
Abstract
Hypoxic-ischemic encephalopathy (HIE) is a major cause of brain damage and neurodevelopmental abnormalities in full-term newborn infants. We are reporting the results of a study comparing cranial magnetic resonance imaging (MRI) and cranial sonography (US) in 150 neonates with suspected HIE. Magnetic resonance imaging findings were normal in 44 patients (29%); 18% of patients showed only basal ganglia (BG) brightness, 10.6% showed brightness of the BG with intracerebral hemorrhage, and 63% of patients showed additional diagnostic details. Cranial US was normal in 75 patients (50%) and showed increased periventricular echogenicity in 32%, intraventricular hemorrhage in 9%, and additional diagnostic details in 13%. There was a positive correlation between MRI studies and US (P = .013). These data suggest that US is a worthwhile modality for the diagnosis of HIE but that early MRI findings will provide additional information in many cases in the detection of cerebral intraventricular hemorrhage.
Introduction
Neonatal hypoxic-ischemic encephalopathy (HIE) is one of the most common causes of cerebral palsy and other severe neurologic deficits in children, particularly in the newborn. Although the exact pathophysiology of HIE is not completely understood, the lack of sufficient cerebral blood flow in conjunction with decreased oxygen content in the blood leads to loss of normal cerebral autoregulation and diffuse brain injury. The exact nature of the injury depends on the severity of hypotension/hypoxemia and the degree of brain maturation. Hypoxic-ischemic encephalopathy occurs in 6 per 1000 live term births. Up to 40% of infants with moderate HIE and 100% with severe HIE either die or develop significant neurological impairments. 1 Neuroimaging modalities that are used for the identification and characterization of the severity, extent, and location of brain injury include ultrasonography (US), computed tomography (CT), and magnetic resonance (MR) imaging. Newer diagnostic technique refinements such as diffusion-weighted MR imaging and MR spectroscopy provide further insight into HIE and the potential for possible therapeutic intervention. 1 Detection, especially in the early phases of neurological deficit in newborns with HIE, is helpful in the management of HIE and in the prevention or minimization of complications. The objective of this study was to compare US findings with MR findings in the same neonates with suspected HIE to determine the efficacy of sonography in the early diagnosis.
Materials and Methods
The study was conducted at King Abdul Aziz Specialist Hospital, Taif, Saudi Arabia, during the period February 2010 to February 2012. All neonates with suspected HIE were potential candidates for the study, with a total of 150 infants enrolled (91 males and 59 females); participants were selected by a simple random convenience sampling. All participants were scanned using a 1.5 Tesla MR imaging system (Magnetom Symphony, Siemens Medical Systems, Erlangen, Germany) with a head coil. A neonatal head coil was not available for this study so an adult head coil was used with the standard imaging protocol modified to increase the repetition time for T1- and T2-weighted images from 400 to 800 msec. Real-time sonographic imaging was done using a 7.5 MHz linear array transducer (Sonoline G50, Siemens Medical Systems, Erlangen, Germany). Cranial sonographic scanning and cranial MR imaging with T1- and T2-weighted images, fluid attenuated inversion recovery imaging (FLAIR), Diffusion Weighted Imaging (DWI), and Apparent Diffusion Coefficient (ADC) studies were performed. All patients were closely monitored during their studies using electrocardiogram (ECG) and pulse-oximetry as well as tracking of temperature, blood pressure, respiration, and standard laboratory testing.
Statistical analysis was done using chi-square testing for MR imaging and US findings versus patient gender, and the Kendall rank correlation (Kendall’s tau-b statistic, which adjusts for equal values) and Spearman rank correlation, rho (Pearson correlation coefficient), to compare MR imaging with US findings.
Results
Figures 1 through 3 show representative comparative MR and US images, demonstrating the features of basal ganglia brightness, increased periventricular echogenicity, and hemorrhage. Table 1 summarizes the magnetic resonance imaging (MRI) findings. Cranial MRI showed normal results in 44 patients (29%). Basal ganglia (BG) brightness alone was seen in 27 patients (18%), 12 patients (8%) had BG brightness with associated intraventricular hemorrhage (IVH), and 4 patients (2.6%) demonstrated BG brightness with either intracranial hemorrhage (ICH) or periventricular hemorrhage (PVH). Forty-eight neonates (32%) showed other associated findings besides BG brightness, and 15 patients (10%) did not demonstrate BG brightness but had other neurodevelopmental changes.
