
Abstract
Behçet’s disease is a chronic inflammatory disorder that often presents with a triad of uveitis, oral aphthous ulcers, and genital ulcerations, along with systemic manifestations such as vascular involvement. We report a case of a 36-year-old male with a significant smoking history who presented with recurrent hemoptysis and a progressive cough, leading to the diagnosis of Behçet’s disease. Physical examination and imaging studies revealed aphthous and genital ulcerations, erythematous nodules, and a pulmonary artery aneurysm. Elevated inflammatory markers supported the diagnosis and treatment with methylprednisolone and infliximab resulted in clinical improvement. The management of pulmonary artery aneurysm in Behçet’s disease includes both medical and interventional strategies, with endovascular interventions like coil embolization being crucial for managing life-threatening hemoptysis or aneurysm rupture.
Introduction
Behçet’s disease (BD) is a chronic, relapsing inflammatory disorder that primarily affects genetically predisposed individuals. First described by Hulusi Behcet in 1937, it is characterized by a triad of uveitis, oral aphthous, and genital ulceration, along with less-frequent systemic manifestations, including gastrointestinal and central nervous system infections. Onset typically occurs between the second and third decades of life, with more severe and multiorgan involvement in those who develop the disease at a younger age. BD is most prevalent in Turkey and the Middle East, earning the nickname “Silk Route Disease.” Vascular manifestations are common, including superficial thrombophlebitis, vein thrombosis, and arteritis, which can lead to occlusive-thrombotic and aneurysmal processes affecting major arteries like the aorta and pulmonary artery, potentially causing heart attacks, hemorrhagic conditions, and pulmonary arterial abnormalities.1,2
We report a case for a 36-year-old male with a significant smoking history presented with recurrent hemoptysis and a progressive cough, leading to the diagnosis of BD after further investigations revealed a pulmonary aneurysm and increased inflammatory markers. The patient was treated with methylprednisolone and infliximab, showing clinical improvement, and was subsequently referred for coil embolization. Follow-up care included education on lifestyle modifications, regular monitoring, and adherence to medication regimens to manage BD and prevent further complications.
Case presentation
A 36-year-old male with a significant history of smoking but no notable prior medical conditions presented to the emergency department of our institution due to recurrent hemoptysis and a progressive cough persisting for 2 months. Upon physical examination, the patient was conscious, oriented, and afebrile, with normal oxygen saturation and stable vital signs. Furthermore, he exhibited aphthous and genital ulcerations, along with multiple tender and erythematous nodules on both upper and lower extremities. Moreover, bilateral decreased air entry was noted.
As a result, further investigations were conducted, including laboratory tests that revealed an increase in inflammatory markers (see Table 1). The chest X-ray demonstrated right-sided hilar nodular infiltration of the lung (as seen in Figure 1), raising suspicion for a lung mass or lobar pneumonia. To accurately determine the underlying cause, additional imaging studies and clinical evaluation were warranted. Consequently, computed tomography (CT) angiography of the chest and neck with intravenous contrast was performed, revealing a saccular aneurysm measuring 3 cm in diameter, arising from the descending branch of the right pulmonary artery. Mural thrombosis was evident, along with a filling defect in the distal segment of the right lower lobe, indicative of a segmental pulmonary aneurysm (see Figure 2). Furthermore, multiple mediastinal and cervical lymph nodes, measuring up to 1 cm, were identified.
Comparative laboratory values on admission day and at discharge day (posttreatment).


Admission chest X-ray demonstrated right-sided hilar nodular infiltration of the lung.
