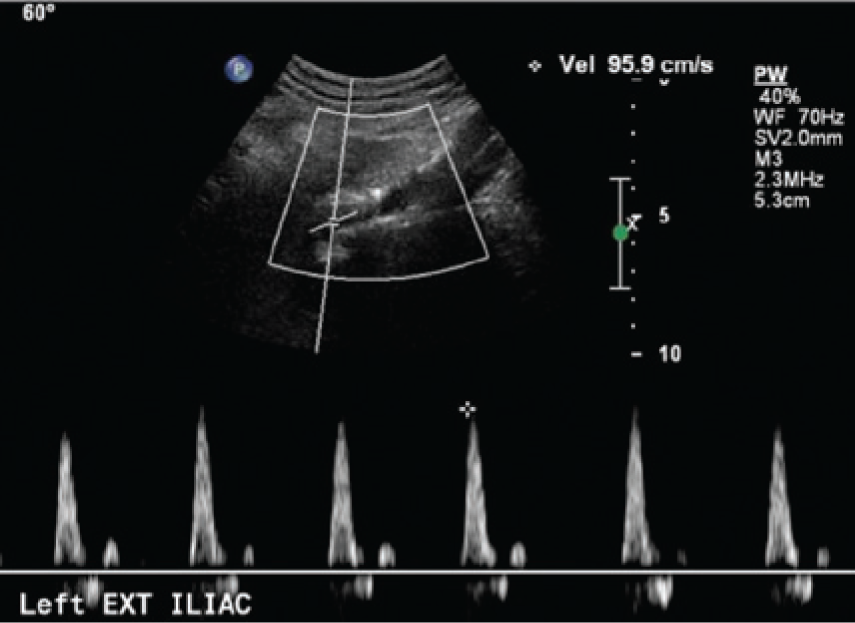
Pulsed-wave spectral Doppler recording of the external iliac artery confirming normal triphasic arterial flow distal to the mass.
Computed Tomography Findings
The patient was then referred to computed tomography (CT) for a noncontrast abdominal and pelvic CT examination to confirm a common iliac artery aneurysm. CT findings showed a large, 8.5 × 8.0 cm internal iliac artery aneurysm just past the iliac bifurcation (Figures 5, 6, and 7). Additional note was made of bilateral common iliac artery aneurysms of 2.5 and 2.6 cm. Mild to moderate left renal hydronephrosis indicated possible extrinsic compression of the left ureter by the internal iliac artery aneurysm. Accumulation of fluid in the surrounding tissues characteristic of a retroperitoneal hematoma (Figure 8) suggested acute rupture of the aneurysm, and the patient was scheduled for immediate transfer to a tertiary care facility for vascular surgery. Ultimately the patient suffered cardiac arrest en route to surgery and was unable to be revived.
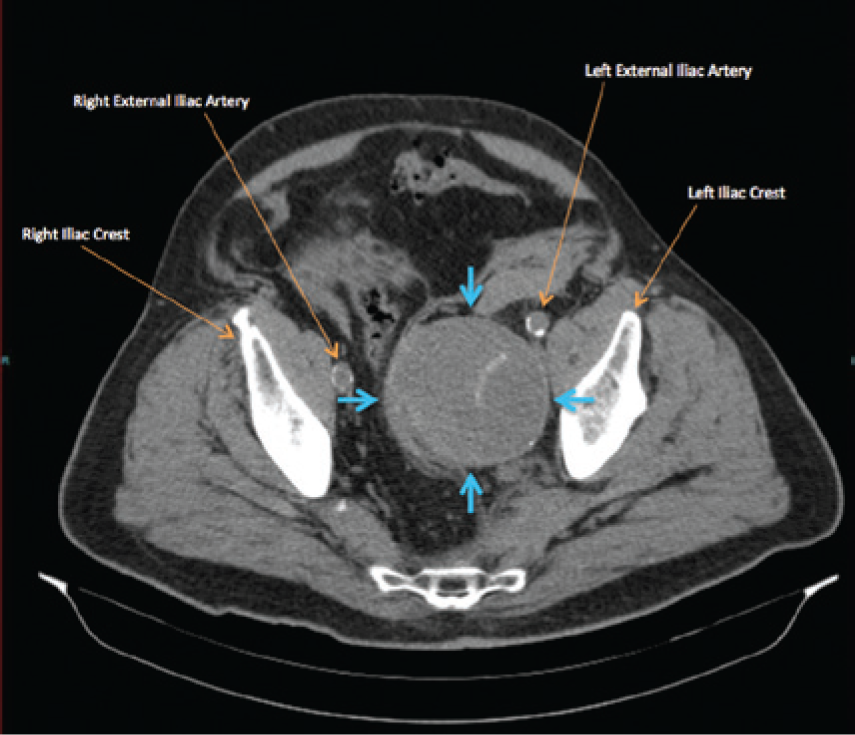
Cross-sectional noncontrast computed tomography image showing the left internal iliac artery aneurysm just past the iliac bifurcation (blue arrows).
