
Abstract
VACTERL syndrome is a multisystem congenital anomaly. The potential findings include vertebral, anorectal, and cardiac anomalies; tracheoesophageal fistula/esophageal atresia; and renal and limb anomalies. This case report presents a pregnant woman in her early 30s presenting with multiple fetal anomalies suggesting this diagnosis.
Keywords
VACTERL syndrome is an uncommon multisystem congenital anomaly with findings that tend to co-occur. These findings may include combinations of vertebral, anorectal, and cardiac anomalies; tracheoesophageal fistula/esophageal atresia; and renal and limb anomalies.1–5 A case is presented with multiple fetal anomalies seen during prenatal sonography that suggested this diagnosis.
Case Report
A woman in her early 30s, G2P1, presented to the antepartum unit for preterm labor. Her physical examination predicted her to be three weeks greater than dates by last menstrual period (LMP). She was 32 weeks 3 days by sonographic evaluation, including all biometric measurements (biparietal diameter, head circumference, abdominal circumference, femur length, humerus length), which was consistent with her LMP dating of 32 weeks 1 day. The family had recently relocated from another state due to her husband’s military service. By her account, she had two prior sonographic examinations at a small community hospital where they said the heart was enlarged but no other anomalies were noted. Her prior pregnancy was unremarkable, with a normal three-year-old daughter at home. She was in good physical condition, was a nonsmoker, and had no history of drug abuse. She had no history of diabetes or hypertension. She was referred for sonographic evaluation. The obstetric sonogram was performed using an Acuson Sequoia 512 imaging unit (Acuson, Mountain View, California) with a 6-MHz curved linear array. Because of the cardiac findings, a fetal echocardiogram also was ordered and performed by the same sonographer following the obstetrical sonogram. The same machine and transducer were used.
The sonographic findings included polyhydramnios with an amniotic fluid index (AFI) measured at 31 cm as well as nonvisualization of the stomach in the fetal abdomen (Figures 1 and 2). Further evaluation of the fetal neck and thorax revealed a blind-ending esophagus with possible anterosuperior communication with the trachea. This sonographic finding suggested esophageal atresia with tracheoesophageal (T-E) fistula (Figure 3).

Polyhydramnios.
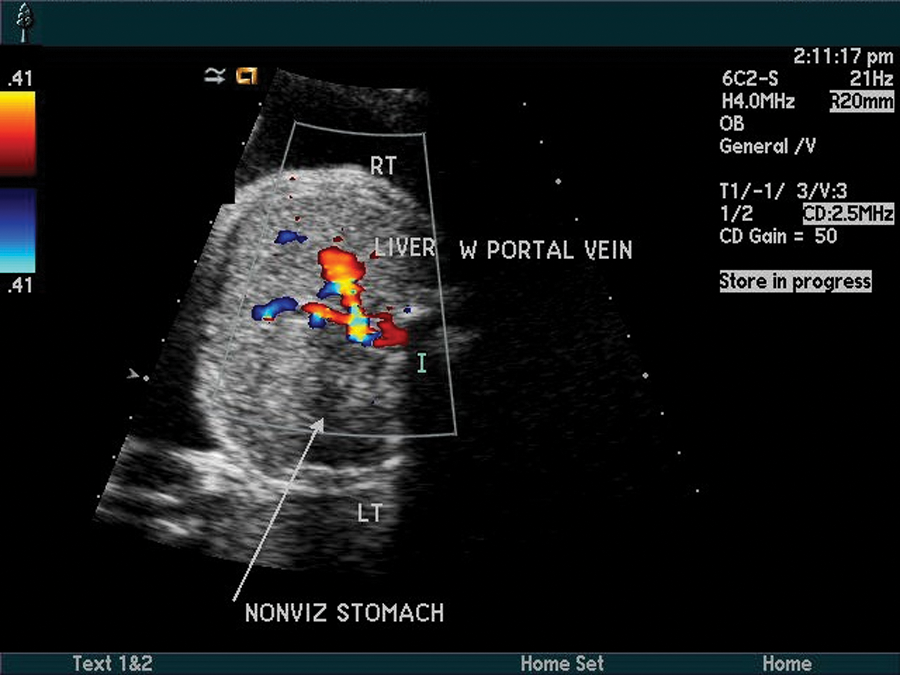
Nonvisualized stomach in fetal abdomen. LT, left; RT, right.
