
Abstract
Emphysematous pyelonephritis is a severe kidney infection that is common in women and patients with diabetes mellitus, but rare in cancer patients. A 64-year-old patient with advanced uterine cervical cancer developed emphysematous pyelonephritis after urine diversion by percutaneous nephrostomy of the left kidney, which is a possible approach to this infection. Antibiotic therapy was started to achieve clinical improvement and preserve renal function, and radical nephrectomy was not an option due to the functional exclusion of the contralateral kidney. The patient progressed with worsening renal function; thus, she started outpatient hemodialysis, with improvement of the uremic encephalopathy. She died 7.7 months after admission, 1 month after treatment for emphysematous pyelonephritis. Treatment should be adjusted to the patients’ needs, including maintenance of hemodialysis to improve symptoms. Further investigation is needed to identify possible causes and prevent emphysematous pyelonephritis in cancer patients.
Introduction
Emphysematous pyelonephritis is an acute and severe necrotizing infection of the renal parenchyma and perirenal tissues resulting in gas formation around the affected kidney1–4 with a mortality rate ranging from 11% to 42%. 5 Treatment requires fluid resuscitation, the use of antibiotics, and surgery. It remains controversial whether the initial approach should be radical nephrectomy or percutaneous drainage. 4 Two systematic reviews support drainage as the best initial approach, including percutaneous nephrostomy.6,7 However, there are reports of treatment with antibiotic therapy alone, without nephrectomy or drainage. 8
In the few cases describing emphysematous pyelonephritis in cancer patients, there is an association with diabetes mellitus or fistulas.9–12 This study aims to describe a case of emphysematous pyelonephritis following urinary diversion by percutaneous nephrostomy (a procedure also used to treat this infection) in a patient with cervical cancer without diabetes mellitus.
Case presentation
A 64-year-old patient was diagnosed with cervical squamous-cell carcinoma and presented with KDIGO 13 stage III post-renal acute kidney injury (serum creatinine described in Table 1) 2 weeks before admission to a cancer hospital. Hemodialysis was required until urinary diversion by bilateral percutaneous nephrostomy performed 8 days after admission, with improvement in renal function 4 days after the procedure. The cervical cancer clinical stage at that time was FIGO 14 IVA.
Laboratory test results (biochemistry, urine, and blood cultures) and antibiotics used to treat urinary tract infection after percutaneous nephrostomy.
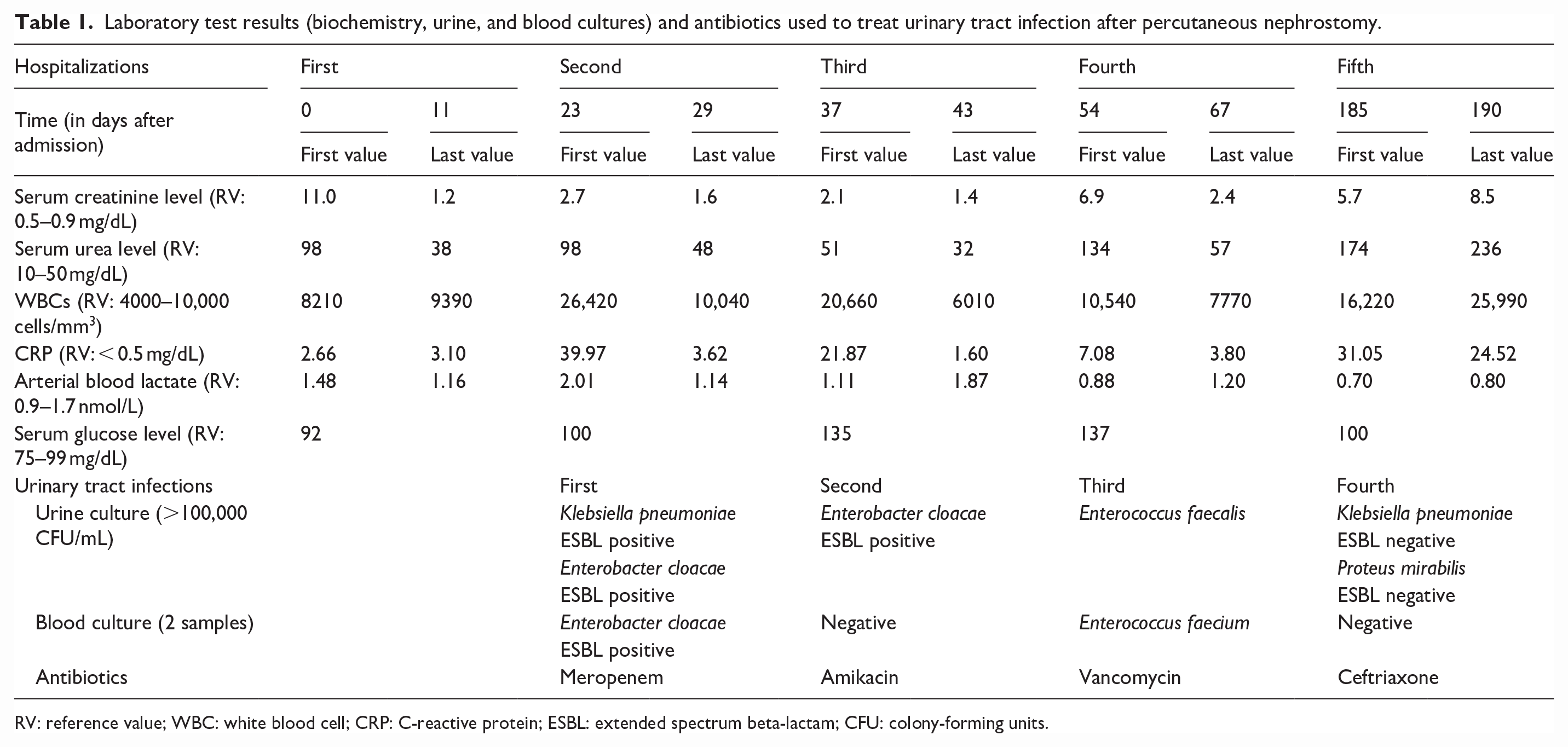
RV: reference value; WBC: white blood cell; CRP: C-reactive protein; ESBL: extended spectrum beta-lactam; CFU: colony-forming units.
