
Abstract
Sialolithiasis is a rare condition characterized by the presence of stones within the salivary gland or duct. Salivary duct stones have an incidence of 1% at autopsy, but only 50 in 1,000,000 present symptomatically per year. Possible signs and symptoms include an upper neck or jaw mass that enlarges and recedes following meals and xerostomia, or dry mouth. Sonography has been used along with a number of other imaging modalities to diagnose this condition. The use of real-time sonographic imaging allows for identification and confirmation of the presence of stones within the salivary gland. Treatment of sialolithiasis generally begins conservatively but can result in surgery if not resolved. This case report demonstrates the use of sonography as an effective method of diagnosing sialolithiasis in a patient with classic symptoms.
The presence of calculi within the human body is not uncommon, but the presence of calculi within the salivary glands is. Sialolithiasis is the presence of calculi, or stones, in the salivary glands or ducts. This condition has a 1% incidence at autopsy, but only about 50 in every 1,000,000 per year present symptomatically. 1 Possible signs and symptoms of sialolithiasis include an upper neck or jaw mass that enlarges and recedes following meals and xerostomia, or dry mouth. 2
Although sonography is commonly used to diagnose the presence of stones in other areas of the body, the salivary glands are not commonly imaged using sonography. However, calcific stones can be visualized more easily and less invasively with sonography than with other imaging modalities. The following case report demonstrates the usefulness of sonography in diagnosing sialolithiasis.
Case Report
A woman in her late 60s presented in the emergency department with a mass at the base of her left jaw. The patient reported a rapid onset of swelling that evening but remarked that it was not painful. She also noted that she had experienced slight xerostomia (dry mouth) on the left side of her mouth. After palpation of the mass for any sign of calcification, the patient was taken for a computed tomography (CT) scan.
The CT was ordered with and without contrast, but because of the patient’s allergy to iodine, the CT was performed only without contrast. A marker was placed in the left submandibular region, and the CT showed no obvious evidence of fluid collection, although the metallic marker somewhat obscured several images. Without the use of contrast, an abscess could not be ruled out. No tracheal effacement was evident, and all remaining soft tissue and bony structures were unremarkable. A large density consistent with calcification was noted near the base of the left jaw (Figure 1). Sonography was suggested for further evaluation of the mass.
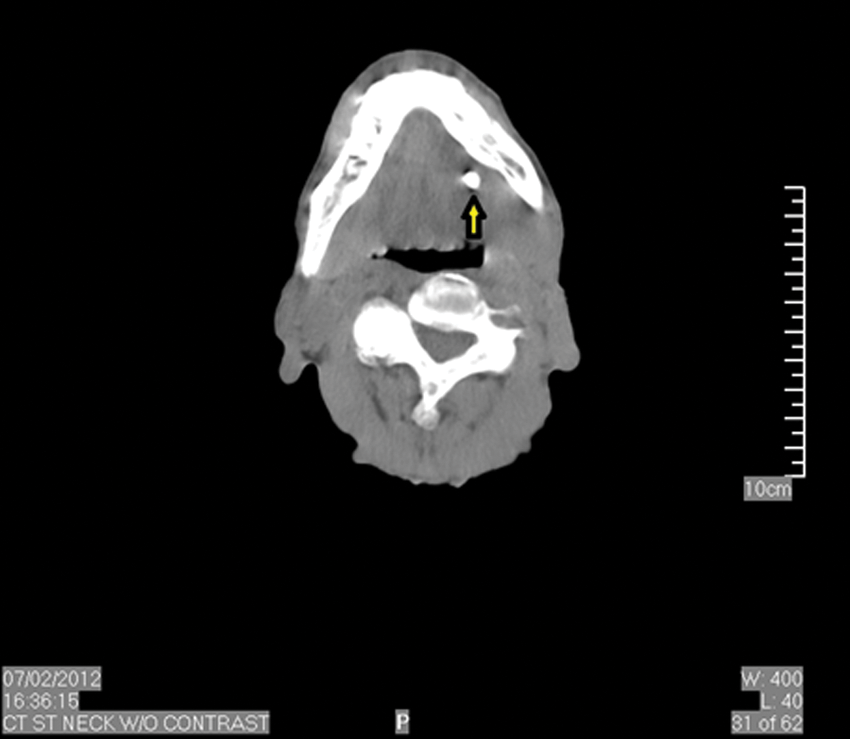
Computed tomography (CT) without contrast demonstrating large echogenic focus at the base of the left jaw (arrow).