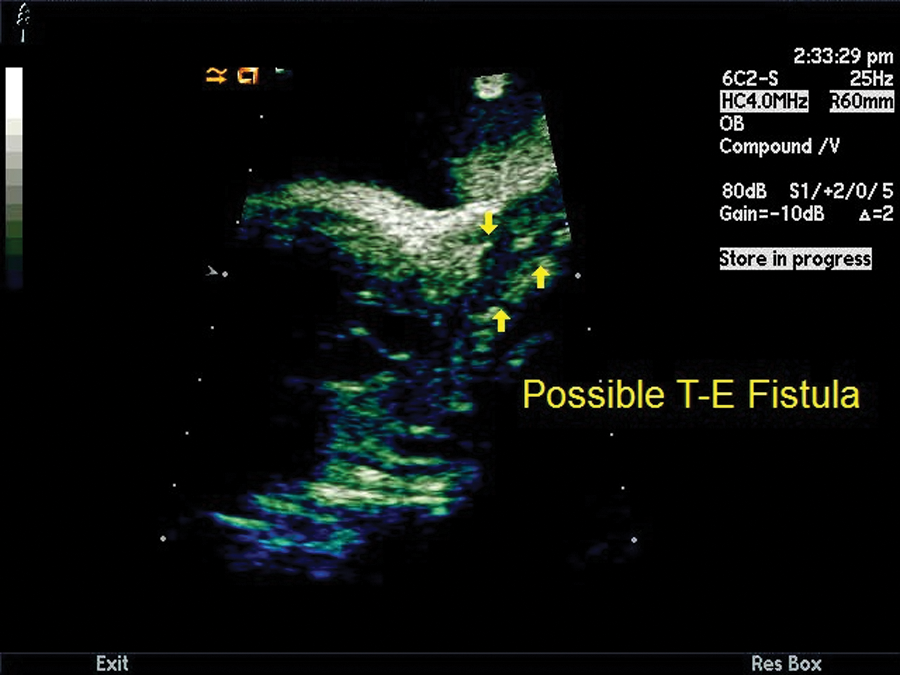
Tracheal atresia/tracheoesophageal (T-E) fistula. There is a blind-ending esophagus with anterosuperior connection with the trachea. This finding along with nonvisualization of the stomach further supported esophageal atresia.
Within the thorax, there were mesocardia and cardiomegaly with the cardiac axis measured at 5 degrees (normal, 45 ± 15 degrees) and the cardiothoracic ratio measured at 47% (normal, approximately 33%) (Figure 4). Cardiac anomalies included truncus arteriosus type 2A with a single truncal valve and the pulmonary arteries arising from the truncus posteriolaterally (Figures 5 and 6). The truncal valve appeared thickened with an associated malaligned subarterial ventricular septal defect (VSD). There appeared to be left atrial isomerism with both left atrial appendages well visualized on the lateral aspect of both atria (Figure 4). Despite the suggestion of left atrial isomerism, the inferior vena cava (IVC) was noted entering medially but directly into the atria without obvious interruption of the IVC. 6 A right aortic arch was also demonstrated (Figure 5).

Mesocardia with possible left atrial isomerism. Arrows point to both left atrial appendages.
