
Abstract
Tracheal diverticulum is a rare and easily overlooked complication following tracheoesophageal fistula repair that poses substantial challenges in airway management for anesthesiologists. We present a case of a 4-month-old girl with esophageal stenosis following tracheoesophageal fistula repair who was presented for repeated endoscopic balloon dilation. During the first two inductions of general anesthesia, endotracheal intubation appeared successful but resulted in unexpected ventilation failure. Successful ventilation was finally achieved after multiple attempts at intubation. Fiberoptic bronchoscopy revealed a tracheal diverticulum before the third induction of anesthesia, explaining the persistent ventilation difficulties. The patient was successfully managed with fiberoptic bronchoscopy–guided intubation while maintaining spontaneous respiration, allowing the endotracheal tube to bypass the diverticulum. This case highlights tracheal diverticulum as an uncommon cause of ineffective ventilation following intubation and suggests that fiberoptic bronchoscopy-guided intubation may be a preferable approach.
Introduction
Tracheoesophageal fistula (TEF) is a rare condition typically diagnosed in the neonatal period. Due to the life-threatening feeding difficulties and respiratory complications, TEF repair is usually performed within the first few days of life. To minimize scarring and reduce the risk of tracheal stenosis, TEF repairs are often conducted, leaving a residual fistula tissue measuring 1 to 2 mm. However, the expansion of this residual tissue into a diverticulum following TEF repair is an uncommon complication. 1 While asymptomatic tracheal diverticula typically do not require treatment, they can pose significant challenges in airway management during anesthesia. We encountered a case in which effective ventilation could not be achieved following intubation, and subsequent bronchoscopy revealed that the residual tracheal diverticulum, following TEF repair, was likely the cause.
Case reports
A 4-month-old girl with esophageal stricture after undergoing TEF repair at 10 days of life presented to the Department of Gastroenterology, West China Second University Hospital, in July 2023. Repeated esophagogastroduodenoscopy with esophageal dilation was scheduled every 2 weeks. General anesthesia with tracheal intubation was planned. During the first two inductions of anesthesia, mask ventilation was achieved without difficulty. The vocal cords were exposed by direct laryngoscopy, and a 3.5-mm inner diameter (ID) cuffed endotracheal tube (ETT) was passed through the vocal cords with no resistance at a depth of 10 cm from the incisors. However, there was an absence of chest rise, end-tidal CO2, and breath sounds. Subsequently, oxygen saturation (SpO2) began to decline. The ETT was then withdrawn, and mask ventilation was successfully reestablished. Considering the possibility of the tracheal tube tip slipping into the esophagus, a second intubation was performed with a visual laryngoscope, which directly visualized the ETT passing through the glottic opening (Figure 1(a) and (b)). However, there was still no evidence of successful ventilation. The ETT was again withdrawn, and mask ventilation continued. The anesthesiologist then asked for assistance, and another more experienced anesthesiologist performed a third intubation attempt, but ventilation still failed. Esophageal intubation was ruled out, and suspicion turned to a possible serious laryngospasm and tracheal spasm. Subsequent measures included deepening anesthesia, continuous epinephrine infusion, and airway surface anesthesia with lidocaine. Effective ventilation was finally achieved after several attempts to intubate.