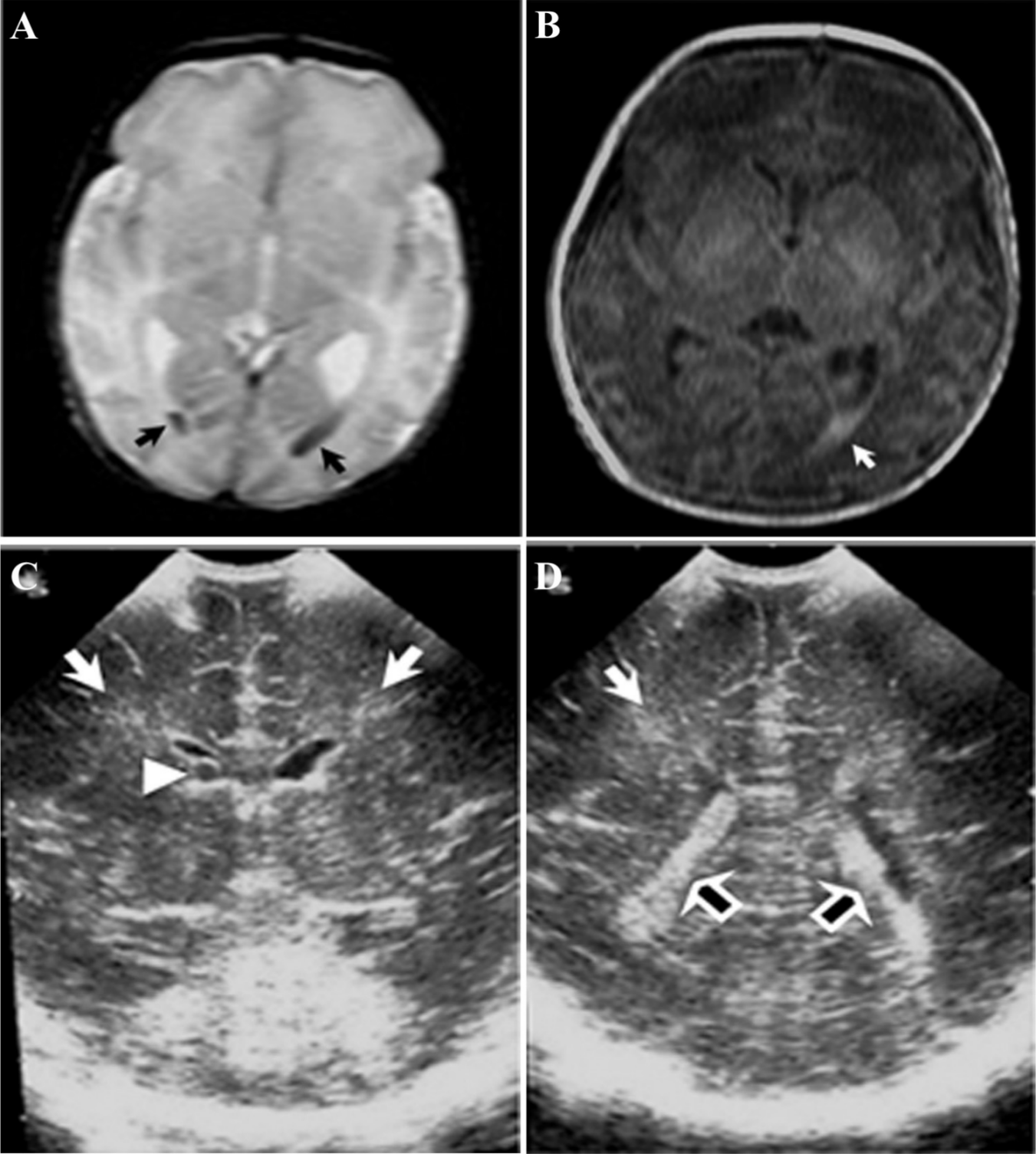
Comparative cranial magnetic resonance imaging (MRI) and ultrasonography (US) for the same neonate. (A) T2-weighted MRI image showing intraventricular hemorrhage (IVH) within both lateral ventricles (arrows). (B) T1-weighted MRI image showing bright basal ganglia and IVH in the left lateral ventricle (arrow). (C) Coronal sonographic image through the frontal horns and bodies of the lateral ventricles showing bilateral IVH (arrows) and a right subperiventricular small cyst (arrow head). (D) Coronal sonographic image through the frontal horns and bodies of the lateral ventricles showing IVH on the right (white arrow) and increased periventricular echogenicity bilaterally (open arrows).