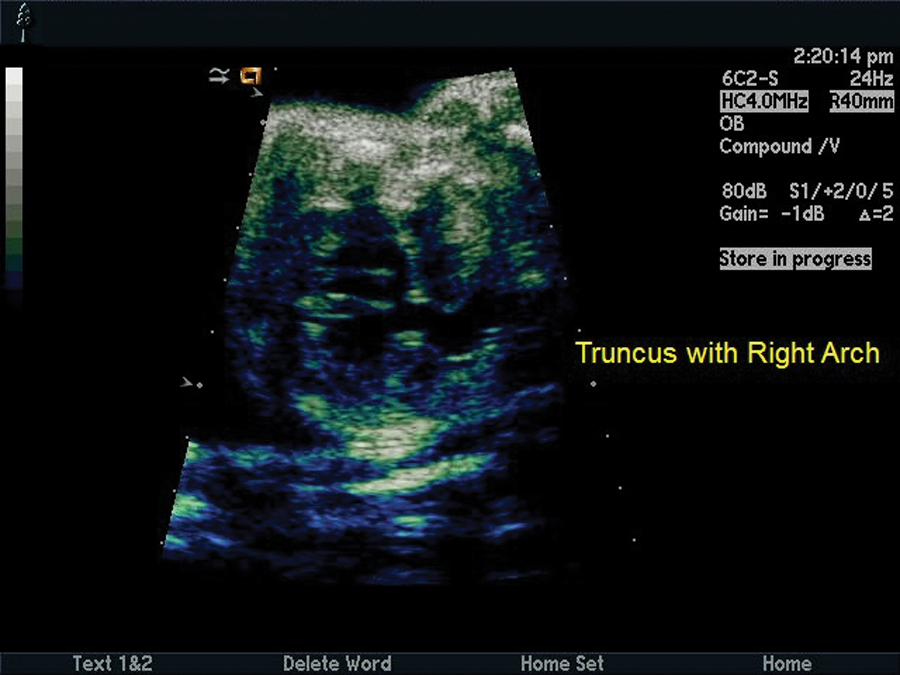
Truncus arteriosus. Single outflow tract with thickened truncal valve overriding the ventricular septum. Subarterial ventricular septal defect (VSD) and right aortic arch are noted.
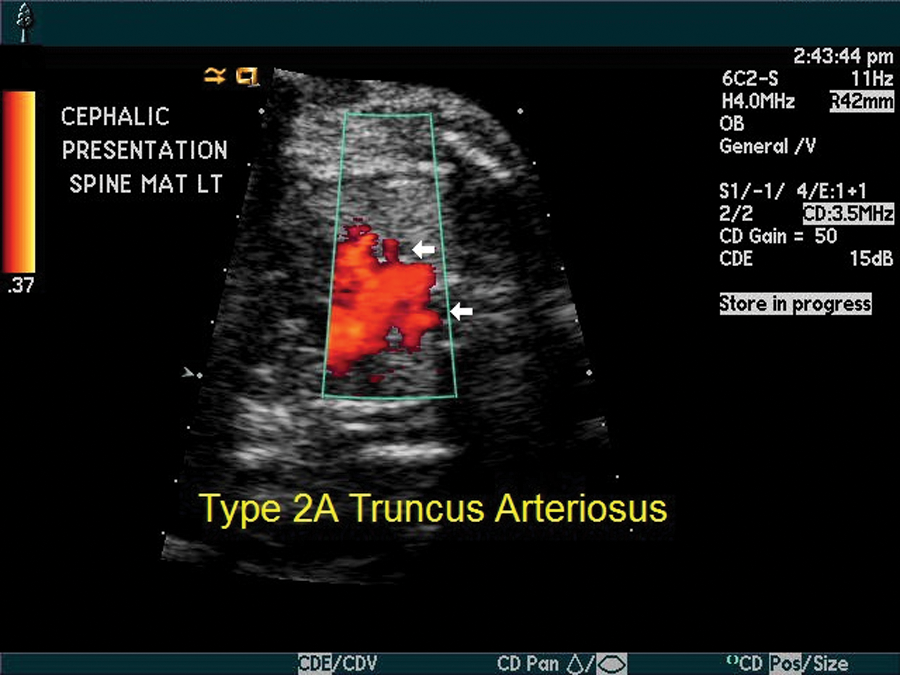
Truncus arteriosus. Pulmonary artery branches appear to arise posteriolaterally from the truncus, suggesting type 2A truncus arteriosus.
There was mild scoliosis of the lumbar spine with left lateral hemivertebrae (Figure 7). No other spinal anomalies were noted. A solitary right kidney was noted in the fetal abdomen without hydronephrosis (Figure 8). No limb abnormalities were demonstrated. A final sonographic finding was the presence of a single umbilical artery with only the right umbilical artery visualized (Figure 9). The sonographic findings in this case are summarized in Table 1.

Coronal image of the spine demonstrates a lateral hemivertebrae.
