
Abstract
When performed by a trained sonographer, fetal echocardiography can be instrumental in identifying cardiac pathology and abnormal cardiac physiology before a baby is born. Even though the diagnostic accuracy of a fetal echocardiogram can be limited by maternal body habitus, gestational age, and fetal position, sequential exams allow for detailed analysis of the cardiac structures. Early identification and diagnosis of intrauterine cardiac anomalies and subsequent pregnancy management and delivery planning are essential to providing the best possible outcome for fetuses born with heart defects. In this case study, we describe a rare combination of congenital heart defects diagnosed in an uncontrolled type 1 diabetic mother while in her second trimester of pregnancy.
Keywords
Introduction
Type 1 diabetes is a chronic metabolic disease in which the pancreas produces little or no insulin, leading to elevated blood glucose levels. These elevated glucose levels interrupt normal cellular metabolism and eventually lead to organ dysfunction. Human studies have demonstrated a strong link between maternal glycemic level, as indicated by the association of plasma glucose and HbA1c levels, with the incidence of congenital malformations in offspring.1,2 Diabetic embryopathy describes the relationship between diabetes and congenital birth defects and fetal mortality. 3
Atrioventricular septal defects (AVSDs) have an incidence of 4 to 5.3 per 10 000 live births. 4 This complex congenital heart defect consists of a primum atrial septal defect (ASD), an inlet ventricular septal defect (VSD), and a common atrioventricular (AV) valve (Figure 1). In some instances, a common AV valve can preferentially loom above one ventricle more so than the other; thus, the appearance of an unbalanced canal can become more evident as the pregnancy progresses. When this occurs, the contralateral ventricle can be mildly to severely hypoplastic. In embryos of diabetic pregnancies, early development of the endocardial cushions is inhibited. 3
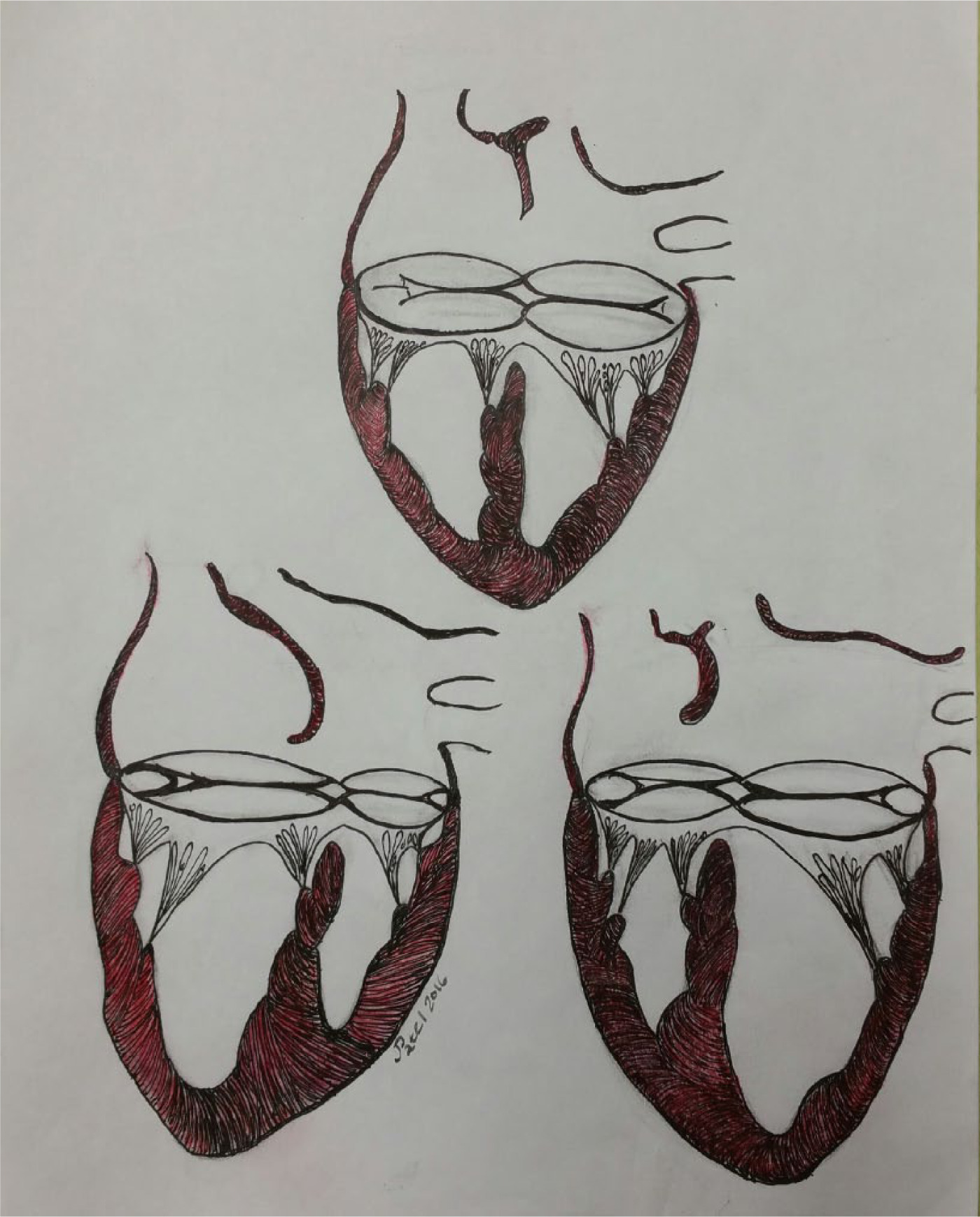
(Top) complete balanced atrioventricular septal defect; (left) complete unbalanced atrioventricular septal defect/right ventricle dominant; (right) complete unbalanced atrioventricular septal defect/left ventricle dominant. Image by Jayur Patel.
