
Abstract
Aneurysm of the main pulmonary artery is a rare finding in adults. This case presents the finding of an asymptomatic 4.6-cm pulmonary artery aneurysm in a woman in her early 60s detected on routine transthoracic echocardiography. All pertinent data are presented, and the clinical significance of the pulmonary artery aneurysm is discussed. The case emphasizes the importance of following a complete and thorough echocardiographic examination protocol. A limited study is likely to miss significant incidental findings such as is reported here, particularly if it involves the right heart.
Aneurysm of the ascending aorta or abdominal aorta is not uncommon. Aneurysm of the main pulmonary artery, first described by Walshe in 1862, 1 is a rare finding in adults. Indeed, it has been reported in only 1 of 14,000 autopsies. 2 Aneurysm of the main, right, or left pulmonary artery can be a manifestation of arteritis, Behcet disease (an autoimmune disorder), or congenital disease such as tetralogy of Fallot; be secondary to pulmonary stenosis or pulmonary hypertension; or result from intravenous drug use or mycotic infection.3–12 In this case, the finding of a main pulmonary artery aneurysm in a woman in her early 60s by transthoracic echocardiography is very unusual and instructive. Cardiologists and heart surgeons in community settings rarely if ever encounter aneurysm of the main pulmonary artery. Unless the aneurysm is huge or there is severe pulmonary hypertension, pulmonary stenosis, or other comorbidity, the approach is clinical management and monitoring with transthoracic echocardiography.
Case Study
A white woman in her early 60s was referred by her internists for a transthoracic echocardiogram evaluation because of heart murmur and history of porcine aortic valve placement in 2003. There was a history of old lacunar infarct on computed tomography (CT) in 2003, spinal stenosis, hypertension treated with metropolol, chronic musculoskeletal pain treated with Vicodin, and cholescystectomy and hernia repair in 2003. Body surface area was 2.23 m2 and blood pressure was 135/76 mm Hg. The chief complaint was general body aches, and an echocardiogram was ordered as a routine follow-up of aortic valve replacement and 2/6 systolic murmur. No transthoracic echocardiogram had been ordered in the past seven years.
The fully digital transthoracic echocardiogram was performed with a Biosound North America MyLab 30CV-X Vision (Esaote North America, Indianapolis, IN, USA) using a phased-array PA 230 probe with second harmonic imaging. Because of body habitus, the study was performed with the patient in a standard 30-degree torso up position but supine instead of left lateral decubitus. She was in no acute distress and narrated a history of occasional exertional dyspnea. There was no significant history of orthopnea or paroxysmal nocturnal dyspnea. There was a midline scar from a previous porcine aortic valve replacement in 2003. The calculated left ventricular ejection fraction (area-length method from apex) was 71%. Left ventricular systolic dimension was 5.3 cm and diastolic dimension 3.3 cm; the left atrial diameter was mildly dilated at 4.4 cm, with the left atrial area 17 cm2. The right ventricle demonstrated normal size and function with no flattening of the interventricular septum. There was trace mitral insufficiency with trace tricuspid insufficiency, with an estimated right ventricular systolic pressure of 37 mm Hg (simplified Bernoulli formula). There was complete plethora of the inferior vena cava. The porcine aortic valve was functioning normally and was free of calcific process with no insufficiency. Mean gradient across the aortic valve was 10 mm Hg, peak gradient was 20 mm Hg, and calculated aortic valve area by the continuity equation was 1.7 cm2. There was no dilatation of the ascending or visualized descending thoracic aorta and no pericardial effusion, but there was a striking dilatation of the main pulmonary artery at and above the pulmonic valve (Figure 1). The greatest diameter of the main pulmonary artery was 4.6 cm, measured in the parasternal short-axis dimension from the third intercostal space with the patient supine. A split-screen comparison of the main pulmonary artery diameter compared with the ascending aorta diameter obviated the impression (Figure 2). Color Doppler was remarkable for classic and chaotic yin-yang red-blue swirl, characteristic of aneurysm. There appeared to be only physiologic pulmonary insufficiency with a mean gradient across the pulmonary valve of 5 mm Hg, peak velocity of 1.7 m/s, and peak gradient of 10 mm Hg.