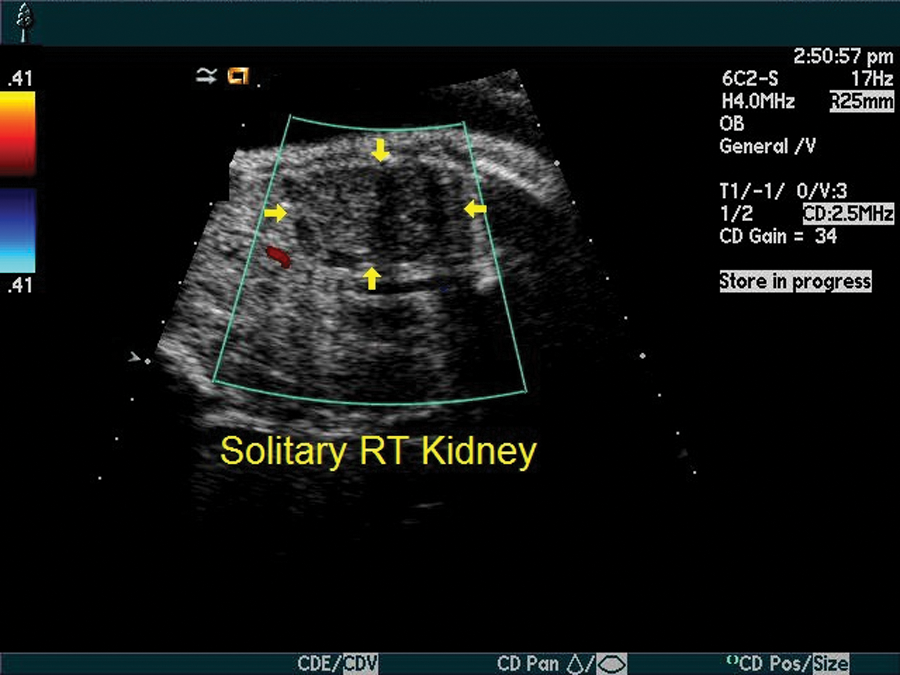
Unilateral renal agenesis. Solitary right (RT) kidney was demonstrated in the fetal abdomen.
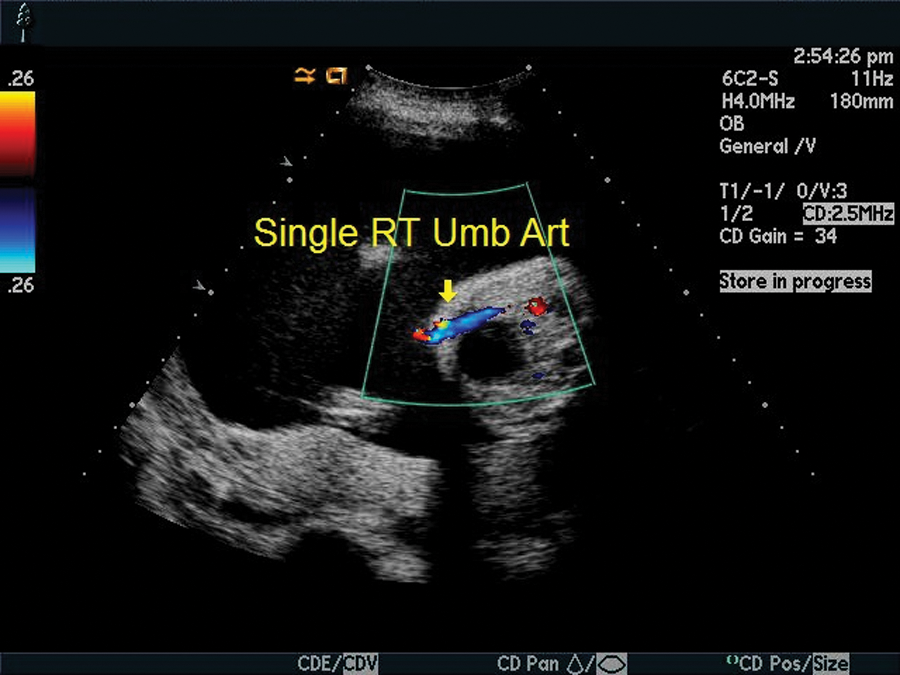
Single umbilical artery. The left umbilical artery was not visualized at the level of the cord insertion. RT, right.