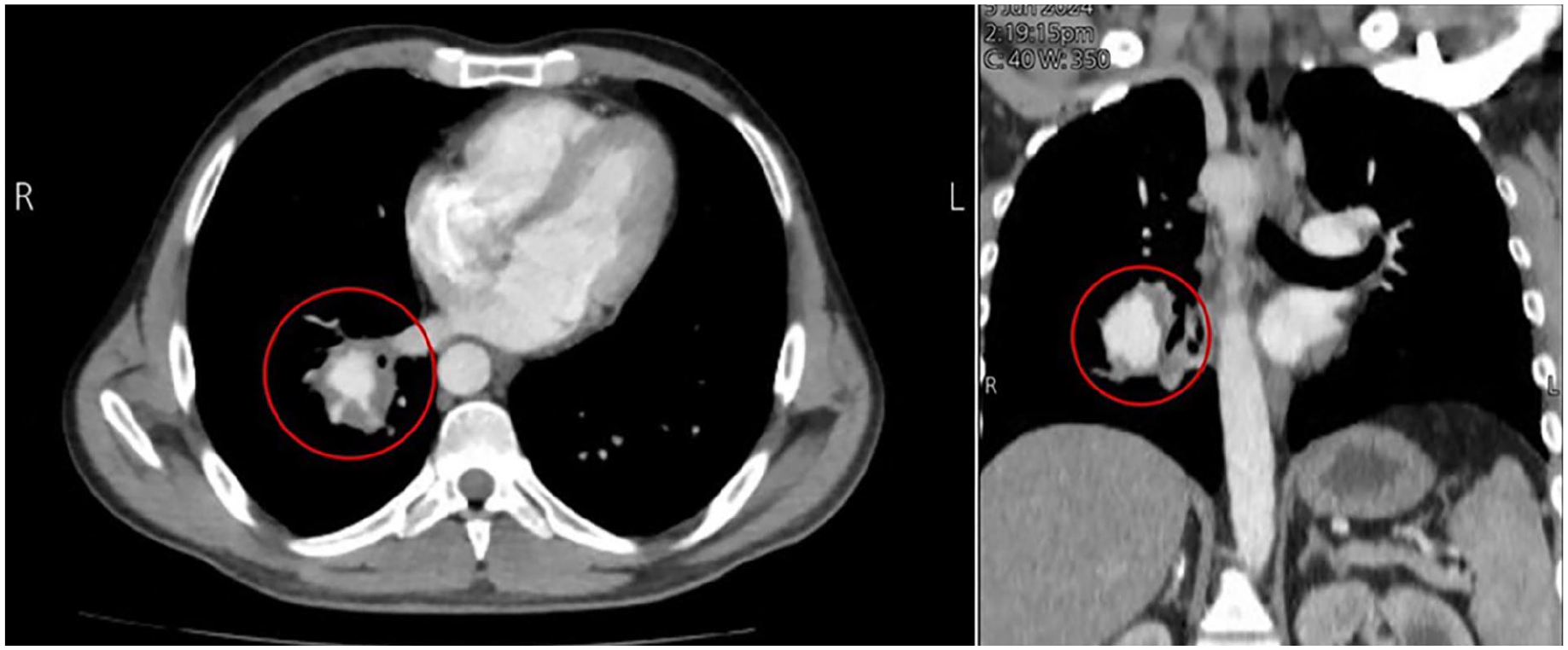
Depicts a saccular aneurysm measuring 3 cm in diameter, originating from the descending branch of the right pulmonary artery (proximal segment of the right lower lobe branch).
Subsequently, the patient was diagnosed with BD based on the International Study Group criteria. The treatment regimen included intravenous methylprednisolone at a dose of 1 mg/kg once daily for 3 days to rapidly reduce inflammation. Additionally, infliximab was administered at a dose of 5 mg/kg on the first day and on day 12 to prevent aneurysm progression. Following the initial treatment, the patient was referred to another hospital for coil embolization of the right descending pulmonary artery aneurysm (PAA).
Over the next few days, the patient showed signs of clinical improvement, with a reduction in hemoptysis and a gradual resolution of cough. Repeat laboratory tests indicated a decrease in inflammatory markers (see Table 1), suggesting a positive response to the treatment. Additionally, imaging studies, including a follow-up chest X-ray and CT scan, demonstrated stabilization of the pulmonary aneurysm without further enlargement or additional complications.