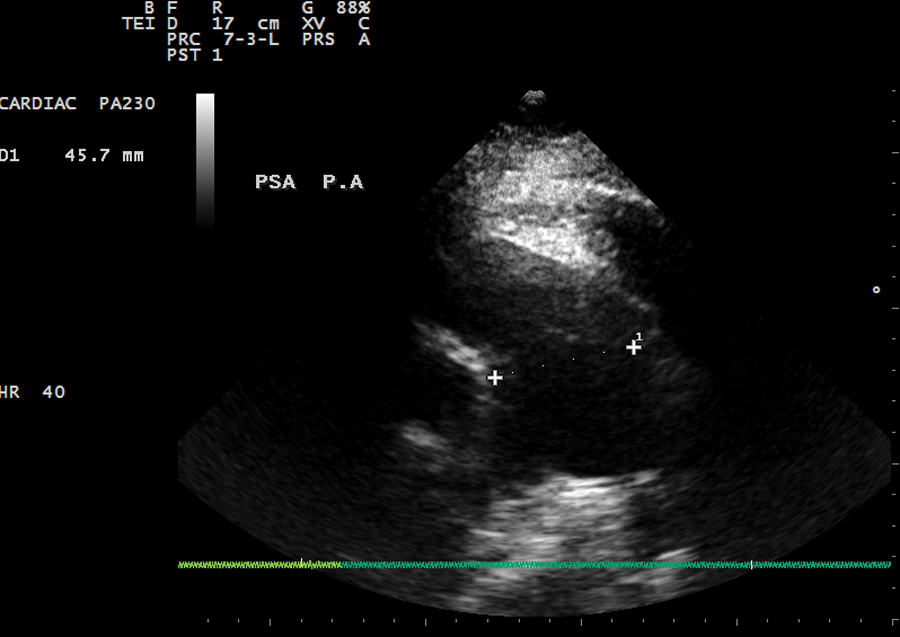
Two-dimensional echocardiogram showing dilation of the main pulmonary artery (45.7 mm) at and above the pulmonic valve.
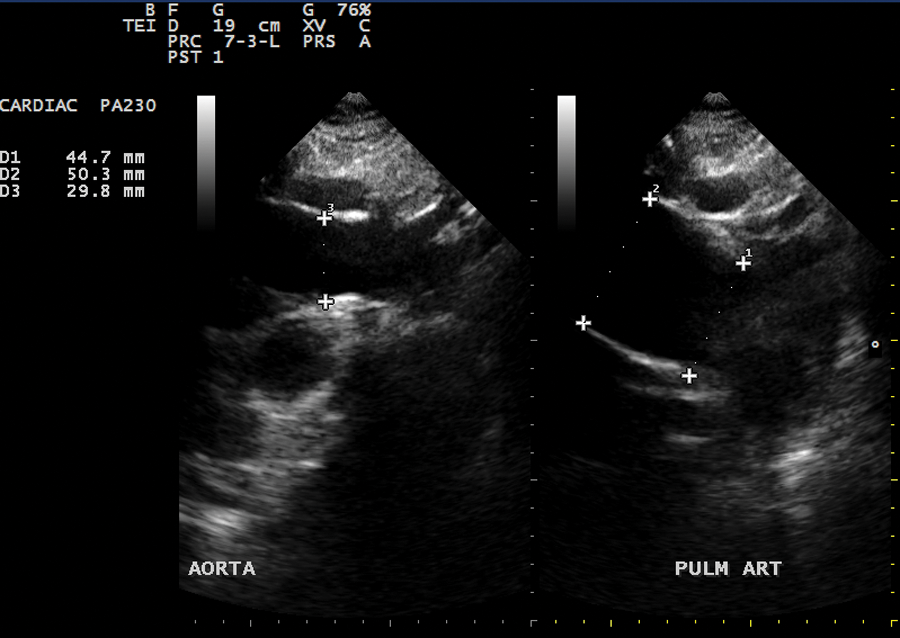
Two-dimensional split screen echocardiogram comparing the diameter of the ascending thoracic aorta (29.8 mm) to the proximal main pulmonary artery (50.3 mm).