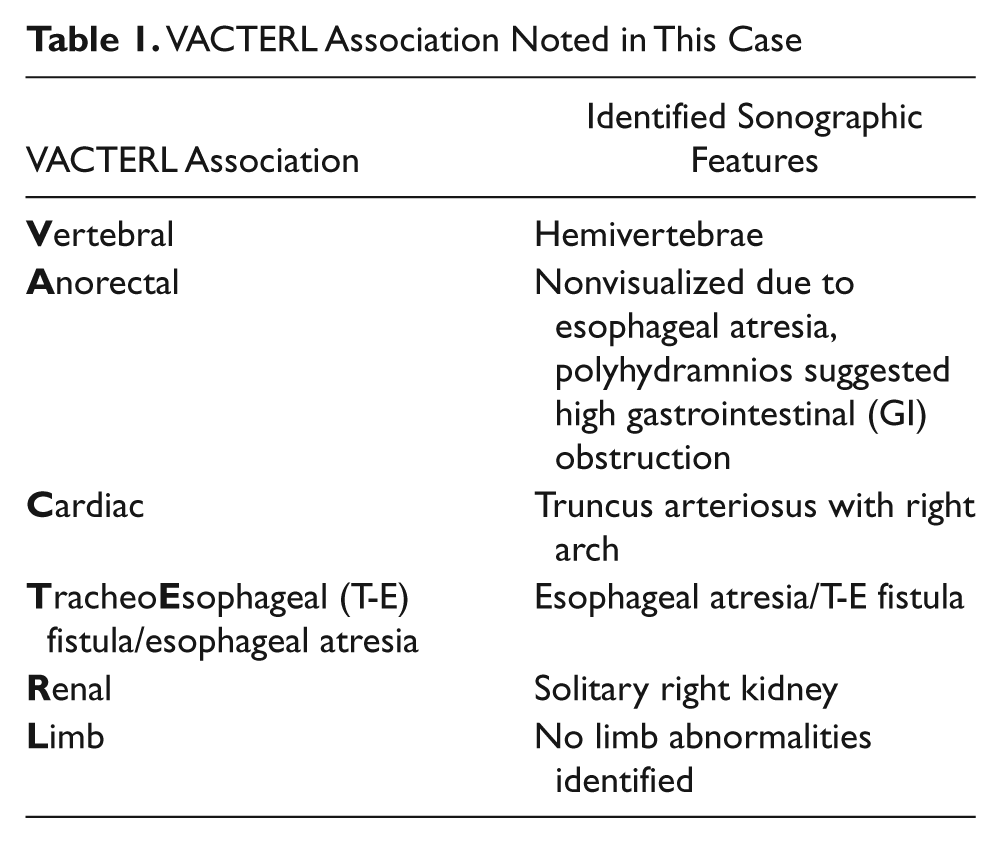
VACTERL Association Noted in This Case
The discharge plan from our antepartum unit was for the infant to be delivered at our tertiary hospital; however, the mother went into preterm labor, and the infant was delivered emergently at 36 weeks’ gestation at the military hospital near her home. By report, the infant passed away on day two of life due to severe complications of the T-E fistula. The infant was not transferred to our hospital, and the details of the neonatal care provided at the delivering hospital were not made available to our facility.
Discussion
VACTERL syndrome is a multisystem congenital anomaly. The potential findings include vertebral, anorectal, and cardiac anomalies; tracheoesophageal fistula/esophageal atresia; and renal and limb anomalies. VACTERL was first described as VATER by Quan and Smith in 1973 7 but was later expanded to include cardiac anomalies and a less strict definition of limb abnormalities by Temtamy and Miller in 1974. 8 The incidence of VACTERL is estimated to be approximately 1 in 10,000 to 1 in 40,000 live births. 6 The VACTERL association is considered when a minimum of three features are demonstrated (Table 1). 6 There is a much higher incidence of VACTERL in offspring of diabetic mothers, 6 although in the case presented, the mother was not diabetic. The incidence of VACTERL defects by type are described below.
Vertebral anomalies as a whole occur in approximately 24% of all cases of VACTERL.4,9 The vertebral anomalies noted include, but are not limited to, tethered cord, hemivertebrae, butterfly-shaped vertebrae, and absent or additional ribs.
Anorectal anomalies, including imperforate anus and duodenal atresia, occur in 14.3% of cases. 9 The case presented demonstrated an absent stomach and polyhydramnios suggesting a higher obstruction at the esophagus.