The patient returned 23 days after resolution of acute kidney injury due to pyelonephritis. Antibiotic treatment was guided by urine and blood culture results (Table 1), with clinical and renal function improvement. Two weeks after the first pyelonephritis (37 days after admission), she had fever (38.8°C), leukocytosis, and further deterioration of renal function. After antibiotic therapy for the second pyelonephritis (Table 1), the patient underwent percutaneous nephrostomy catheter replacement with a double-J antegrade catheter in the left urinary collecting system (40 days after admission to the hospital). The bilateral percutaneous nephrostomy catheters were removed 3 days after double-J placement, and the absence of hydronephrosis was confirmed by ultrasound. Some improvement in renal function was observed at hospital discharge (Table 1).
On day 54, after admission, the patient was admitted to the hospital with fever (38.1°C), decreased diuresis, and elevated serum creatinine (Table 1). An ultrasound showed new bilateral dilatation of the collecting system, even with a well-placed double-J catheter in the left kidney. Cultures were obtained, antibiotic therapy was started, and bilateral percutaneous nephrostomies were performed. The right percutaneous nephrostomy catheter was removed after 3 days due to severely reduced urine output, secondary to progression of right-sided chronic kidney disease. The left renal double-J catheter was not removed due to the possibility of a vesical fistula.
With clinical improvement and no recurrence of urinary tract infections, a new tumor staging was performed. An imaging study on day 107 after admission confirmed an extensive fistulous tract, and the bladder largely infiltrated by the tumor lesion with some gas formation (Figure 1(a)). Onco-specific treatment was planned. This patient underwent carboplatin chemotherapy (5 cycles of 95 mg per dose, adjusted for renal impairment—AUC 2 multiplied by estimated creatinine clearance) in combination with external beam radiotherapy, total dose 4500 cGy in the fifth month after admission. BOOST was not indicated due to the presence of the tumor fistula. As a result, a slight reduction of the tumor and no change in the suspicious lymph nodes were observed. Post-treatment imaging showed no evidence of gas in the bladder (Figure 1(b)).

(a) Pelvis magnetic resonance image showing invasion of the neoplasm into the bladder (*), tumoral fistula (**), and presence of gas bubbles in the bladder (full arrow). (b) Pelvis magnetic resonance imaging showing an enlarged vesicotumoral fistula (***) and disappearance of gas in the bladder. (c) Computed tomography with coronal plane reconstruction showing the presence of air in the left renal pelvis (single arrow) already with percutaneous nephrostomy, confirming emphysematous pyelonephritis.
On day 160 after admission, there was improvement in urinary diuresis. The left nephrostomy catheter was removed after remaining occluded for 4 days, and imaging confirmed the absence of left urinary tract hydronephrosis. Seven days later, there was a spontaneous outflow from the double-J catheter placed in the left kidney through the bladder, with no left hydronephrosis 24 h after the event.