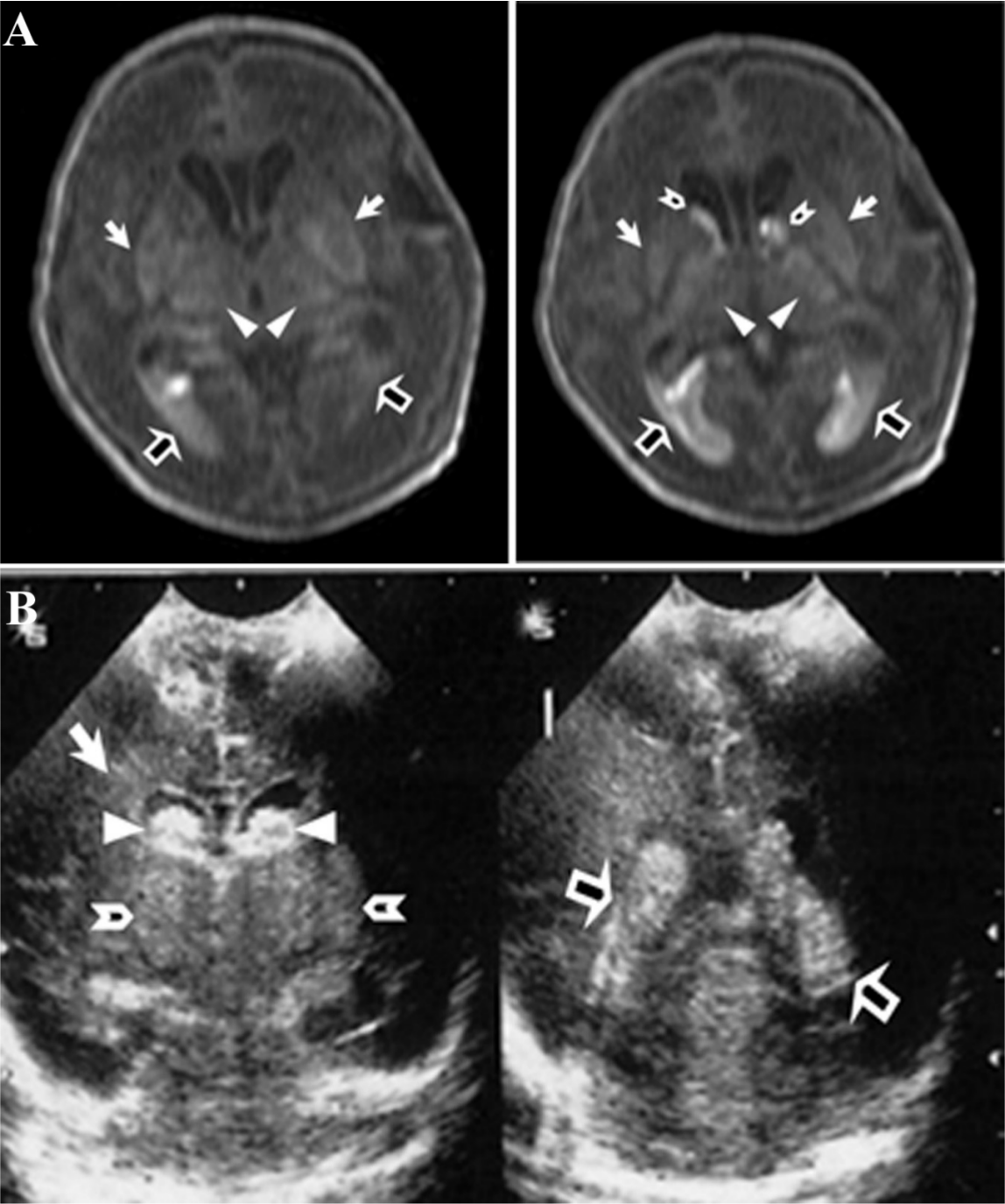
Comparative cranial magnetic resonance imaging (MRI) and ultrasonography (US) for the same neonae. (A) Cranial MRI, T1WI showing smooth brain surface, bright basal ganglia (arrows) and thalami (arrow heads), germinal matrix haemorrhage (open arrow heads), and IVH within both lateral ventricles (open arrows). (B) Cranial US showing increased periventricular echogenicity (arrow), increased basal ganglia echogenicity (open arrow heads) with germinal matrix haemorrhage (arrow heads), and IVH (open arrows).