At the recommendation of the interpreting physician, a computed tomographic angiogram (CTA) (Figure 3) was ordered, which confirmed a 4.5-cm main pulmonary artery aneurysm. Three-dimensional reconstruction (Figure 4) clearly demonstrated marked dilatation of the main pulmonary artery with normal narrowing into the right and left pulmonary arteries.
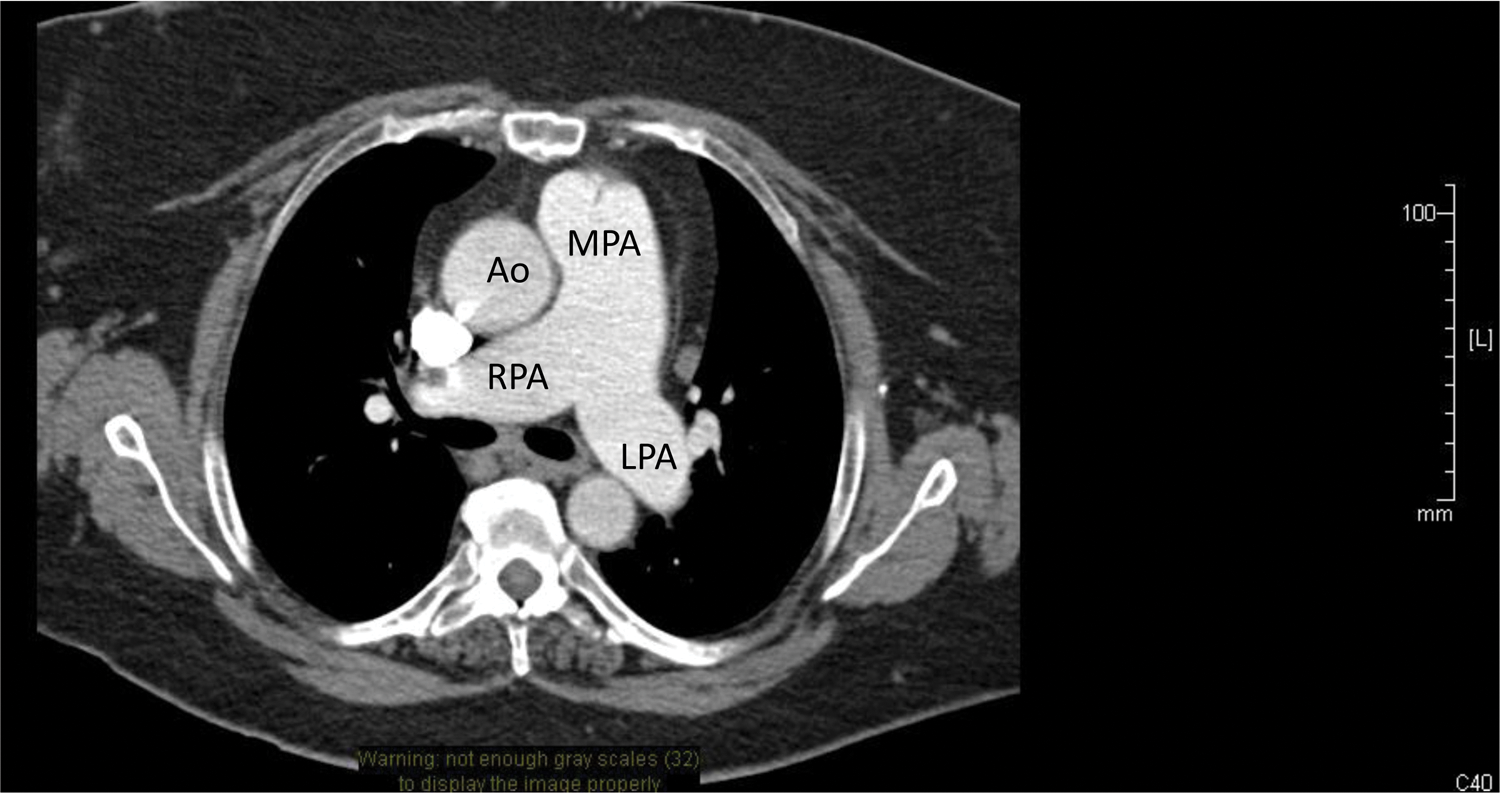
Cardiac computed tomographic angiogram. Ao, ascending aorta; MPA, main pulmonary artery; RPA, right pulmonary artery; LPA, left pulmonary artery.

