
Abstract
The sonographic features of extrarenal manifestations of complicated acute pyelonephritis (APN) have rarely been reported. A case of severe APN in a young woman is presented with the imaging workup done exclusively by conventional sonography using color and power Doppler. Discussion places a focus on the imaging spectrum and clinical significance of the extrarenal manifestations. The hepatobiliary findings of APN appear to signify accompanying sepsis and gravity of the condition, and gallbladder wall thickening must not be misdiagnosed as acute cholecystitis.
Although the renal imaging findings of acute pyelonephritis (APN) have been repeatedly presented in the literature, the extrarenal manifestations of complicated APN have rarely been reported,1,2 especially those related to the sonographic diagnosis. 3 A case of severe APN with extrarenal imaging findings in a young woman is presented, with the imaging workup exclusively based on sonography findings, focusing on the imaging spectrum and clinical significance of the extrarenal manifestations.
Case Report
A 20-year-old woman presented to the emergency department with a 24-hour history of intense right-sided abdominal pain. Six days earlier, she had developed a febrile urinary tract infection, refusing hospitalization and following an empirical antibiotic treatment. Physical examination on presentation to the emergency department showed a thin, acutely ill-looking woman with diffuse abdominal tenderness. An intense nonproductive cough was also present with no auscultatory findings. Her vital signs were as follows: temperature, 40°C; blood pressure, 80/60 mm Hg; pulse rate, 105 bpm; and respiratory rate, 25 per minute with oxygen saturation of 99%. Chest radiograph revealed blunting of the right costophrenic angle. The patient was admitted to the hospital directly from the emergency department.