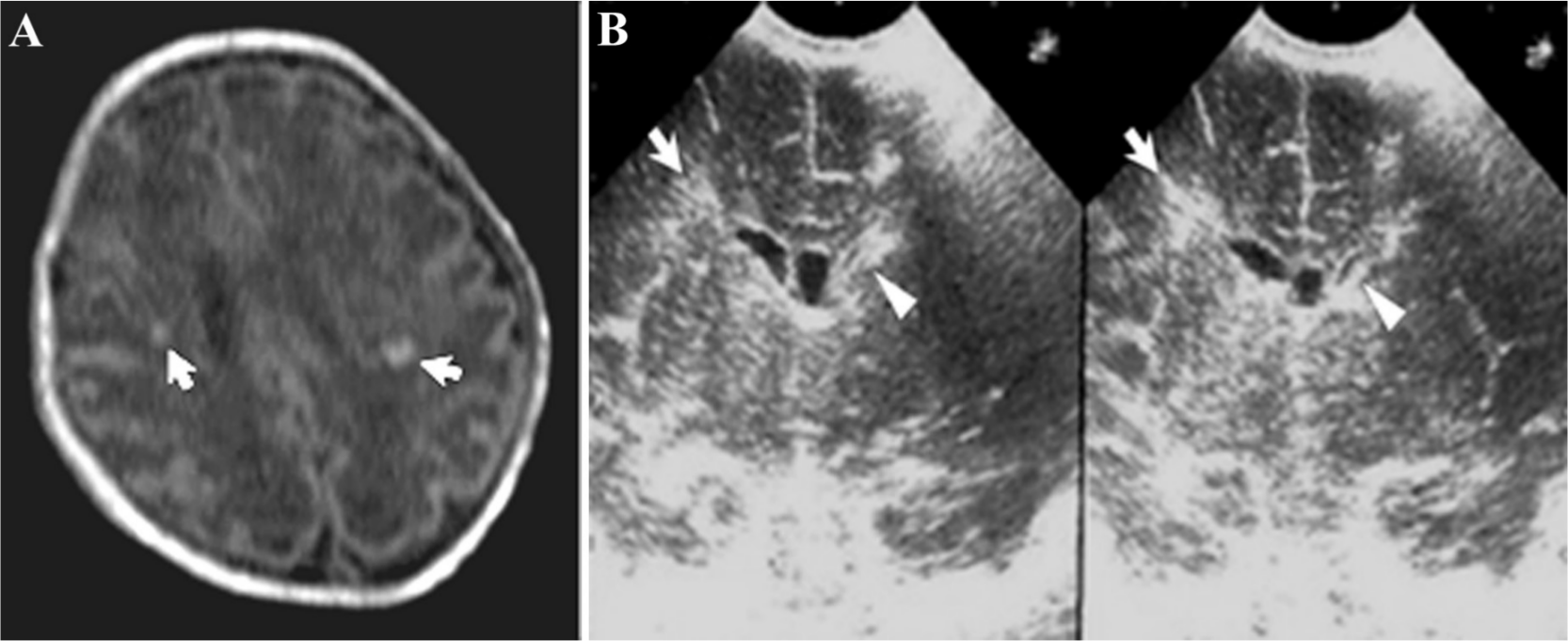
Comparative cranial magnetic resonance imaging (MRI) and ultrasonography (US) for the same neonae. (A) Cranial MRI, T1WI showing smooth brain surface, asymmetrical lateral ventricles with multiple periventricular, and subcortical white matter abnormal bright foci (arrows). (B) Cranial US showing asymmetrical lateral ventricles with attenuated left one (arrow heads) and increased periventricular echogenicity (arrows).