Sonography was performed on the soft tissues of the neck below the left mandible using an Acuson Sequoia C512 system (Siemens Medical Solutions, Malvern, Pennsylvania) with a linear-array 14-MHz transducer. The mass was thoroughly examined in the long and transverse planes (Figures 2 and 3), including Doppler assessment of blood flow to the area (Figure 4). A heterogeneous well-circumscribed mass was visualized. The mass measured 3.8 × 3 × 1.8 cm, and diffuse, normal blood flow was demonstrated within and around the area. Cystic structures lacking the presence of flow were visualized throughout the mass (Figure 5). An area of possible calcification was noted, with posterior acoustic shadowing present (Figures 5 and 6). These traits were indicative of a salivary duct stone. The soft tissue mass was characteristic of submandibular salivary gland tissue. The patient was referred to an ear, nose, and throat (ENT) specialist for further evaluation.
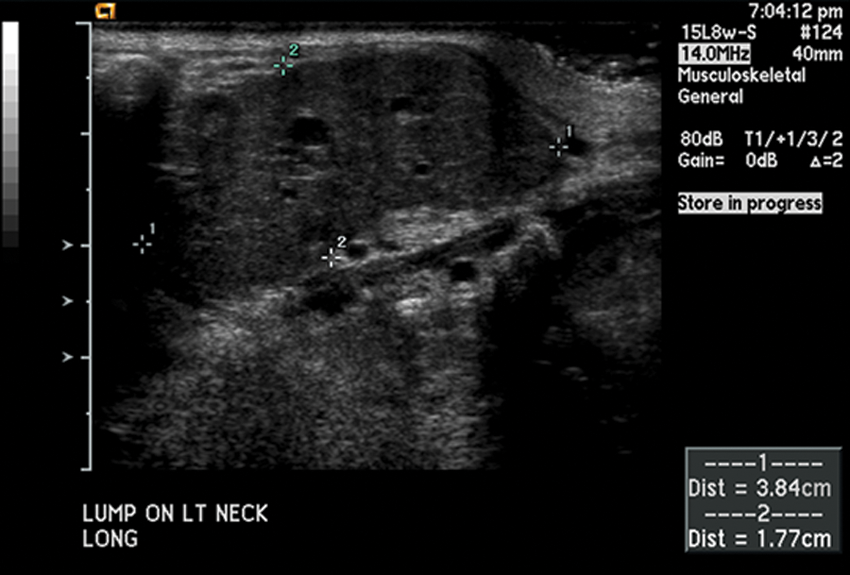
Longitudinal view of neck mass measuring 3.84 cm in length and 1.77 cm in height.
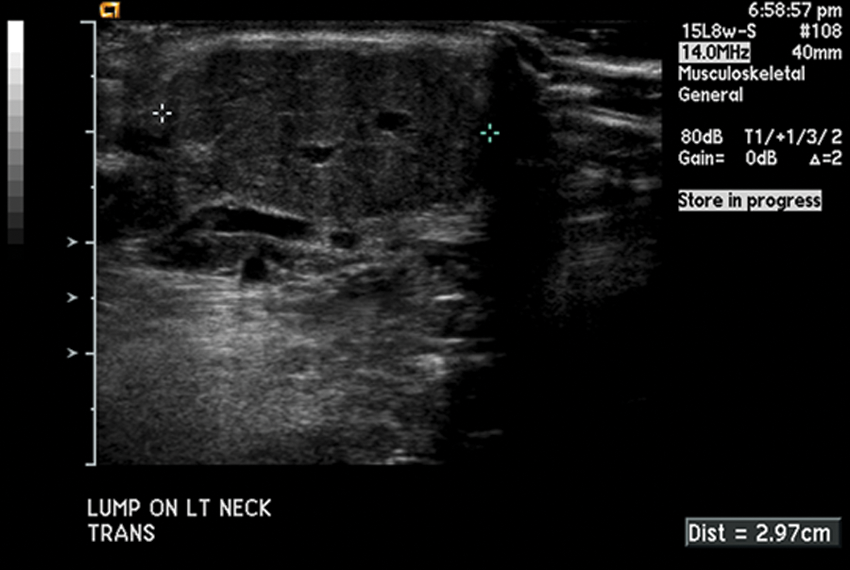
Transverse view of neck mass, measuring 2.97 cm in width.