Ten days later (day 177 after admission), renal function deteriorated, requiring a final percutaneous nephrostomy. One week later, serum creatinine remained elevated with gross hematuria in the percutaneous nephrostomy, fever (39°C), and leukocytosis (Table 1).
When there was no improvement in renal function after urine diversion by percutaneous nephrostomy, a glomerulopathy secondary to a paraneoplastic syndrome was hypothesized. However, on day 185 after admission, computed tomography showed a well-placed percutaneous nephrostomy catheter, with the resolution of the hydronephrosis. Nonetheless, it showed gaseous foci interspersed in the calices and left renal pelvis, no gas in the bladder (Figure 1(c)), an increase in the vesicotumor fistula, and cancer progression with lung metastasis.
The patient remained hemodynamically stable, cultures were obtained, and antibiotic therapy was started (Table 1) for the treatment of emphysematous pyelonephritis, with the intention of trying to control this infection and thereby improve renal function. In addition, it would be possible to study the continuation onco-specific treatment. However, the patient’s renal function deteriorated, and radical nephrectomy was not feasible due to the progression of the cancer and the functional exclusion of the right kidney. Thus, the patient was referred to palliative care with hyperactive delirium due to uremic encephalopathy. The prognosis was a few weeks, and the delirium did not improve with the drug treatment.
On day 205 after admission, the patient started outpatient hemodialysis, with an improvement of the uremic encephalopathy, and on day 219 after admission, the left percutaneous nephrostomy catheter was removed because it had no output. The patient died on day 232 of admission, 1 month after treatment for emphysematous pyelonephritis.
Discussion
This case describes a rare and severe infection, rarely observed in cancer patients, following renal pelvic drainage for urinary diversion, a procedure also indicated for the treatment of emphysematous pyelonephritis. The correct diagnostic approach is necessary to provide the best available treatment, especially in patients with advanced cancer. In the case of emphysematous pyelonephritis, the diagnosis is made by radiologic studies.
In 1898, Kelly and MacCallum described cases of pneumaturia in three groups: when air is mechanically introduced through the bladder; when gas is produced in the urinary tract by some fermenting organism, which may reach any part of the urinary tract with or without calculi or glycosuria; and when there are fistulas between the bladder and some hollow viscera. 15 The term “emphysematous pyelonephritis” was introduced by Schultz and Klorfein in 1962, highlighting the higher prevalence of this disease in women and in patients with diabetes mellitus in the presence of enterobacteria. 16 Other case series also show that emphysematous pyelonephritis can occur in patients with ureteral obstruction and in immunocompromised patients.1,4,6
A meta-analysis found an overall mortality rate of 25% (11%–42%), a worse prognosis when patients received only conservative treatment (volume resuscitation and antibiotics), in the presence of bilateral emphysematous pyelonephritis, and in the presence of thrombocytopenia. Diabetes mellitus was not a risk factor for mortality. 5 Huang and Tseng classified emphysematous pyelonephritis into five groups according to severity 17 :
1. Gas limited to the collecting system.
2. Gas limited to the renal parenchyma only.
3A. Gas perinephritic extension or abscess.
3B. Gas extension beyond Gerota’s fascia.
4. Bilateral emphysematous pyelonephritis or in a single kidney (highest mortality rate: 50%).
Based on these studies, the possible risk factors for a worse prognosis in this case were conservative treatment and infection in a solitary kidney. This patient was a female with malignant ureteral obstruction undergoing oncologic treatment with a functionally excluded right kidney. Knowing the severity of the disease was important in the decision-making process with the patient and her family.
Two systematic reviews with meta-analysis concluded that clinical management and percutaneous gas drainage is the best approach (mortality from 13.5% to 18%), leaving radical nephrectomy for special cases.4,6 Paradoxically, in the present case, emphysematous pyelonephritis occurred in the presence of a drainage catheter. In addition, radical nephrectomy was not feasible due to functional exclusion of the contralateral kidney. Possible reasons for this infection were the presence of neoplastic disease, obstruction, and manipulation of the kidney prior to infection. Considering the progression of the metastatic disease, the high risk of death associated with emphysematous pyelonephritis, and the risks of dialysis and its chronic maintenance for the patient, the decision was to treat the patient conservatively with antibiotics.