Common arterial trunk (truncus arteriosus) is also a rare type of heart defect, affecting fewer than 1 out of every 10 000 babies. 5 In this condition, a single arterial vessel leaves the heart, giving rise to the aorta, branch pulmonary arteries, and coronary arteries. A large subarterial VSD is found in the majority of patients with truncus arteriosus. 6
Development of the cardiac outflow tract requires cell migration from the neural crest. These cells contribute significantly to the septation of the outflow segment and the formation of the great vessels. Therefore, malformations in the outflow segment may be due to impaired neural crest cell migration. 3
Case Report
A G10/P3/A6 patient in her early 30s was referred by her perinatologist for fetal echocardiography secondary to a diagnosis of hypoplastic left ventricle and single outflow tract. It was a singleton pregnancy at 20 weeks 6 days. The patient’s medical history was positive for insulin-dependent diabetes and obesity. Maternal medications included prenatal vitamins once a day, Humalog 12 u TID, and Lantus 35 units HS. Her glycosylated hemoglobin level (HbA1c) at the first obstetrician’s visit was 12%.
A fetal echocardiogram was performed using a Philips IE33 (Koninklijke Philips Electronics, Netherlands) with a C5-1 curvilinear probe. Fetal imaging was limited due to poor acoustic windows secondary to maternal body habitus and fetal position. Initially on our first scan, the fetus was located in a cephalic presentation with the stomach and cardiac apex on the left, indicating abdominal situs solitus and levocardia. There was evidence of a primum atrial septal communication and a perimembranous ventricular septal defect. There was a single AV valve without evidence of stenosis and regurgitation, leading into two ventricles. The right ventricle was normal in size, whereas the left ventricle was hypoplastic and non-apex forming. When an anterior sweep was performed to assess the outflow tracts, there were two parallel outflow tracts identified; therefore, a diagnosis of unbalanced complete AVSD with double outlet right ventricle (DORV) was given (Figure 2).