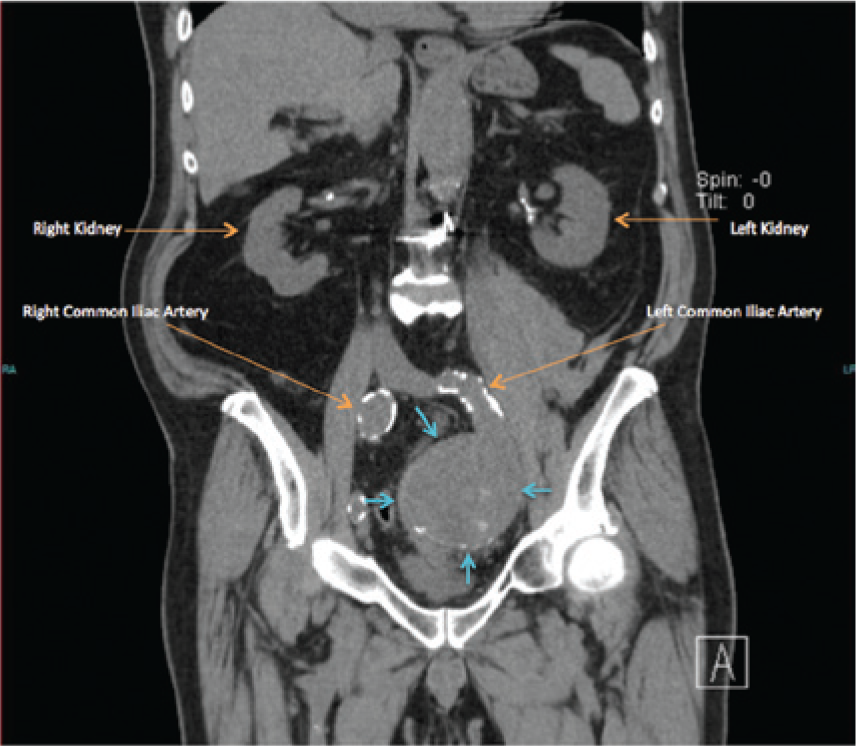
Coronal noncontrast computed tomography reconstruction showing the aneurysmal left internal iliac artery (blue arrows).
