
Abstract
The objective of this study was to investigate whether gallbladder wall thickening in cirrhotic patients adds risk to the formation of gallstones. In this retrospective study, 259 patients with cirrhosis resulting from hepatitis B or hepatitis C were included (152 men, 107 women; mean ± SD, age 48.8 ± 11.4 years [range, 29–77 years]) and compared with 300 healthy participants comprising the control group. All participants had a standard abdominal sonographic assessment. The prevalence of gallstones in cirrhotic patients with and without gallbladder wall thickening was studied, and the distribution of gallstones and gallbladder wall thickening in different Child-Pugh classes was compared. The prevalence of gallstones in cirrhotic patients, cirrhotic patients with and without gallbladder wall thickening, and healthy participants was 27.4%, 28.8%, 13.0%, and 5.3%, respectively. The prevalence of gallstones in cirrhotic patients with gallbladder wall thickening was not significantly higher than in those without gallbladder wall thickening (P > .05). Gallbladder wall thickening occurred with a higher frequency in Child-Pugh B and C patients, and normal thickness of the gallbladder wall was seen more frequently in Child-Pugh A patients (P < .05). Gallstones were found more frequently in Child-Pugh A and C patients (P < .05). In conclusion, gallbladder wall thickening in cirrhotic patients does not significantly add any risk for the formation of gallstones.
Liver cirrhosis caused by hepatitis B and hepatitis C is a common disease worldwide. Patients with cirrhosis have many changes in different tissues and organs, often with significant biliary system impairment. As a result, gallbladder wall thickening occurs, and a higher incidence of gallstones is seen.1–6 However, gallbladder wall thickening and gallstone formation do not take place in all cases. Although a study by Zhang et al 5 showed that gallbladder wall thickening is a risk factor for gallstone formation, no other confirming reports have been found, and more evidences is needed to determine the relationship, if any, between gallbladder wall thickening and gallstone formation. The purpose of this study was to investigate whether gallbladder wall thickening adds significant risk to the formation of gallstones.
Patients and Methods
A cross-sectional retrospective study on the incidence of gallstones in cirrhotic patients was conducted based on the clinical data in our hospital medical information system from January 2005 to September 2011. The hospital institutional review board approved the study and informed consent was waived.
Two hundred fifty-nine patients with liver cirrhosis resulting from hepatitis B or hepatitis C were enrolled (152 men, 107 women; mean ± SD age 48.8 ± 11.4 years [range, 29–77 years]). Patients excluded from the study included 19 patients with alcoholic cirrhosis, 3 patients with primary biliary cirrhosis, 3 patients with cryptogenic cirrhosis, and 26 patients with coexisting diabetes or hyperlipidemia or with a prior cholecystectomy. The control group was selected from participants undergoing a general health screening from July 2010 to September 2011, matched as closely as possible to the study group with respect to sex, age, and lifestyle. A total of 300 control participants were enrolled (177 men, 123 women; mean ± SD age 50.8 ± 11.8 years [range, 30–74 years]), with 14,868 potential control participants excluded. Exclusion from the control group was based on coexisting liver diseases, heart disease, nephropathy, diabetes, hyperlipidemia, prior cholecystectomy, and significant alcohol consumption (>20 g/d, average weekly consumption). All patients and control participants had a standard abdominal sonographic assessment. The establishment of the diagnosis of liver cirrhosis and Child-Pugh class was based on a combination of clinical history, laboratory tests, medical imaging studies, and biopsy. A thickness of the gallbladder wall less than 4 mm was considered normal, and a thickness equal to or greater than 4 mm was considered thickened.5,6 Scoring for classification into Child-Pugh categories was based on laboratory measures of total bilirubin, serum albumin, and the prothrombin time international normalized ratio, as well as the presence and severity of ascites and hepatic encepalopathy. 7 This system is widely used to determine the clinical severity of cirrhosis and can be used to gauge disease prognosis; two-year mortality ranges from 15% for class A to 65% for class C.
The sonographic examination was performed respectively by five experienced sonologists using a Logiq 9 (GE Healthcare, Waukesha, Wisconsin), Voluson Expert 730 (GE Healthcare, Piscataway, New Jersey), HD11XE (HP Medical Systems, Dalian, China), Sonos 5500 (HP Medical Systems, Eindhoven, Netherlands), or Siemens Sonoline Premier (Siemens Medical Systems, Shanghai, China) system. All examinations were done using a convex transducer with a frequency range of 2 to 5 MHz. The patients and control participants were instructed to fast overnight (12 hours) before their sonographic examination. The incidence of gallstones in the control group and in cirrhotic patients with and without gallbladder wall thickening was recorded, and the proportion of gallstones and gallbladder wall thickening in different Child-Pugh classes was compared.