In the few cases describing emphysematous pyelonephritis in cancer patients, there is an association with diabetes mellitus or fistulas in clear renal cell carcinoma, urothelial carcinoma, hepatitis B virus hepatocarcinoma, and non-small cell lung cancer.9–12 Of these, only the patient with lung cancer had survived the infection, three patients had diabetes mellitus, and one patient had a fistula directly in the kidney.9–12 Here, we present the first case of emphysematous pyelonephritis after urinary diversion by percutaneous nephrostomy (a procedure also used to treat this infection) in a patient with cervical cancer without diabetes mellitus.
A vesicotumoral fistula with gas was found in the bladder 2 months before the diagnosis of emphysematous pyelonephritis. Thereafter, the gas disappeared although the size of the fistula increased. The time between the last percutaneous nephrostomy and the development of infection was 8 days. There was no gas in any part of the urinary tract other than the left kidney. Possible causes of emphysematous pyelonephritis include ureteral obstruction, immunologic dysfunction due to neoplastic disease, and prior oncologic treatment. Possible causes that require further investigation include multiple manipulations, infections, and the consequent use of antibiotics prior to emphysematous pyelonephritis.
Both the double-J catheter and percutaneous nephrostomy are established techniques for restoring renal function in the setting of malignant ureteral obstruction. The double-J catheter would be the procedure of choice because it is less invasive. However, its use is strongly influenced by the local anatomy. Besides the risk of persistent dilatation of the urinary tract and consequent recurrence of pain, which ranges from 21.6% to 46% up to 6 months after its passage, percutaneous nephrostomy is gaining importance.18–20
It is noteworthy that gas developed in the left pyelocaliceal system 8 days after percutaneous nephrostomy, with deterioration of renal function, even in a kidney that had already been drained by the nephrostomy itself, and without improvement of renal function after treatment and resolution of the urinary tract infection. This was different from other nephrostomy catheter-associated infections. Even with a poor evolution of the neoplastic disease, followed by several complications of renal function and infections, this patient always presented herself confident and hopeful in the oncological treatment. Perhaps because of this, pain was not her main complaint throughout the treatment, which was controlled with low doses of methadone.
Her family was relieved when she started dialysis because the treatment helped to improve her uremic encephalopathy until her death.
This study has several limitations, the most important of which are related to its design. Therefore, we cannot generalize the therapeutic management used in this patient, and each case must be studied uniquely. However, this case is peculiar both in terms of diagnosis and therapeutic management.
Conclusion
This case illustrates the difficulty of managing advanced neoplastic disease. Emphysematous pyelonephritis should be considered as a differential diagnosis when urinary diversion is performed and renal function does not improve, even in the absence of fever. Focus on the patient’s needs and follow-up with a palliative care team is essential. Prognosis and treatment options should be discussed with the patients and their families or caregivers, including continuation of hemodialysis to improve symptoms. This can provide relief from the suffering of a devastating and rapidly progressing disease in the last moments of the patient’s life.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X231182532 – Supplemental material for Emphysematous pyelonephritis after urinary diversion by percutaneous nephrostomy in patient with advanced cervical cancer: A case report
Supplemental material, sj-docx-1-sco-10.1177_2050313X231182532 for Emphysematous pyelonephritis after urinary diversion by percutaneous nephrostomy in patient with advanced cervical cancer: A case report by Jeferson Rodrigo Zanon, Henrique Durante, Leandro de Medeiros Nóbrega, Guilherme Accorsi, Priscila Grecca Pedrão and Ricardo dos Reis in SAGE Open Medical Case Reports
Footnotes
Acknowledgements
The authors would like to acknowledge Joyce Ramos de Almeida and the Researcher Support Center of the Jales Cancer Hospital for their help in organizing the necessary documentation for the Review Board—Research Ethics Committee.
Author contributions
JRZ, HD, and RR concepted and designed the study, provided data acquisition and data interpretation, and drafted the article. All authors revised the article for important intellectual content, approved the submitted version of the manuscript, agreed to be personally accountable for the individual’s own contributions and to ensure that questions pertaining to the accuracy or integrity of any portion of the manuscript, even one in which the author was not directly involved, are appropriately investigated, and resolved, including with documentation in the literature if appropriate.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient’s son (next legally authorized representative of the deceased subject kin) for the patient anonymized information to be published in this article.
Research ethics and patient consent
Ethical approval of this case report was obtained from Barretos Cancer Hospital—Pio XII Foundation Review Board (Comitê de Ética em Pesquisa—CEP—do Hospital de Câncer de Barretos—Fundação Pio XII) under the Certificate of Presentation for Ethical Consideration number 56655322.8.0000.5437. This research was conducted regarding the Declaration of Helsinki, and the case report was documented following the CARE Statement.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.