Magnetic Resonance Imaging (MRI) Findings.
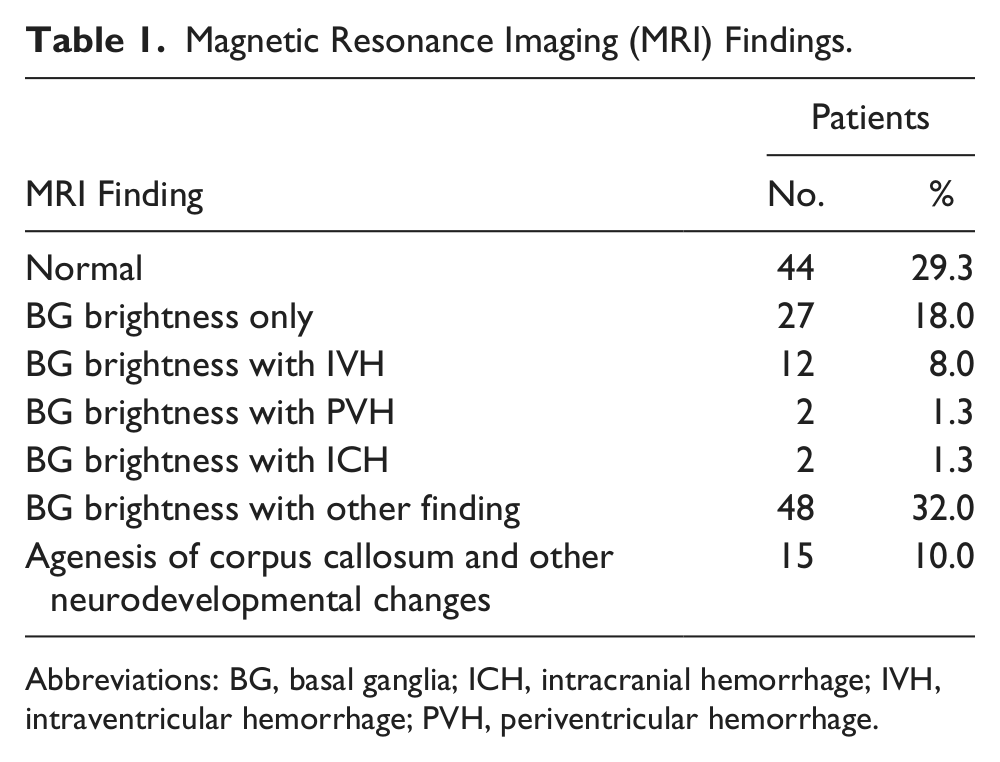
Abbreviations: BG, basal ganglia; ICH, intracranial hemorrhage; IVH, intraventricular hemorrhage; PVH, periventricular hemorrhage.