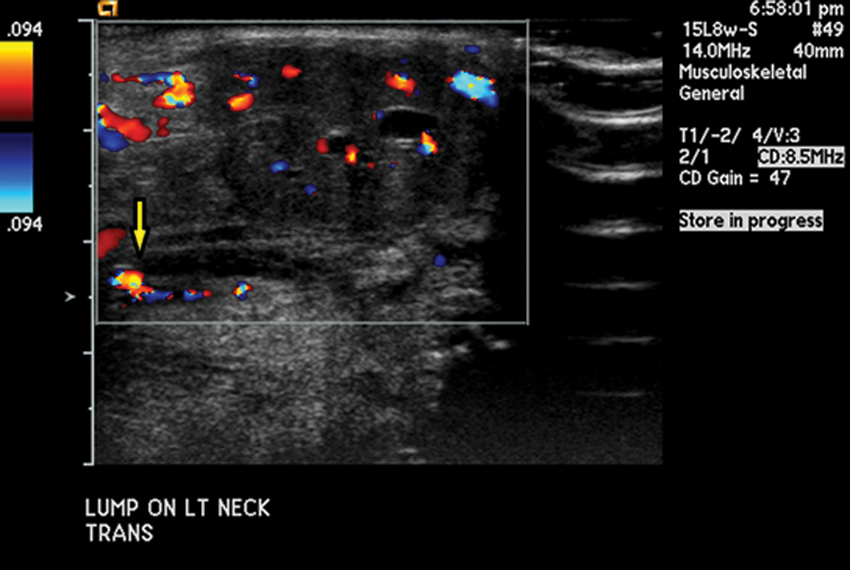
Transverse view of neck mass demonstrating diffuse, normal blood flow. Cystic structures (arrow) are demonstrated throughout the mass.
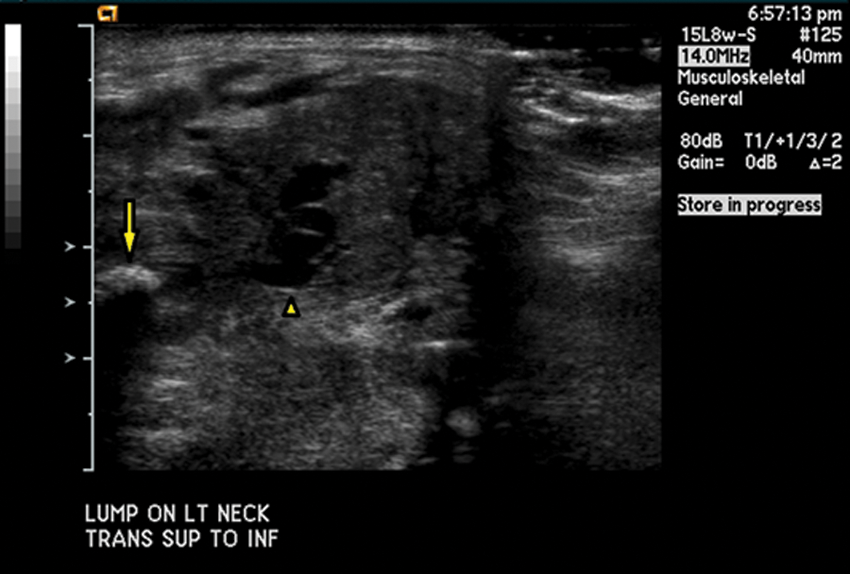
Transverse view demonstrating area of calcification (arrow) with acoustic shadowing. Cystic area (arrowhead) demonstrated directly lateral to calcification.