The visual laryngoscope shows normal vocal cord anatomy and glottic opening (a), with the endotracheal tube (ETT) passing through the glottic opening (b).
A few weeks later, the girl was scheduled for the third endoscopic balloon dilation procedure. Considering that intubation by experienced anesthesiologists had failed to provide effective ventilation in the first two anesthesias, flexible fiberoptic bronchoscopy (FOB) was performed before the third anesthesia to identify if there were any tracheal abnormalities. The FOB revealed a blind pouch 3 cm below the vocal cords and 1.5 cm above the carina, with no signs of fluid or gas movement (Figure 2). We presumed that the ETT had been inadvertently placed into this false tracheal tract during our previous intubation attempts. After preoxygenation with 100% oxygen and nebulization with lidocaine, general anesthesia with preserved spontaneous respiration was induced using sevoflurane (1%–3%) in oxygen. Methylprednisolone 8 mg, atropine 100 µg, fentanyl 15 µg, and ketamine 3 mg were also administered. After loss of consciousness, a 3.5-mm ID cuffed ETT was successfully intubated past the diverticulum under FOB guidance and the ETT was placed 1 cm above the carina and 11 cm past the lips. Following this, 0.5 mg of atracurium was administered. The intraoperative course was uneventful. Due to the difficult intubation, the patient was transferred to the pediatric intensive care unit with tracheal catheter and extubated 3 days later. This case report was published with the written consent of the patient's guardian and conformed to the Case Report (CARE) guidelines. 2
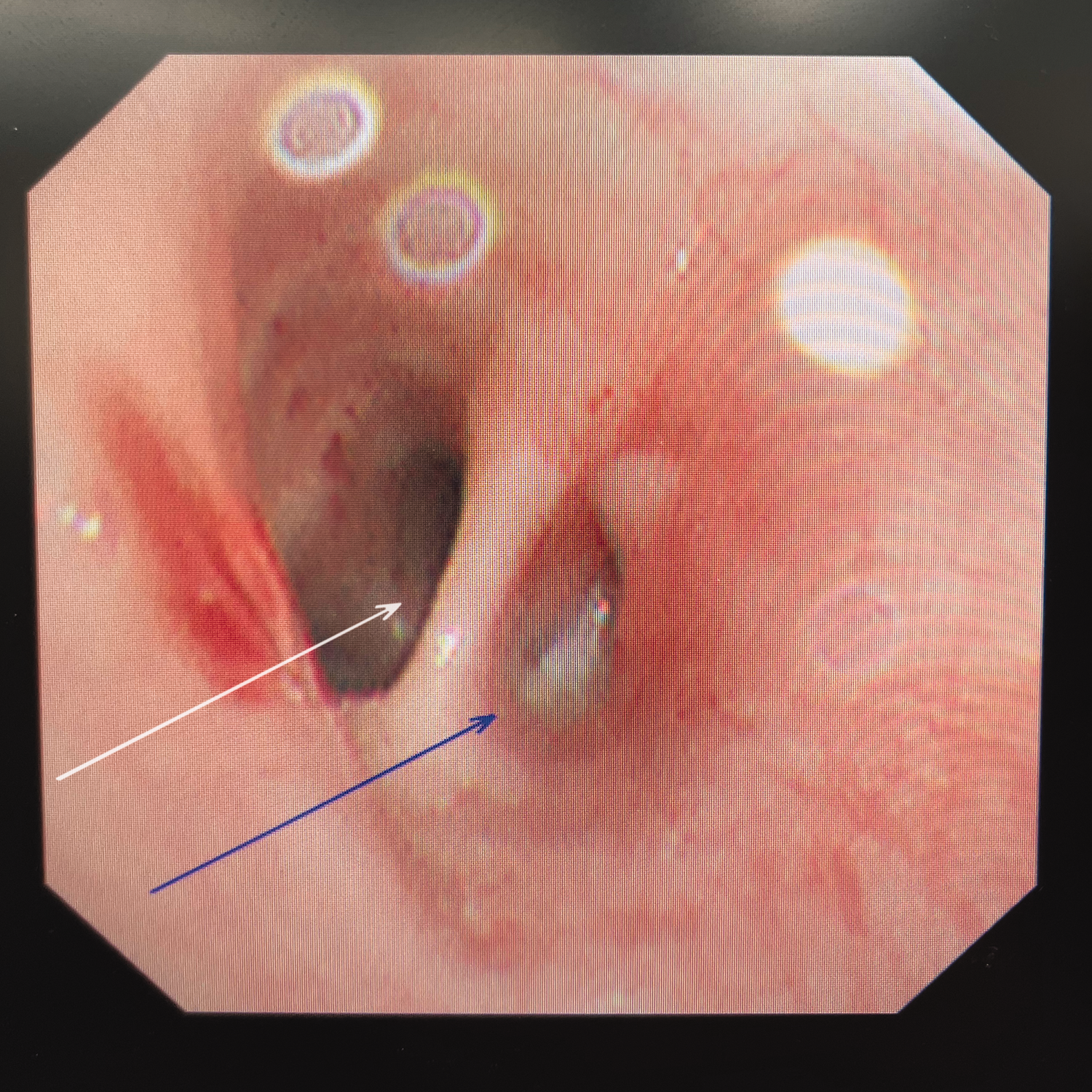
The fiberoptic bronchoscopy (FOB) shows the tracheal diverticulum (blue arrow) 1.5 cm above the carina (white arrow).
Discussion
The major challenges of tracheal diverticulum for anesthesiologists are difficulties in intubation and ventilation, as well as complications associated with positive pressure ventilation. Salhotra et al. 3 reported an unexpectedly difficult intubation in an 11-year-old boy with Lesch-Nyhan syndrome. A 6.5-mm ID endotracheal tube and progressively smaller tubes also failed to pass 1 cm beyond the vocal cords. In the postoperative period, a computed tomography (CT) scan revealed a tracheal diverticulum 9 mm below the vocal cords, which was the cause for difficulty in intubation. Moreover, a diverticulum can provide a false tract, and misplacement of the endotracheal tube into the diverticulum can lead to difficulties in ventilation. This was also observed in our case. Similarly, Merritt et al. 4 reported a similar situation when administering anesthesia to a 6-month-old infant after TEF repair. Mask ventilation and endotracheal intubation were performed with ease. However, no evidence of successful ventilation was observed after placement of the ETT. The wall of a tracheal diverticulum is weaker than normal, especially in the case of an acquired diverticulum, where the wall is predominantly composed of respiratory epithelium. There is a risk of diverticulum perforation under positive pressure ventilation. In earlier cases, mediastinal and subcutaneous emphysema have been reported after intubation due to accidental perforation of the tracheal diverticulum.5,6 Fortunately, in our case, no such adverse events occurred.