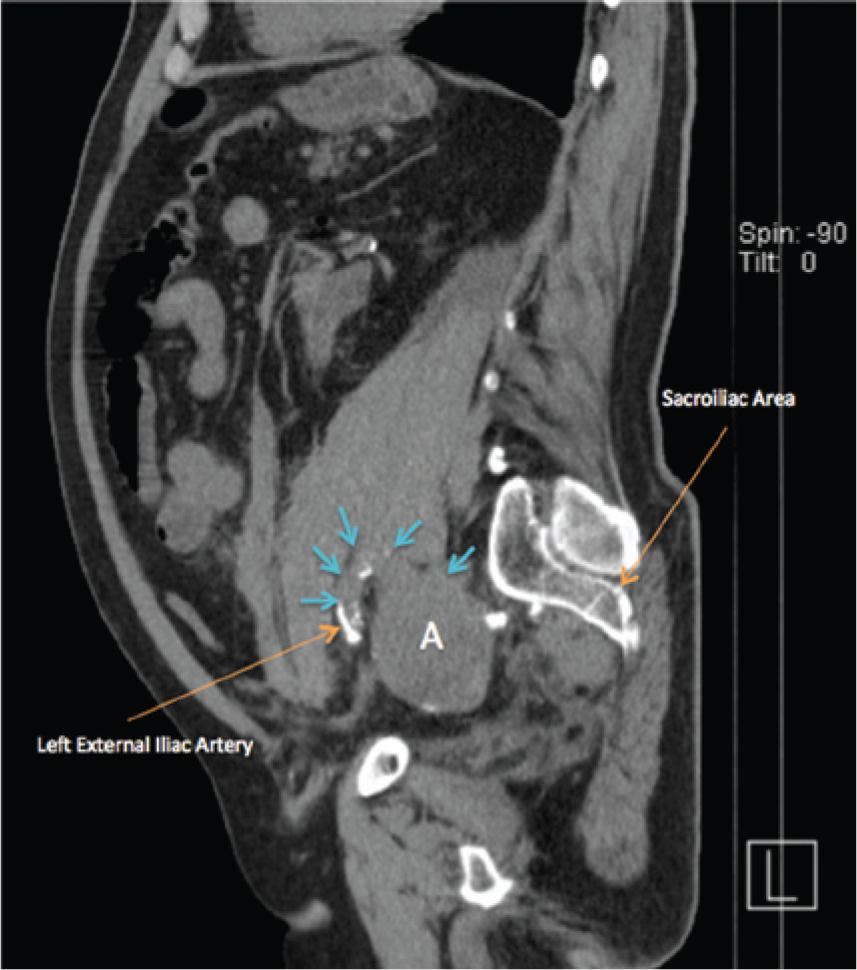
Sagittal noncontrast computed tomography reconstruction showing the external/internal iliac artery bifurcation (blue arrows) and the aneurysm (A).
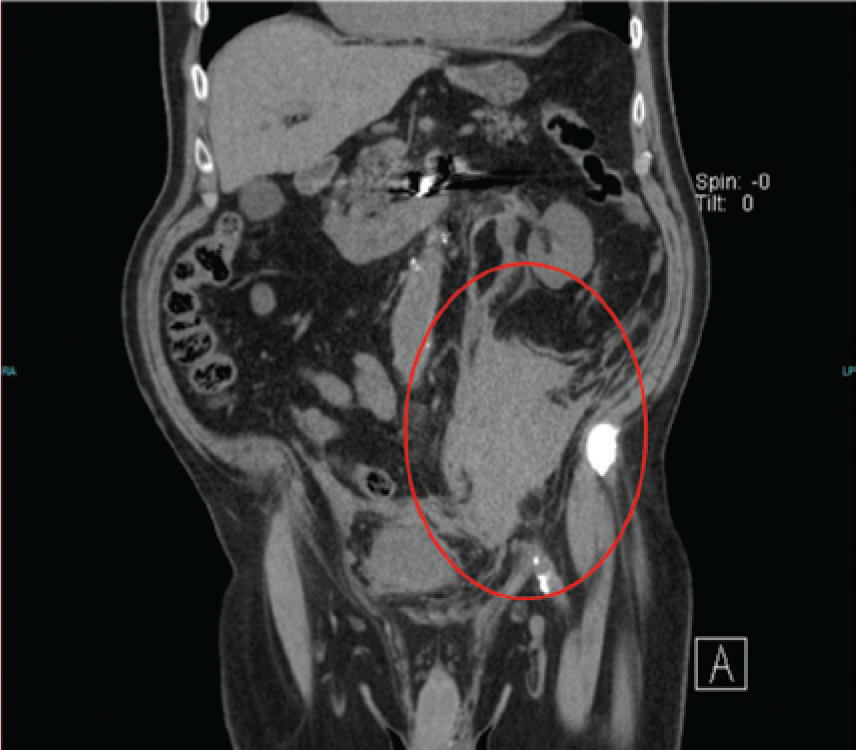
Coronal noncontrast computed tomography reconstruction showing the retroperitoneal hematoma (red oval) secondary to rupture of the internal iliac artery aneurysm.