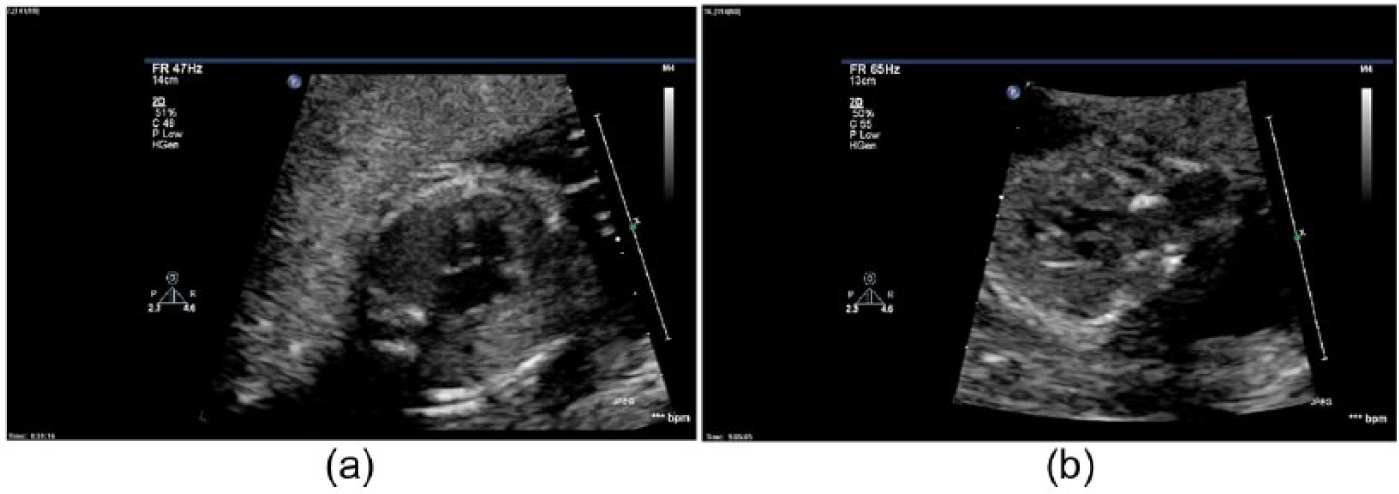
(a) Complete unbalanced atrioventricular septal defect. (b) What appears to be double outlet right ventricle.
At 23 weeks 6 days gestation, subsequent fetal cardiac exam demonstrated an unbalanced appearance of the ventricles with a greater than 50% override of a single truncal vessel, mild dilation of the right ventricle, and small appearance of the left ventricle. Therefore, the working diagnosis was changed to unbalanced complete AVSD with common arterial trunk (Figure 3). A fetal echocardiogram was then scheduled at the local children’s hospital and the diagnosis was confirmed. A meeting with the pediatric cardiothoracic surgeon and a tour of the cardiac intensive care unit were arranged.
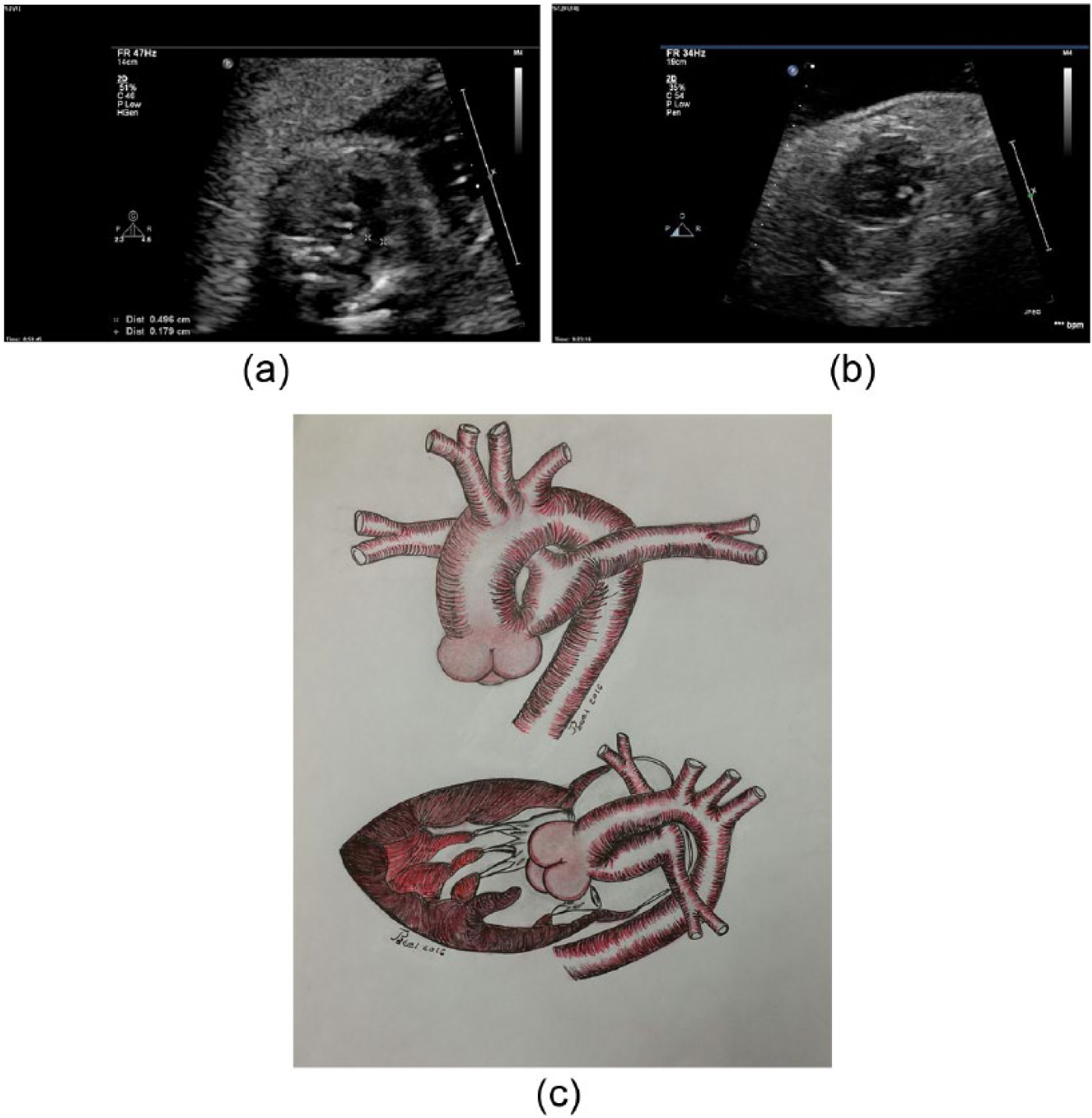
(a) Single outflow with small main pulmonary artery segment. (b) Single outlet with septal override. (c) Common arterial trunk, type 1. Image by Jayur Patel.
During the patient’s final fetal echocardiogram in the office at 34 weeks 6 days, the common AV valve was noted to have minimal regurgitation and there was flow acceleration seen throughout the truncal valve and ascending aorta with a velocity of 1.54 cm/s. In some of the images, there appeared to be a narrowing of the descending aorta by color Doppler, indicating possible coarctation. This exam was also limited due to poor acoustic windows secondary to maternal body habitus. At 37 weeks 2 days gestation, the patient presented to her obstetrician’s office for her weekly fetal surveillance and was found to have a fetal demise.
Discussion