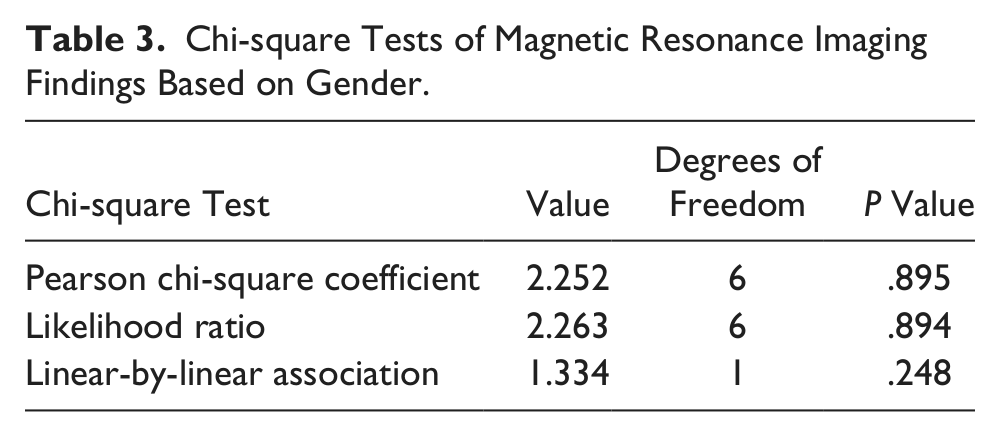
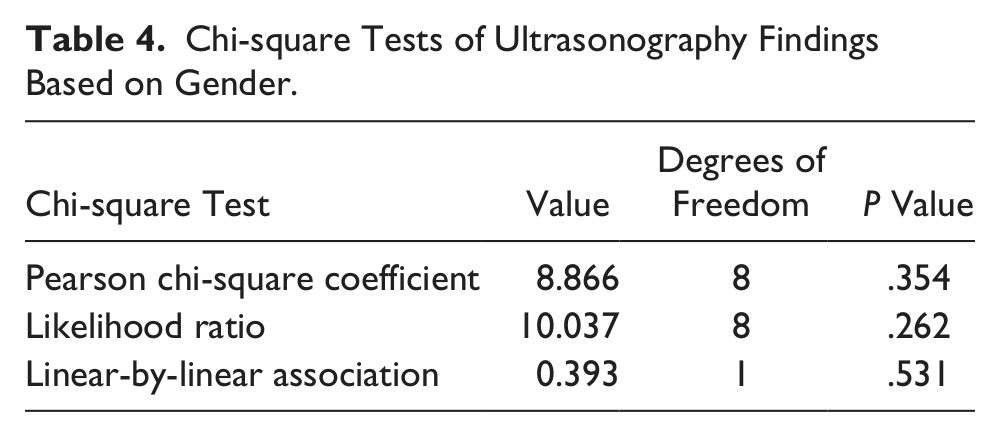
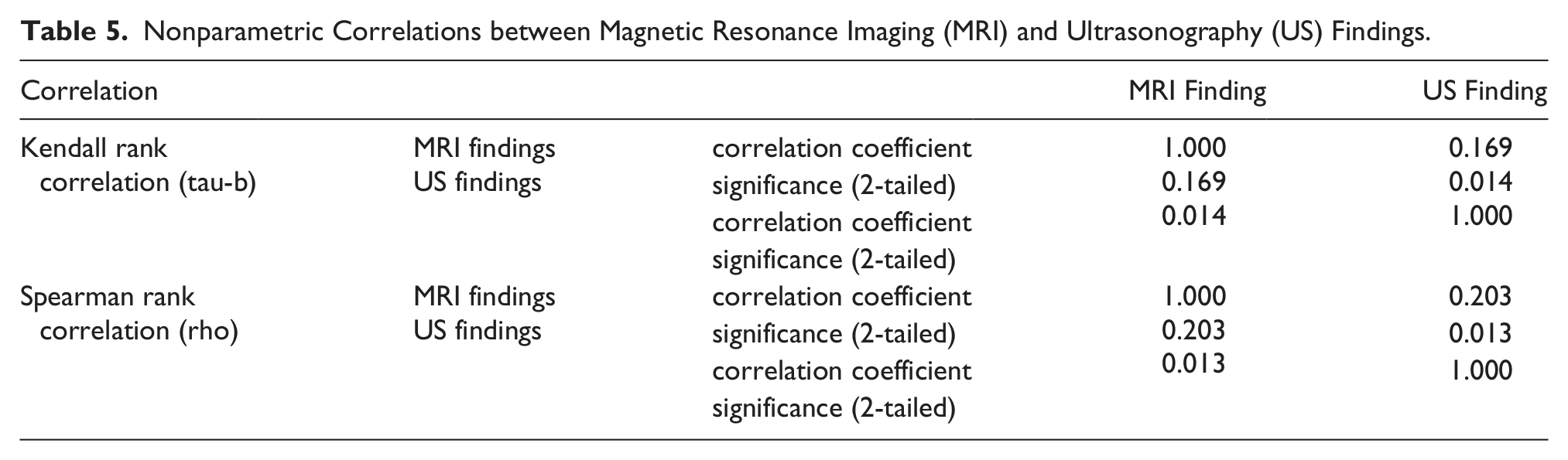
Table 2 summarizes the sonographic findings. Seventy-five neonates (50%) had normal cranial sonography, 48 patients (32%) had increased periventricular echogenicity alone, 14 patients (9%) had increased periventricular echogenicity with IVH, 10 patients (6.7%) had periventricular echogenicity with other associated findings, and 3 patients (2%) were noted to have