Statistical analysis was done using SPSS software (version 11.5; SPSS, Inc, an IBM Company, Chicago, Illinois). Continuous data were expressed as mean ± standard deviation (SD). Variables of different groups were compared using the χ2 test for noncontinuous variables and independent samples t test for continuous variables, respectively. A P value of <.05 was considered statistically significant.
Results
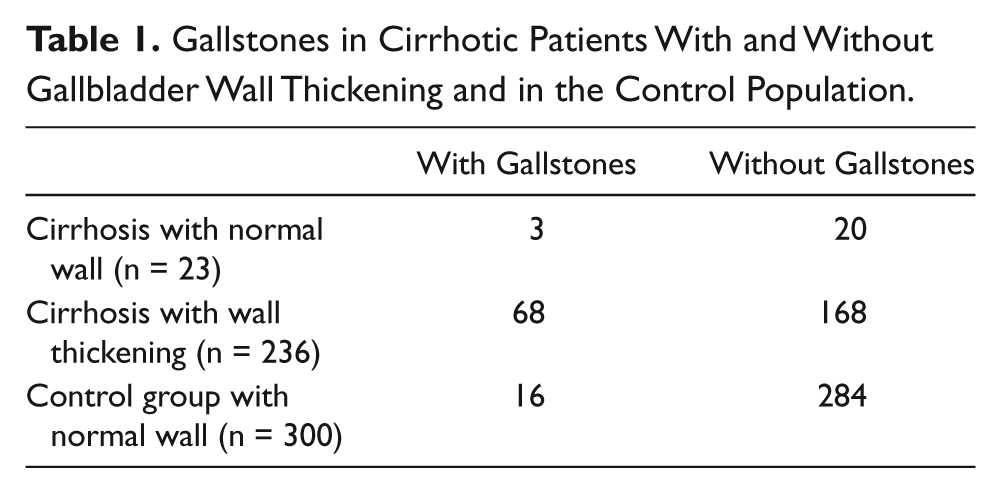
The incidence of gallstones in cirrhotic patients, cirrhotic patients with and without gallbladder wall thickening, and control group participants was 27.4%, 28.8%, 13.0%, and 5.3%, respectively. Table 1 shows that the incidence of gallstones between patients with gallbladder wall thickening (68 of 236, 28.8%) and the control group (16 of 300, 5.3%) was significantly different (P < .001). However, the prevalence of gallstones in cirrhotic patients with (28.8%) and without (13.0%) gallbladder wall thickening was not significantly different (P > .05). In addition, the prevalence of gallstones in cirrhotic patients without wall thickening (13.0%) and in the control group (5.3%) was not significantly different (P > .05).
Gallstones in Cirrhotic Patients With and Without Gallbladder Wall Thickening and in the Control Population
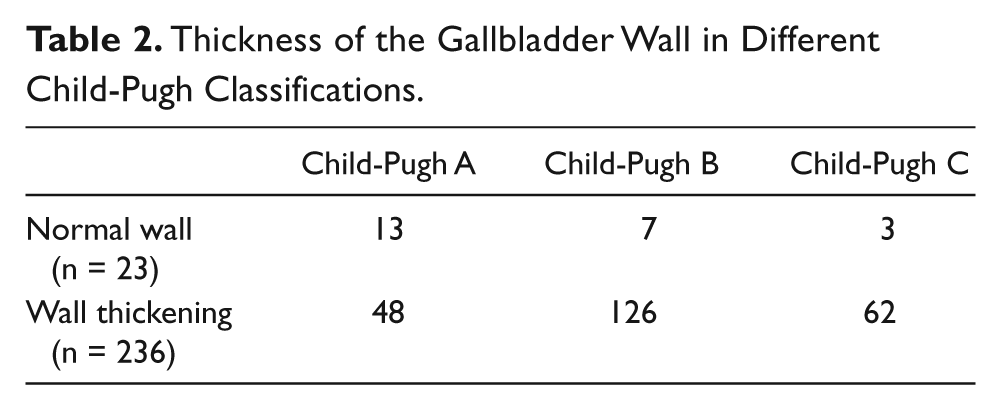
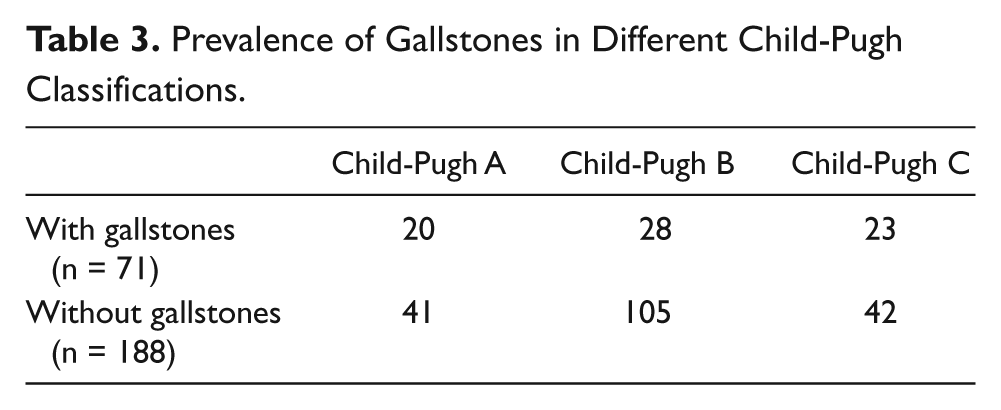
Tables 2 and 3 show the comparison of thickness of the gallbladder wall and gallstones in different Child-Pugh classes. Gallbladder wall thickening occurred predominantly in Child-Pugh classes B and C; normal thickness of the gallbladder wall was seen more frequently in Child-Pugh class A patients (P < .05). Gallstones were found with greater frequency in Child-Pugh class A and C patients (P < .05).
Thickness of the Gallbladder Wall in Different Child-Pugh Classifications
Prevalence of Gallstones in Different Child-Pugh Classifications
Discussion
It is well known that the prevalence of gallstones in cirrhotic patients is higher than in the general population.1–5 The prevalence of gallstones in cirrhotic patients with and without thickening of the gallbladder wall in this study was 28.8% and 13.0%, respectively, with no statistically significant difference between them. This is in contrast to the study by Zhang et al, 5 which showed that gallbladder wall thickening was a risk factor for the development of gallstones. The results of this study indicate that gallbladder wall thickening may not independently affect significantly the development of gallstones, and the factors that contribute to the thickening of the gallbladder wall may not be the same ones that contribute to the development of gallstones. This idea is supported by the study by Acalovschi et al, 8 who showed that the thickness of the gallbladder wall does not correlate with gallbladder emptying parameters that are associated with