On the day of admission, abdominal sonography was done using a Philips iU22 system with a C5-1 curved linear array transducer (Philips Healthcare, Andover, Massachusetts). Sonography showed an enlarged right kidney enlarged with a pole-to-pole length of 14.7 cm. More than the upper half of the organ was noted to have an increased echogenicity, with a bulging contour and loss of corticomedullary differentiation (Figure 1a). Color Doppler showed the relevant area to have a diminished and fragmented vascularity (Figure 1b). The right renal pelvis had a thickened urothelium that measured 4 mm. The left kidney was similarly enlarged with a pole-to-pole length of 13.6 cm and noted to have a slightly heterogeneous echotexture. Freely moving particles were seen in the dependent portion of the urinary bladder, raising the possibility of pyuria. The gallbladder wall thickness measured 1.3 cm with a reticular appearance (Figure 2). The periportal area was shown to be hyperechoic (Figure 3). This finding, also known as a periportal halo sign, measured 5 mm. In addition, increased width and hyperechogenicity of the right anterior extrarenal tissue as well as a small fluid effusion at the right anterior pararenal space were evident (Figure 4). Right pleural, perihepatic, and perisplenic fluid collections were also noted (Figures 3 and 5).
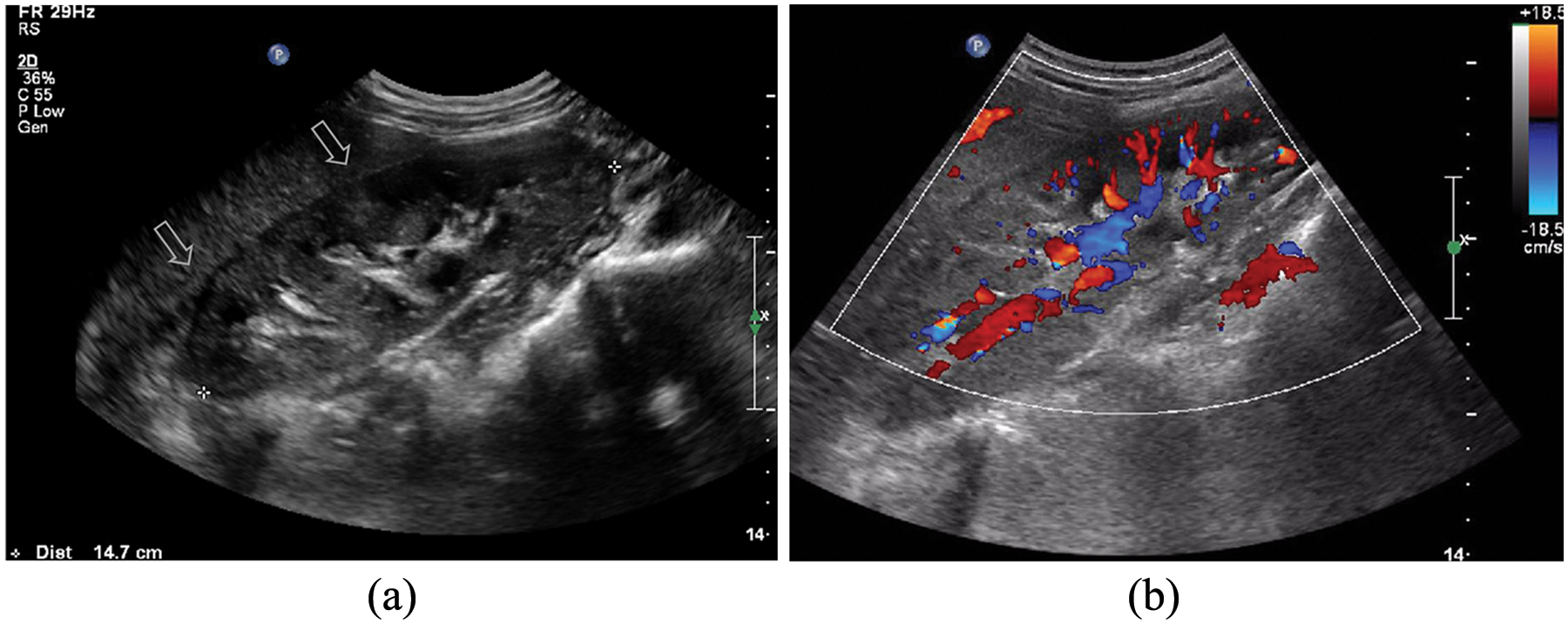
Longitudinal sonographic images of the right kidney obtained at admission. (a) An enlarged kidney with a bulging contour and increased parenchymal echogenicity in its upper half as well as loss of corticomedullary differentiation is depicted (arrows). (b) On color Doppler, decreased vascularity and color signal fragmentation in the relevant area are shown.
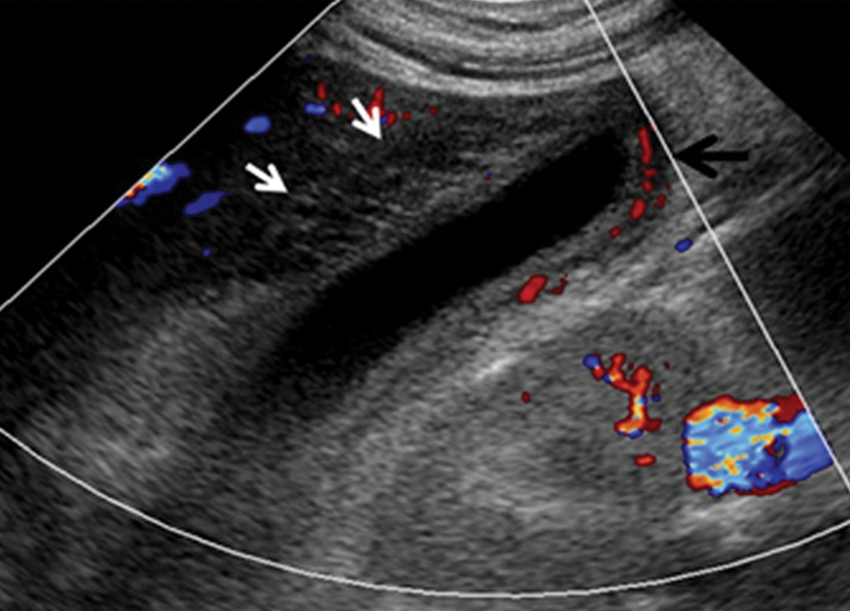
Longitudinal color Doppler sonographic image of the gallbladder. The gallbladder wall is markedly thickened with a reticular pattern (white arrows). Wall hyperemia is evident by the clear depiction of the cystic artery (black arrow).