cerebral/subarachnoid hemorrhage. Chi-square testing showed that there was no statistically significant relationship between patient gender and the findings for either MRI (Table 3; P = .895) or US (Table 4; P = .354). Nonparametric statistical analysis indicated a positive correlation between the MRI and US findings (Table 5; rho = 0.169, P = .013).
Ultrasonographic (US) Findings.
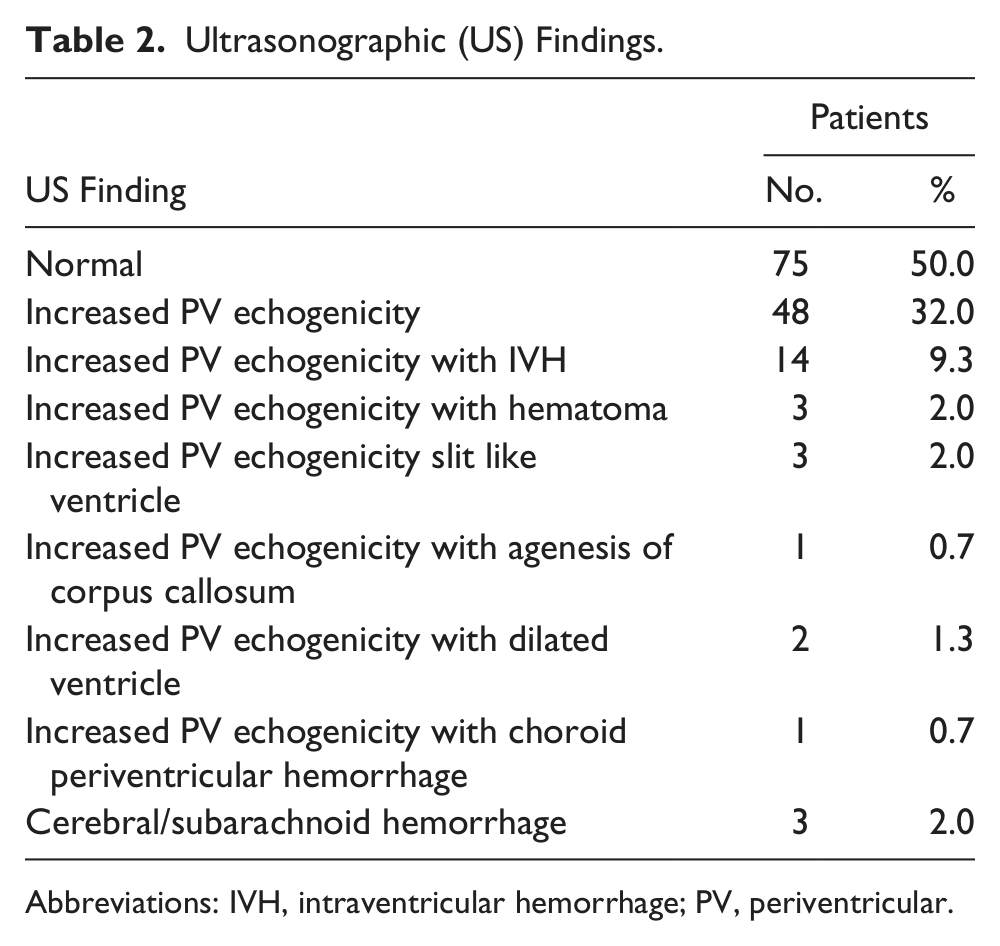
Abbreviations: IVH, intraventricular hemorrhage; PV, periventricular.