the development of gallstones. In this study, gallbladder wall thickening occurred predominantly in Child-Pugh class B and C patients, and normal thickness of the gallbladder wall was associated predominantly with Child-Pugh class A. These findings suggest that gallbladder wall thickening may be associated with the severity of the disease, and this is partially consistent with the study by Wang et al. 6 In addition, gallstones appeared more frequently in Child-Pugh class C patients than in class B patients, suggesting that the formation of gallstones may be associated with the progression of liver disease, consistent with a number of reports in the literature,2,5,9,10 although not with the study by Conte et al. 1 The proportion of gallbladder wall thickening in Child-Pugh class A versus B plus C had a very significant difference, indicating that gallbladder wall thickening primarily occurs toward the end stage of cirrhosis.
Once gallbladder wall thickening has occurred in Child-Pugh class A, it will remain throughout the remaining stages of the disease; certainly, gallbladder wall thickening may occur in Child-Pugh class B or C alone, consistent with the study by Wang et al. 6 This study shows that gallstones occur significantly more often in patients with cirrhosis than in the noncirrhotic population, although not all cirrhotic patients develop gallstones and/or gallbladder wall thickening. These findings correlate with other reports in the literature, suggesting that not only the elements contributing to the formation of gallstones in the general population play a role in cirrhotic patients, but other elements secondary to the cirrhosis, such as impaired gallbladder contractility and motility, may also significantly affect the development of gallstones.2–4,8–10
The potential limitations of this study include the fact that this was a retrospective cross-sectional study and no data were collected regarding longitudinal surveillance of any patients, and thus any dynamic information on changes of the gallbladder wall and gallstones is lacking.
In conclusion, the prevalence of gallstones in cirrhotic patients with gallbladder wall thickening and in cirrhotic patients with normal thickness of the gallbladder wall was not significantly different, suggesting that the gallbladder wall thickening commonly seen in cirrhotic patients does not independently increase the risk for the development of gallstones. Gallstones appear to develop predominantly either relatively early in the cirrhotic process (Child-Pugh class A) or much later in Child-Pugh class C patients, with a lower prevalence seen in Child-Pugh B patients.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Professors Rong Tu and Li Huang and to sonologist Ying Guan for their helpful advice and assistance in preparing this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.