Furthermore, the patient’s aphthous and genital ulcerations, as well as the erythematous nodules on his limbs, began to heal, indicating a systemic response to the immunosuppressive therapy. Regular monitoring and follow-up visits were scheduled to ensure ongoing management of BD and to detect any potential complications early. Moreover, the patient was educated on lifestyle modifications, including smoking cessation, which is crucial for managing BD and preventing further vascular complications. He was also advised to adhere to his medication regimen and attend regular follow-up appointments with both his primary care physician and rheumatologist.
Discussion
BD is a chronic, multisystem inflammatory disorder characterized by recurrent oral and genital ulcers, uveitis, and skin lesions. This disease can affect various organ systems, leading to diverse manifestations, including vascular, gastrointestinal, neurological, and pulmonary complications. 2
Diagnosing BD commonly involves the International Study Group criteria. These criteria stipulate that recurrent oral ulceration must be present, accompanied by at least two additional manifestations: recurrent genital ulceration, eye lesions, skin lesions, or a positive Pathergy Test 3 (see Table 2).
International study group criteria for diagnosing Behçet’s disease. 3

BD can lead to several severe complications. For instance, documented cardiovascular issues, including coronary artery disease and heart valve abnormalities, contribute significantly to morbidity. Moreover, gastrointestinal manifestations, such as ulcerations, may lead to hemorrhage and perforation, sometimes necessitating surgical intervention in severe cases. Additionally, neurological complications, such as meningoencephalitis and cerebral vasculitis, though less common, present significant challenges and are associated with high morbidity and mortality. Furthermore, the most severe complication is vasculitis involving both arteries and veins. Specifically, among these, PAAs are rare but highly serious. They occur in approximately 1%–7% of BD patients and can be life-threatening due to the risk of rupture, which is a major cause of death in these patients. Typically, PAAs in BD present with symptoms such as hemoptysis, dyspnea, and chest pain. The aneurysms can be multiple and bilateral, often leading to severe outcomes if not managed promptly.4–7
PAAs in BD require a comprehensive differential diagnosis, as they can be mistaken for conditions such as infective endocarditis, pulmonary embolism, tuberculosis, and other vasculitides, including Takayasu arteritis and Wegener’s granulomatosis. To accurately diagnose PAAs in BD, various imaging studies are employed. Chest radiography, CT, magnetic resonance angiography, and pulmonary angiography are crucial in identifying the presence, size, and extent of the aneurysms. These imaging techniques provide detailed insights necessary for effective diagnosis and subsequent management. 4
The management of PAAs in BD encompasses both medical and interventional strategies. Medical therapy primarily includes corticosteroids, such as methylprednisolone, to reduce inflammation. Additionally, immunosuppressive agents such as cyclophosphamide, azathioprine, infliximab, and colchicine are employed to prevent aneurysm progression and reduce systemic inflammation. Additionally, endovascular interventions, such as coil embolization or the use of stents and plugs, are utilized to manage life-threatening hemoptysis or aneurysm rupture. These methods typically result in fewer adverse effects compared to surgical options (see Table 3). Surgical interventions, including aneurysmorrhaphy, lobectomy, or pneumonectomy, are considered when medical and endovascular treatments are unsuccessful. However, these procedures carry high risks and are reserved for severe cases.8–10
Provides an overview of the primary treatment options for Behçet’s disease along with their associated side effects.