Chi-square Tests of Magnetic Resonance Imaging Findings Based on Gender.
Chi-square Tests of Ultrasonography Findings Based on Gender.
Nonparametric Correlations between Magnetic Resonance Imaging (MRI) and Ultrasonography (US) Findings.
Discussion
Hypoxic-ischemic encephalopathy is the most important cause of neurological morbidity and mortality in preterm and full-term neonates. Diagnosis and detection of early phase neurological deficits in babies with HIE is the most important step to determine the appropriate supportive treatment methods. Following initial resuscitation and stabilization, treatment of HIE is largely supportive and should focus on adequate ventilation and perfusion, careful fluid management, avoidance of hypoglycemia or hyperglycemia, and treatment of seizures.2,3 Interventional strategies are focused on avoiding any further brain injury in these infants. 4
The results of this study demonstrated the sensitivity and specificity of cranial MRI and US in diagnosing HIE. Among the 150 neonates, MRI studies detected brightness of the BG in 18%, brightness of the BG with IVH in 8.0%, ICH and PVH in 2.6%, and further details regarding diagnosis with implications for management (choroid plexus hemorrhage, agenesis of corpus callosum, epidural hematoma, cystic changes, and ventricular changes) in 63%. Cranial ultrasound detected increased periventricular echogenicity in 32% and IVH in 9% and showed further details in 13% of patients. There was a significantly positive correlation between the MRI and US findings (rho = 0.169, P = .013) as seen in Table 5. However, as shown in Tables 1 and 2, MRI was more sensitive in detecting abnormalities, consistent with other published series.5-7 There were 44 patients (29.3% of 150) with normal MRI findings while 75 patients (50%) had normal US findings. Additionally, the range of MRI findings was wider than the US findings.
Evidence of BG injury and ICH occurred with the highest frequency among MRI findings. These findings are compatible with a study by Liauw et al 8 that showed that the most frequent early MRI finding in HIE neonates is BG brightness in T1-weighted images, either as a solitary finding or in combination with other findings. Sie et al 7 showed that early MRI studies also were more sensitive than US studies in the detection of hemorrhagic lesions. In this study of 50 patients with increased periventricular echogenicity by US, early MRI provided no additional diagnostic information in 32% of patients. In the remainder of the patients, MRI allowed better differentiation of lesions at an earlier stage than sonography. There was very strong correlation between the early MRI results and the final sonographic diagnosis, but lesser correlation between the early results of both tests. They concluded that sonography remains a valuable modality for evaluation, but when inhomogeneous echogenicities are noted, early MRI will provide important information on the presence and extent of HIE.
Previous authors have suggested a gender bias for HIE, indicating a higher risk for male infants. 9 That is in contrast to the results of this study, summarized in Tables 3 and 4, which showed no statistical relationship between gender and HIE findings for either MRI or US evaluation.
A potential limitation of the present study is the use of an adult head coil for MRI examinations. Because the field of view is small, the possibility of a poor signal-to-noise ratio exists, which could limit sensitivity to increased echogenicity in the cerebral structures of interest. To counter this and gain the optimum possible resolution, the MR protocol followed increased the repetition time from 400 msec to 800 msec. This value was selected based on the results of Shroff et al, 10 who showed that the standard MR sequences used in adults must be adapted for use in neonates; the neonatal brain has longer T1 and T2 relaxation times because of its higher water content and lower protein and lipid contents.
Conclusion
This study suggests that sonography, a widely available and noninvasive technique, can provide valuable diagnostic information in cases of intracranial ventricular hemorrhage and is helpful in diagnosing HIE. The data further indicate, consistent with previous reports in the literature, that early MRI will provide additional information in many cases and that it is likely to remain the standard of care for imaging for HIE in the neonate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.