Discussion
An artery is considered aneurysmal when its size is 50% larger than (or 1.5 times) the normal native artery diameter. Iliac artery aneurysms are found in about 25% of patients with an abdominal aortic aneurysm (AAA); however, the overall prevalence of iliac artery aneurysms in the adult population is just 1%, even when associated with AAA.1 -5 Internal iliac artery aneurysms make up about 20% of all iliac artery aneurysms and about 0.5% of all intra-abdominal aneurysms.1,3,4 The mean size at diagnosis is 7.7 cm, with aneurysms greater than 6 cm more likely to be symptomatic.3,6,7
Risk factors for internal iliac artery aneurysm are consistent with those commonly associated with peripheral vascular atherosclerotic disease. Strong associations are seen for male gender (with a ratio of six to one vs. females), white race, smoking, hypertension, advanced age (mean age 67.2 years), and prior AAA repair. 7 Other less common non-atherosclerotic risk factors include: history of traumatic childbirth, high forceps delivery, Caesarean section, or hysterectomy; arterial dissection; and Marfan’s Syndrome or other connective tissue disorders. Because internal iliac artery aneurysms are uncommon and exist deeply within the pelvis, they are difficult to diagnose on physical examination and typically only become symptomatic when they rupture, begin to compress upon neighboring structures, expand, or form an arteriovenous fistula.2,3 The symptoms of internal iliac artery aneurysm vary widely and can be very nonspecific; they have been reported to include urological and neurological symptoms, constipation, leg edema, and cellulitis.2,7
Sonography has been suggested as useful for asymptomatic diagnosis of an iliac artery aneurysm, although operator variability, bowel gas, and abdominal girth can make imaging of these vessels a diagnostic challenge.2,3,7 The precise location of the aneurysm (external vs. internal vs. common iliac arteries) can be difficult to define with sonography (as was the case with this patient). Computed tomography angiography (CTA) is the preferred diagnostic modality for acutely symptomatic patients, subject to its normal limitations of relatively large doses of radiation and intravenous contrast (which was contraindicated in this patient due to abnormal renal function tests). Magnetic resonance (MR) imaging and MR angiography can be used as well, but is limited by expense, availability, and extensive contraindications in the presence of medically complicated patients (e.g., those with metal implants and the risk of gadolinium-related kidney disorders). Arteriography can be used to confirm an iliac artery aneurysm, but its invasive nature and inability to truly define the diameter of an aneurysm limits this modality’s usefulness with iliac artery aneurysms. 8 Ultrasound technology has improved considerably since an early study in 1989 that showed that sonographic examination failed to detect 76% of iliac artery aneurysms when compared to angiography and computed tomography; however, the limitations noted previously remain. 7
When an iliac aneurysm is more than 3 to 3.5 cm in diameter, intervention is recommended and includes the following options: retroperitoneal-approached resection and reconstruction, intraoperative proximal ligation, proximal coil occlusion, and endovascular graft placement.7,9,10
The risk of rupture from an internal iliac artery aneurysm is approximately 33% (and up to 50%-60% in some reports), 11 with mortality from emergent repair estimated to be between 33% and 50%.7,12 Mortality from elective repair is typically much lower, but may still be as high as 7% to 11%.2,3,12 When an iliac artery aneurysm ruptures, it most often ruptures into the retroperitoneum, though rupture into the bladder (causing hematuria), peritoneum, colon, or iliac veins (creating an arterio-venous fistula) have also been reported. 10 Rupture of an internal iliac artery aneurysm has a high mortality rate, estimated anywhere between 50% and 100%.3,13 The prognosis for a patient with acute rupture in an emergent setting is grim overall, and it is even less encouraging for an anticoagulated patient such as the patient in this case study.
Conclusion
Internal iliac artery aneurysms are uncommon, and they are often found only when they have become large with a high attendant risk for rupture and significant resulting mortality. Early detection of these aneurysms is important for appropriate management. Sonography is the screening modality of choice in asymptomatic patients with multiple risk factors. The relatively high incidence of coexisting iliac artery aneurysms with abdominal aortic aneurysms makes sonographic investigation of the iliac artery system essential in the assessment and treatment of high-risk patients. This case demonstrates the appearance of an internal iliac artery aneurysm in a patient difficult to evaluate on physical examination because of large body habitus with acute rupture. The case illustrates how early detection and correlation with CT can aid the diagnosis of iliac artery aneurysm in such an acutely symptomatic patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.