Three-dimensional reconstruction of a computed tomographic angiogram. Ao, aorta; MPA, main pulmonary artery.
Discussion
This case demonstrates a rare and highly unexpected finding of an aneurysm of the main pulmonary artery. Few citations of main pulmonary artery aneurysm were found in a general literature search, and no citations at all were found dating back to 1985 in the Journal of the American Society of Echocardiography. The performing sonographer followed a strict standardized protocol that allowed a highly atypical and potentially life-threatening main pulmonary artery aneurysm to “fall out” of the normal template. It is easy to pay scant attention to the structure and function of the normally low-pressure and low-resistance right heart, instead focusing on the systemic and high-pressure left side. This case is interesting in that the main pulmonary artery aneurysm was not described at any time after the patient’s aortic valve replacement. At least one upper chest and shoulder x-ray in 2004 for shoulder injury did not show any unusual cardiac or hilar silhouette. The patient did experience shortness of breath but had not been diagnosed with pulmonary hypertension, lung disease, or any autoimmune disorder. The patient is morbidly obese, further clouding the distinction between conditioning and any clinical manifestation of pulmonary artery aneurysm. The literature does suggest that many patients who develop main, left, or right pulmonary aneurysm develop Behcet disease, an autoimmune disorder that manifests mainly with vision problems, venous thrombosis, and central nervous system dysfunction.3,6,13,14
Mycotic (infected) arterial aneurysm may occur as a result of bacterial infection, especially from intravenous drug use. Mycotic may be something of a misnomer, as the word is more of a morphologic definition than a description of a source cause of developing an arterial aneurysm.10–12 Pulmonary arterial wall stress may occur in the main, right, or left pulmonary artery as a reaction to significant pulmonary hypertension or pulmonary embolism. 15 The sonographer and interpreting clinician should evaluate for the presence of pulmonary aneurysm with or without significant pulmonary hypertension when Doppler-derived right-sided pressures exceed 40 mm Hg. Guidelines and standards published by the American Society of Echocardiography suggest that the distal diameter of the main pulmonary artery should not exceed 3.3 cm in diameter. 16
Most community adult and even pediatric cardiologists have not encountered aneurysm of the main pulmonary artery, which normally should not exceed 3.3 cm.8,16 From a technical standpoint, 2D transthoracic sonographic imaging of the main pulmonary artery17,18 is accomplished by optimizing lateral resolution, which resolves the minimum separation of two points aligned along a direction perpendicular (objects that are side by side) to the sonographic beam, as opposed to axial resolution, which defines objects in a plane above and below one another. Consequently, it is not uncommon for there to be complete ultrasonic dropout of images on a transthoracic study where lateral resolution is suboptimal—for example, in the interrogation of the main pulmonary artery in the parasternal short-axis view or the lateral wall of the left ventricle from the apical four-chamber view. Several experienced cardiac surgeon(s) who reviewed this particular case suggested a wait-and-see approach favoring monitoring, preload and afterload management, and regular surveillance transthoracic echocardiograms. Surgical resection in otherwise asymptomatic patients is not recommended, unless the aneurysm grows to a giant size.11,19–21
Conclusion
Aneurysm of the main pulmonary artery is a rare finding during routine transthoracic echocardiograms. This 2D study demonstrated a 4.4- to 4.5-cm main pulmonary artery aneurysm in a patient without demonstrable pulmonary stenosis or pulmonary hypertension. Normal diameter of the main pulmonary artery should not exceed 3.3 cm. Computed tomographic angiography with 3D reconstruction confirmed the transthoracic echocardiographic finding. This case underscores the importance of recognizing significant pathology in the right heart.
Footnotes
Acknowledgements
The author acknowledges the encouragement and guidance of Dr David J. Amalfitano, DO, FACOS, FCCP, in the preparation and writing of this manuscript.
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author received no financial support for the research, authorship, and/or publication of this article.