The rudimentary cardiovascular system makes its appearance at approximately 3 weeks after conception, with the first heartbeat occurring at approximately 21 to 22 days. The 4th and 7th week mark the formation of the four-chambered heart. The endocardial cushions form, grow, and fuse, dividing the atrioventricular canal. If blood flow energy is altered in any way during this process, preferential blood flow to the right or left side of the canal can instigate the beginnings of an unbalanced chamber formation.
The cardiac crux is formed from the central membranous section and surrounding muscular part of the ventricles. This allows the right ventricle to communicate with the pulmonary artery and the left ventricle to communicate with the primitive aorta. This process is another critical area that could elicit streaming of the mixed flow to one outflow tract more so than the other.
Congenital birth defects in infants of diabetic mothers have been found to be associated with pregestational diabetes that is uncontrolled in the first trimester of pregnancy. 7 These defects can involve the craniofacial structures, cardiovascular system, musculoskeletal system, and the central nervous system. Continued blood glucose elevation throughout pregnancy can also lead to stillbirth, preterm delivery, and macrosomia. This case study demonstrates the appearance, treatment, and outcome of a fetus with two complex congenital heart defects born to an uncontrolled type 1 diabetic mother. A review of the literature yielded one similar case. 8
Conclusion
Noninvasive, detailed fetal echocardiography is instrumental in diagnosing congenital heart disease when performed by skilled sonographers. Early diagnosis allows time for patient education and delivery planning. In this case study, we demonstrated how the limitations of ultrasound can influence diagnostic accuracy and how follow-up examinations are necessary for confirmation and to assess the well-being of the fetus at risk.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.