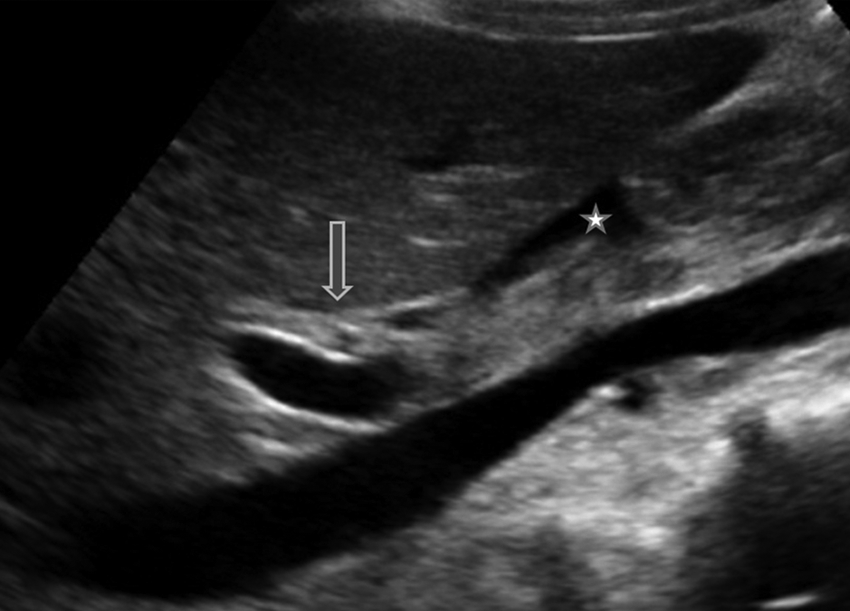
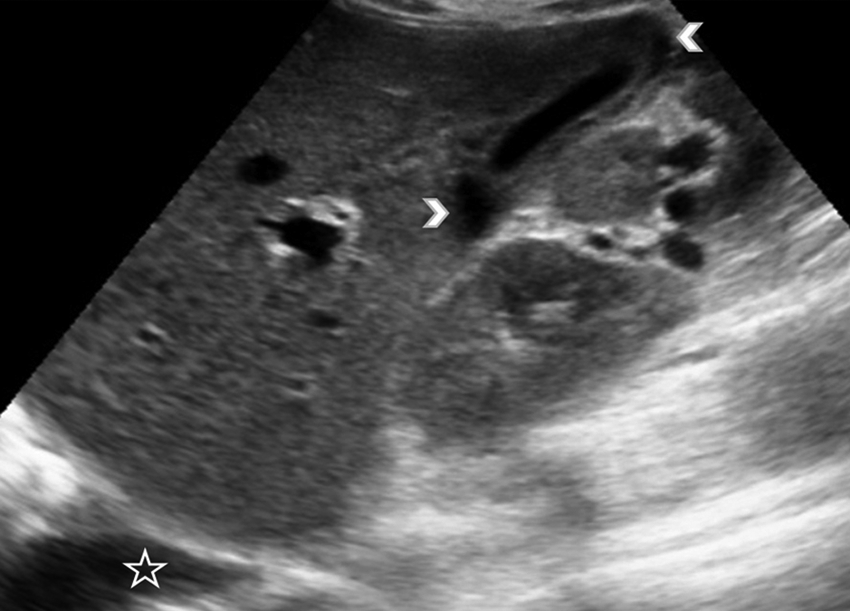
Oblique sonographic image at the level of the porta hepatis. The periportal area is thick and hyperechoic (arrow). A small subhepatic fluid collection is also seen (*).
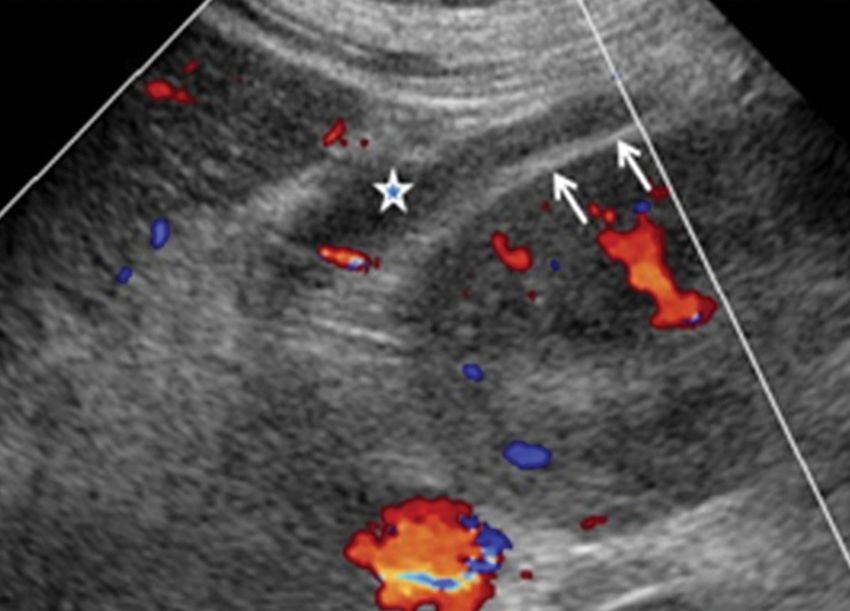
Oblique sonographic image at the level of the anterior pararenal space. Increased width and hyperechogenicity of the right anterior extrarenal tissue is shown (arrows) with a small amount of fluid effusion within (*).
Oblique sonographic image at the level of the right hepatic lobe. Small pericholocystic (arrowheads) and pleuritic (*) fluid collections are recognized.