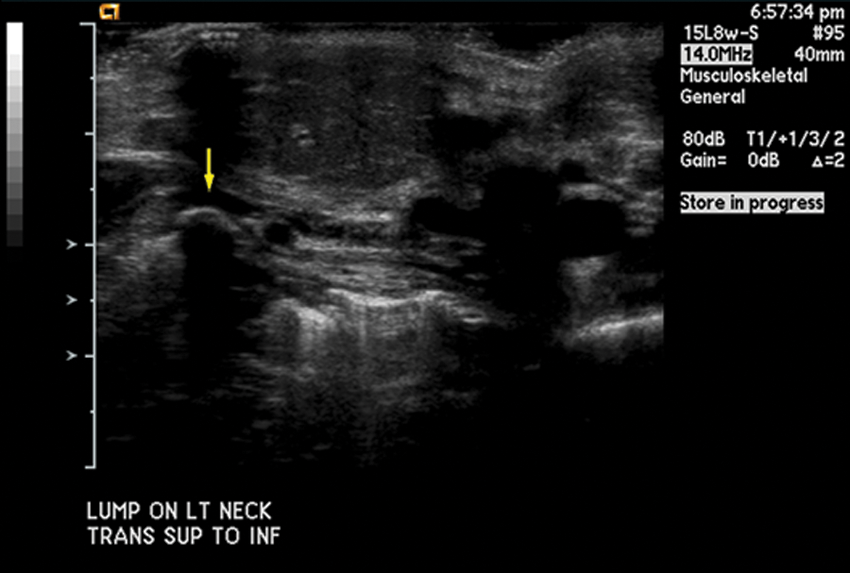
Transverse view demonstrating area of calcification (arrow) with acoustic shadowing.
The ENT specialist saw the patient as an inpatient in the hospital. He determined that there were stones present in the gland and diagnosed her with sialolithiasis. He noted that due to the stones, the swelling of the gland would continue to increase and decrease. He determined that no further treatment was necessary at this time. The patient was directed to stay well hydrated and suck on sugar-free lemon drops to keep the saliva moving. If the patient noted a large increase in swelling again, she was directed to return to his office for further evaluation and treatment.
Discussion
There are three types of salivary glands located around the mouth: the parotid glands, the submandibular glands, and the sublingual glands. The salivary glands are responsible for producing saliva and delivering it to the mouth when stimulated. Saliva is carried to the mouth through a system of ducts. The main ducts are the Stensen duct, which drains the parotid gland, and the Wharton duct, which drains the submandibular gland and part of the sublingual gland. 1 The Stensen duct is longer and narrower than the Wharton duct; however, saliva is able to flow with gravity into the oral cavity.
Calculi are formed due to a relative stagnation of calcium-rich saliva in a setting of partial obstruction. 1 Stones are largely composed of calcium phosphate and calcium carbonate as well as other salts and organic material such as glycoproteins, desquamated cellular residue, and mucopolysaccharides. 2 The submandibular gland is the most common site for calculi, with an incidence rate of 80% to 92%. 3 Reasons for this high occurrence are due largely to the duct itself. The Wharton duct is large and long, and salivary flow is slow and against gravity. Saliva in this duct also tends to be more alkaline, with a high mucin and calcium content. 3 Other factors that may increase the incidence of stones are the presence of dehydration, use of anticholinergic medications such as Effexor, and trauma-induced predisposition to stones. 1 Patients who experience chronic sialadenitis, or inflammation of the salivary gland, are also at a greater risk of developing calculi. Common causes of sialadenitis include postoperative dehydration, radiation therapy, and immunosuppression such as diabetes mellitus, organ transplant, chemotherapy, and human immunodeficiency virus (HIV). 2 The patient in this case was later noted to be under treatment for cancer and currently on hospice care, which contributed to her increased risk for developing sialolithiasis.