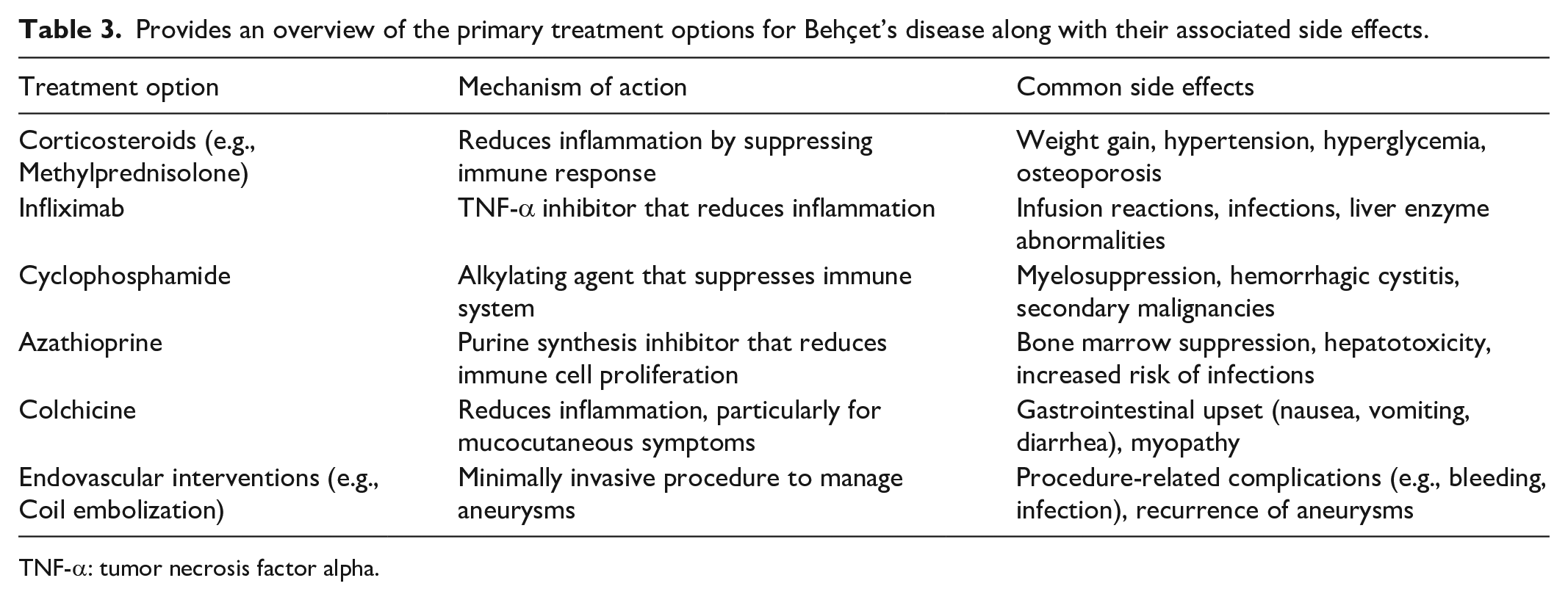
TNF-α: tumor necrosis factor alpha.
The prognosis of PAAs and other severe complications in BD is generally poor due to the high risk of rupture and recurrent aneurysms. However, early diagnosis and aggressive treatment can improve outcomes. The introduction of immunosuppressive therapy has significantly improved survival rates. Nonetheless, long-term prognosis remains guarded, and continuous monitoring is essential to manage relapses and complications. 11
Finally, one of the primary limitations of this case report is the lack of detailed long-term follow-up data. While the initial treatment outcomes showed promising improvements in the patient’s condition, including reduced inflammatory markers and stabilization of the pulmonary aneurysm, we did not have the opportunity to document subsequent follow-up visits. This absence of extended follow-up limits our ability to fully evaluate the long-term efficacy of the treatment regimen and monitor for potential relapses or late complications.
Conclusion
BD is a complex multisystem inflammatory disorder that can lead to severe vascular complications such as PAAs. In this case, we are reporting the necessity of a high index of suspicion for BD in patients presenting with multisystem inflammatory symptoms, particularly in the presence of vascular manifestations. Early diagnosis and aggressive treatment with immunosuppressive therapy and interventional procedures are critical for improving patient outcomes and preventing life-threatening complications. Long-term management and regular follow-up are essential to monitor disease progression and ensure ongoing care.
Footnotes
Acknowledgements
We express our deep gratitude to the medical ward staff for their invaluable support in completing this report.
Author contributions
A.B.O. contributed to patient management and data collection; A.A. drafted the manuscript and was responsible for the overall coordination of the case report; Z.S. assisted in data collection and manuscript revision; A.S. provided critical insights and revisions to the manuscript; O.S. assisted with literature review and manuscript editing; J.K. conducted radiological analysis and interpretation; M.A. supervised the case report and reviewed the manuscript; Y.G. supervised the case report and reviewed the manuscript; All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient Himself for his anonymized information to be published in this article.