Laboratory tests showed elevated values for white blood cell (WBC) count of 22,900/mm3; (normal values, 3800–10,500/mm3;); C-reactive protein, 29.62 mg/dL (normal values, <0.5 mg/dL); erythrocyte sedimentation rate, 63 mm (normal values, 0–20 mm); alanine aminotransferase, 43 U/L (normal values, 10–40 U/L); aspartate aminotransferase, 41 U/L (normal values, 10–40 U/L); gamma-glutamyl transferase, 53 U/L (normal values, 0–30 U/L); international normalized ratio, 1.3 (normal values, 0.9–1.2); and fibrinogen, 584.9 mg/dL (normal values, 200–380 mg/dL). Diminished laboratory values were seen for hematocrit, 28.8% (normal values, 36.8%–45.6%); serum creatinine, 0.55 mg/dL (normal values, 0.7–1.3 mg%); serum potassium, 2.8 mmol/L (normal values, 3.5–5.1 mmol/L); and serum albumin, 2.3 g/dL (normal values, 3.5–5.5 g/dL). Laboratory values were within normal limits for platelet count, 168,000/µL (normal values, 150,000–400,000/µL); serum urea, 28 mg/dL (normal values, 8–50 mg/dL); alkaline phosphatase, 78 U/L (normal values, 40–150 U/L); and serum sodium, 136 mmol/L (normal values, 136–145 mmol/L). The urine was noted to be cloudy, and urinalysis showed marked pyuria (80–100 WBC per high-powered field). In combination, the findings of inflammation with abnormal liver and renal function tests presented a clinical picture consistent with complicated acute pyelonephritis and sepsis.
The patient was treated with ceftriaxone (2 g/d) and became afebrile on the fourth day of hospitalization. The urine culture yielded Escherichia coli >100,000 colony-forming units/mL. Repeated sonography on the seventh day of hospitalization showed diminished swelling of the kidneys compared with the previous sonogram with a normal echotexture, as well as a normal gallbladder appearance. Both the pleural and peritoneal fluids had been absorbed. The patient was discharged on the eighth day of hospitalization with complete recovery.
Discussion
Urinary tract infection (UTI) most commonly occurs in young women. Acute pyelonephritis is the most serious form of UTI, which affects the renal parenchyma, interstice, and pelvis. In approximately 35% of patients, when host defenses are compromised, APN gives rise to complications such as renal corticomedullary or perirenal abscess, papillary necrosis, or emphysematous pyelonephritis, and it is then characterized as a complicated case of APN. 4 Without proper treatment, the renal pelvis and parenchyma can be damaged, and following sepsis, this may be fatal. 5
Previously reported imaging findings of the extrarenal manifestations of complicated APN are ascites, pleural effusion, gallbladder wall thickening, and hepatic periportal tracking. Two different explanations have been suggested for the pathogenesis. These have been attributed to either direct extension of the adjacent inflammation 3 and/or increased vascular permeability and sodium reabsorption with or without hypoalbuminemia related to sepsis. 2
Gallbladder wall thickening is a nonspecific finding that may also be seen in various noncholecystic pathologic conditions such as congestive heart failure, renal failure, hepatitis, cirrhosis, ascites, and hypoalbuminemia.6–8 On sonography, the presence of striations (also known as a reticular pattern) in the clinical setting of acute cholecystitis serves as an alert of gangrenous changes in the gallbladder. Conversely, in cases of inflammation close or distal to the gallbladder, the above-mentioned sonographic sign is a further confirmation of the inflammatory severity and spread, as well as the resultant sepsis. 4
Hepatic periportal tracking is a sign predominantly seen on computed tomography but has also been described in sonography.2,9 It reflects altered hepatic lymphatic dynamics and may also be seen in cirrhosis, hepatitis, primary or metastatic liver neoplasms, biliary obstruction, liver transplant recipients, right-sided cardiac failure, bone marrow transplant recipients, severe preeclampsia, and pediatric blunt abdominal trauma. As an extrarenal imaging finding in APN, hepatic periportal tracking indicates a more serious clinical course of the disease. 10
In the case presented, the patient was a young woman who was admitted with the clinical picture of complicated APN with sepsis. After a careful and meticulous abdominal sonogram, outside the consequential parenchymal changes of both kidneys and the perirenal findings on the right side (as a consequence of extension of inflammatory process), there was no evidence of obstructive abnormalities, renal abscess, papillary necrosis, or emphysematous pyelonephritis. The thickened urothelium of the right renal pelvis and the floating debris within the urine bladder (although not specific findings) supported the sonographic diagnosis. 11 The positive gallbladder wall thickening sign, as well as the fluid accumulation into the third space, was indicative of the incipient sepsis on the day of admission, and both disappeared after successful therapy. The hepatic periportal tracking sign was negative from the onset (not greater than 5 mm), 9 and this finding predisposed the patient to a less severe clinical condition.
Conclusion
The extrarenal manifestations of complicated acute pyelonephritis can be adequately identified with sonography and used to signify accompanying sepsis and the gravity of the present illness. Furthermore, the hepatobiliary findings should not be confused with other medical conditions causing a similar imaging picture, especially when there is no clinical suspicion of acute pyelonephritis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.