Formation of stones in the salivary glands is more common in men than in women, and it is rare in children. The majority of patients are between 30 and 60 years of age, and 75% present with single stones. Submandibular stones tend to be larger and intraductal, whereas parotid stones are usually smaller and multiple. 2 Differential diagnoses associated with sialolithiasis include sialadenitis, both viral and bacterial; radiation sialadenitis; lymphoepithelial cysts secondary to HIV; Sjögren syndrome; malnutrition; and tumors.3,4 Sjögren syndrome is an immune system disorder characterized by dry mouth and eyes. In a study performed by Shimizu et al, 5 three cases of patients with Sjögren syndrome were examined with sonography. The purpose of the examination was to evaluate the damage in the glands due to chronic xerostomia. In all three patients, microliths were found in the parenchyma of the parotid gland, most of which did not demonstrate typical characteristics of calculi such as comet tail artifact or posterior shadowing. In all three cases, an additional imaging modality was used and confirmed the presence of stones in the parenchyma of the parotid gland.
Although CT, magnetic resonance (MR) imaging, and x-ray can be used to diagnose sialolithiasis, the most effective diagnostic imaging modality is sonography. Ultrasound is noninvasive, fast, and widely available, making it a first choice when assessing for sialolithiasis. Although results are operator dependent, sonography can detect up to 90% of salivary duct stones, despite that approximately 20% to 40% of salivary duct stones are not opaque on plain films. 1 A study conducted by Jager et al 6 examined the possibility of MR sialography, which uses evoked salivation as a contrast as opposed to an invasive contrast substance, as an alternative imaging method. Because of its noninvasive approach, MR sialography was considered superior to CT or digital radiographic sialography. The authors concluded that the use of MR sialography in delineating the submandibular ductal system and detecting stones was similar in accuracy to digital sialography and superior to sonography due to increased specificity and sensitivity, but with added expense. On the basis of these results, MR sialography would have been a possible alternative imaging modality in this case to further confirm the presence of calculi in the salivary ducts.
Treatment of sialolithiasis usually begins conservatively with a number of measures, depending on the cause of the stones. Initial treatments include hydration, warm compresses, and massage of the gland. It is often recommended that the patient use a sialagogue, such as sugar-free lemon drops, to continue salivary gland stimulation and keep saliva moving. 3 If the calculi are caused by an anticholinergic medication, it is recommended that the patient discontinue use of the medication. Nonsteroidal anti-inflammatory drugs (NSAIDs) are recommended for pain, and antibiotics may be prescribed if infection is suspected. Stones that are less than 2 mm in diameter often pass spontaneously and do not require surgery. 2
If a conservative approach is not effective, a more aggressive treatment may be pursued transorally. If a stone is near the opening of the Wharton duct, the duct may be cannulated, dilated, and the stone removed. Stones that are deeper may require surgical excision of the duct or the entire gland. Extracorporeal shock wave lithotripsy may also be used on intraductal stones that are less than 7 mm and easily located by sonography. Finally, wire basket extraction under fluoroscopic guidance may be used for stones that are extraglandular and mobile. 2
Conclusion
Sialolithiasis is a rare salivary gland disorder characterized by the presence of calculi within the salivary gland or duct. Although it is possible to diagnose this condition using a number of imaging modalities, the most cost-effective mode is sonography, detecting up to 90% of salivary duct stones. Although treatment can become extensive and lead to surgery, most stones can be treated simply with hydration, warm compresses, massage, and the use of sialagogues.
This case demonstrated the use of two imaging modalities to identify and diagnose sialolithiasis: sonography and CT. Sonography was shown to be an effective way of confirming a diagnosis of stones in the salivary gland. A conservative method of treatment was used to treat the patient; however, if symptoms worsen, ductal cannulation may be considered.
Footnotes
Acknowledgements
The author thanks Brent A. Amos, Dr Jeffery Jennings, and Dr Michael Shaw for their help in gathering data for this case study.
Declaration of Conflicting Interest
The author declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author received no financial support for the research and/or authorship of this article.