Generally, tracheal diverticula were confirmed through virtual chest CT and flexible endoscopy. However, as shown in our case (Figure 3(a) to (d)), a preoperative CT failed to detect this abnormality, and the diverticulum was finally identified by bronchoscopy. This discrepancy may be attributed to the dynamic collapse of the diverticulum during quiet breathing, its pressure-dependent expansion during mechanical ventilation, or its location at a bronchial.7–9 For patients diagnosed with tracheal diverticula, regional anesthesia is the preferred option to avoid airway-related complications. If general anesthesia is required, a supraglottic airway device, such as a laryngeal mask airway, may be considered. If tracheal intubation is necessary, the positional relationship between the diverticulum and the catheter tip, as well as the presence of airway stenosis, should be assessed first. This will help in selecting an appropriate ETT. For patients undergoing general anesthesia with tracheal intubation, induction with preserved spontaneous breathing or fiberoptic bronchoscopy-guided awake intubation is considered a more suitable approach. FOB can be used to ensure that the endotracheal tube tip is placed at the appropriate depth, avoiding the diverticulum at the distal end of the tube. Otherwise, it may cause diverticulum perforation due to excessive ventilation pressure. Some reports suggest that using a double-lumen endotracheal tube instead of a single-lumen tube can help occlude the diverticulum opening and prevent perforation. 10 However, it is more likely to cause airway mucosal damage than single-lumen endotracheal intubation. Therefore, double-lumen endotracheal tubes may be more suitable for distal tracheal diverticula or when surgical procedure requirements necessitate one-lung ventilation.

Preoperative chest computed tomography (CT) shows no anatomical abnormalities of the airway. The superior level of the tracheal carina (a, b) and the tracheal carina level (c, d) are indicated.
For anesthesiologists who have received standardized training, the inability to ventilate after intubation is not a common occurrence, especially when the endotracheal tube passes through the glottis under direct laryngoscopy. According to the algorithm from the Practice Guidelines of the American Society of Anesthesiologists Task Force, unconscious patients who ventilate well with a mask are managed through the nonemergency pathway. 11 It becomes crucial to adopt a differential approach to exclude potential causes, rather than repeatedly attempting intubation, which may lead to swelling of the vocal cords and airway, resulting in difficulties with mask ventilation. In emergency airway situations, patients are more likely to be at risk of life-threatening complications. In our case, the most likely initial cause of ventilation failure was esophageal intubation, which is a common cause of ineffective ventilation after intubation. Therefore, a second intubation was performed under laryngoscopy, but there was still no effective ventilation. We then considered the possibility of severe airway spasm, which is more likely to occur during intubation in children. Other common causes, such as equipment failure and catheter obstruction, were ruled out in our case. After excluding these common causes, altered tracheal anatomy should be considered, particularly in patients with a history of previous surgeries or medical conditions involving the trachea. 12 We did not consider this possibility during the first two anesthesias. FOB can clearly show the structure of the trachea and the position of the endotracheal tube tip.
Conclusion
This case report highlights the need to be wary of tracheal diverticulum as a potential complication following the repair of a TEF, which may cause difficulty in intubation, airway compromise, or an inability to provide effective ventilation. For the future anesthetic management of a patient with a tracheocele, initial intubation with a fiberoptic bronchoscope could increase the success of the first-attempt intubation and reduce the risk of airway injury.
Footnotes
Acknowledgments
The authors gratefully acknowledge all participants for their contribution to this study.
Author contributions
Conceptualization: Shanshan He, Bo Tao, Teng He.
Data curation: Shanshan He, Bo Tao.
Formal analysis: Shanshan He, Bo Tao.
Investigation: Shanshan He, Bo Tao.
Methodology: Shanshan He, Bo Tao.
Validation: Teng He.
Writing—original draft: Shanshan He.
Writing—review & editing: Bo Tao, Teng He.
Data availability statement
The original contributions presented in the study are included in the article, and further inquiries can be directed to the corresponding authors.
Declaration of conflicting interests
The authors have no conflicts of interest to disclose.
Ethics statement
Ethical committee approval was not required for this case report. The patient’s guardian was informed that any personal medical information included in the report would be redacted or anonymized to protect privacy. Written informed consent was obtained from the patient’s guardian for the publication of this case report. The patient and her guardian hope that sharing her experience will provide the medical community with valuable insights to improve the diagnosis and treatment of future patients.
Funding
This research did not receive any funding.