Cardiac lesions are varied with VACTERL association, but the most common type of cardiac defects are ventricular septal defects (22.3%). 6 The incidence of cardiac defects overall is 32%. This case reported severe cardiac anomalies involving truncus arteriosus, mesocardia (heart pointed to midline), and possible left atrial isomerism. Isomerism is a condition where there are two left or right atria. In left atrial isomerism, as seen in this case, there is an association with polysplenia and interruption of the IVC with azygous continuation to the superior vena cava (SVC). Truncus arteriosus represents 1% to 2% of congenital heart defects in live-born infants 10 and occurs in approximately 5 to 15 of 100,000 live births. 11 There is no significant difference in the incidence in the United States compared with other countries. The mortality and morbidity of truncus arteriosus without surgical intervention are varied. The median age at death ranges from two to three weeks. The cause of death in unrepaired cases is usually cardiac arrest or failure due to insufficient systemic arterial blood supply. Hatemi et al in 2008 11 described the severe postnatal complications that can be expected with repair of the cardiac defects in patients with VACTERL syndrome. These are related to the noncardiac components, specifically those associated with esophageal atresia/tracheoesophageal fistula repair. They reported a case study where there was a successful cardiac repair of multiple VSDs but near-lethal complications, including postoperative pneumonia, aspiration, tracheomalacia, and pulmonary hypertension.
Esophageal and tracheoesophageal atresia is a relatively common abnormality that can occur as an isolated finding or in conjunction with other anomalies. The global incidence is approximately 1 in 3500 births. 1 In the United States, the incidence of esophageal atresia is 1 case in 3000 to 4500 births. Internationally, the highest incidence of this disorder is in Finland, where it is 1 case in 2500 births. 2 Of the associated anomalies, the VACTERL association is the most common. Shaw-Smith 3 has proposed that there may be a genetic etiology to esophageal atresia and the VACTERL association—specifically, the FOX transcription factor gene cluster at 16q24.1. Microdeletions at this genetic focus may cause a broad spectrum of anomalies resembling that of the VACTERL association.3,5 The role of genetic testing using high-resolution microarrays may be helpful in further delineating the role of the 16q24.1 locus in the etiology of severe developmental malformations such as the VACTERL association. In the case presented, the mother was referred to a regional perinatologist for consultation and genetic counseling at 33 weeks’ gestation, but no information regarding any genetic screening that may have been done was available to our hospital after discharge.
The incidence of renal anomalies with VACTERL is approximately 17%.9,12 Of the renal anomalies, reflux is the most common anomaly (7.1%), followed by horseshoe kidney, bilateral atresia, solitary kidney (as seen in this case), uretero-pelvic junction obstruction, and dysplastic kidney. 13
Limb or skeletal anomalies are seen in approximately 8.9% of VACTERL cases.6,13 The most common is absent or deformed radius, followed by digital anomalies and hip dysplasia.
In addition to the typical features of VACTERL syndrome, a single umbilical artery is a common finding, 9 as was seen in this case. Another anomaly that has a phenotypical overlap with VACTERL is the 22q11 deletion syndrome. It has been associated with esophageal atresia and cardiac and renal anomalies but does not usually include vertebral and anal atresia. 9
Because of the complicated patterns of the co-occurrence of these anomalies, when sonographic findings of an anomaly suggest the possibility of VACTERL syndrome, a thorough diagnostic workup for the related findings is indicated. With increased availability of surgical treatment for tracheoesophageal fistula and congenital heart defects, enhanced ventilator support and neonatal anesthesia, and improved neonatal intensive care management, infants with the prenatal diagnosis of VACTERL syndrome now survive to adulthood much more frequently than children diagnosed just a few decades ago.6,13 A more thorough, uniform diagnostic workup and a low threshold for investigation of the primary disorder may enhance the quality of clinical management in these patients.
Conclusion
This case demonstrates a prenatal diagnosis based on at least four components of the VACTERL syndrome, including hemivertebrae, truncus arteriosus with right aortic arch, esophageal atresia and T-E fistula, and a solitary right kidney. Additional findings included polyhydramnios and a single umbilical artery. The original discharge plan had been for the infant to be born at our tertiary hospital. The mother went into preterm labor and delivered the infant at the military hospital near her home. The infant was not transferred to our hospital and by report passed away on day two of life secondary to severe complications of the T-E fistula. The details of the neonatal care provided at the delivering hospital were not made available to our facility, but even without postnatal data, the original findings were strongly diagnostic for the VACTERL syndrome. When sonographic findings of anomalies such as these do suggest the VACTERL syndrome, a complete, thorough diagnostic workup is indicated to help direct the best possible clinical management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.