
Abstract
The correlation between cryptogenic stroke and patent foramen ovale is high in young patients. Currently, transesophageal echocardiography is the gold standard for detection. However, it is invasive and limits Valsalva maneuvers. This article reviews the diagnostic accuracy of the three modalities: transthoracic echocardiography, transesophageal echocardiography, and transcranial Doppler. The results suggest that transcranial Doppler sonography is an accurate, easily accessible procedure for detecting patent foramen ovale and should be considered an excellent alternative to transthoracic or transesophageal echocardiography. Transesophageal echocardiography is still necessary for patients who require treatment. The combination of transcranial Doppler and transesophageal echocardiography provides the highest level of information regarding the complete diagnosis of patent foramen ovales.
Keywords
Cerebral vascular accident, or stroke, is the second leading cause of death worldwide and a common cause of long-term disability. 1 The incidence worldwide is 258/100,000 persons with wide variations between high- and low-income economies. 2 In the United States, the Centers for Disease Control and Prevention reports stroke affects 795,000 individuals each year, is the fifth leading cause of death, 3 and is the leading cause of long-term disability.3,4
Between 80% and 87% of strokes are classified as ischemic with cardioembolism, large vessel atherosclerotic disease, and small vessel occlusive disease as the most common causes. 5 The category of cryptogenic stroke is used when the stroke is believed to be ischemic, but there is no identifiable cause. 6 Cryptogenic strokes are believed to be caused by emboli when they do not present as a lacunar infarct on imaging, there is a lack of extracranial atherosclerosis causing greater than 50% stenosis, and other embolic risk factors such as intracardiac thrombus, cardiac tumors, or valvular vegetations are not present.6,7 Cryptogenic strokes are believed to comprise 25% to 40% of all embolic strokes. 8
When an embolic source for stroke cannot be clearly identified, atrial septal abnormalities such as atrial septal defects and pulmonary shunts are considered potential causes. An atrial septal defect (ASD) is a defect of the interatrial septum that results in a right-to-left shunt (RLS) across the atrial septum, leading to unoxygenated blood bypassing the lungs and going into the systemic circulation. Patent foramen ovale (PFO) is a common type of ASD, occurring in approximately 30% of adults. 9 Although there is no clear relationship between patient age and the occurrence of cryptogenic stroke, 10 up to 55% of cryptogenic strokes occur in those younger than 45 years compared to 42% of strokes in those older than 45 years. The prevalence of PFO is 55% in younger patients who present with cryptogenic stroke. 11
The foramen ovale allows the shunting of blood from the right atrium (RA) directly into the left atrium (LA) in utero. The foramen should fuse within the first year of life. A PFO typically does not result in an RLS due to the higher left heart pressures, can typically be regarded as a normal structural variant, and can be asymptomatic.12,13 However, during a cough or a Valsalva maneuver, right heart pressures can exceed the left pressures, allowing an RLS to occur. 12 Small shunts are not regarded as severe and do not receive treatment. Serious concern is given to larger shunts because of the risk of thrombi passage and subsequent ischemic stroke. Detection of these larger PFOs is important, especially in young patients experiencing stroke-like symptoms, because it suggests that a large RLS with thrombi passage could be occurring.
Patent Foramen Ovale Detection by Sonography
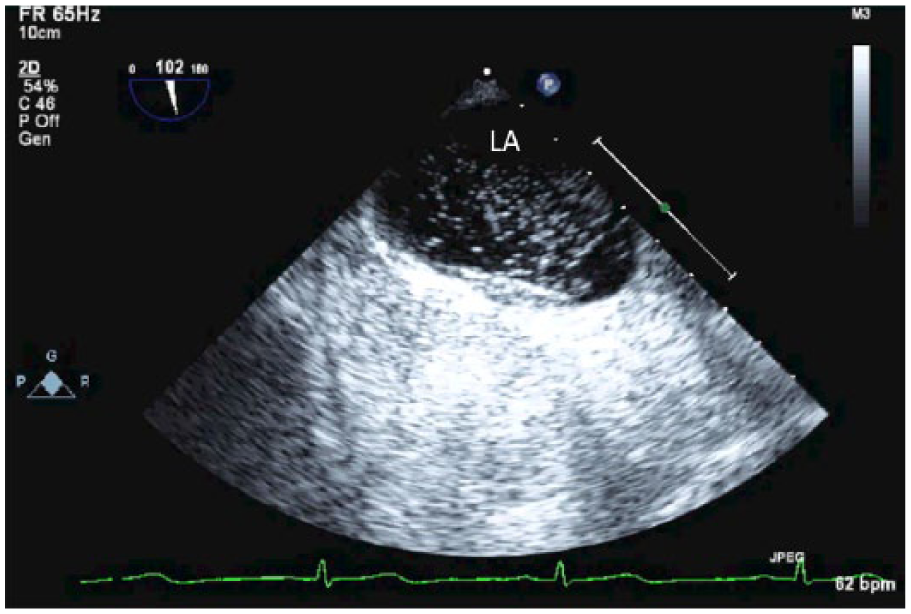
Three sonographic imaging techniques can be used to assess for PFO: transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), and transcranial Doppler (TCD). In a standard TTE examination, a PFO may appear by 2D imaging alone as a noncontinuous interatrial septum (Figure 1). Color Doppler can be used to assess for a color jet flowing into the LA from the interatrial septum, indicating an RLS. This approach is only successful at identifying less than 5% of patients with PFO. 12 Gray-scale and color Doppler cannot be the only indicators for a RLS in TTE, and therefore contrast injection with Valsalva maneuver is required (Figure 2).
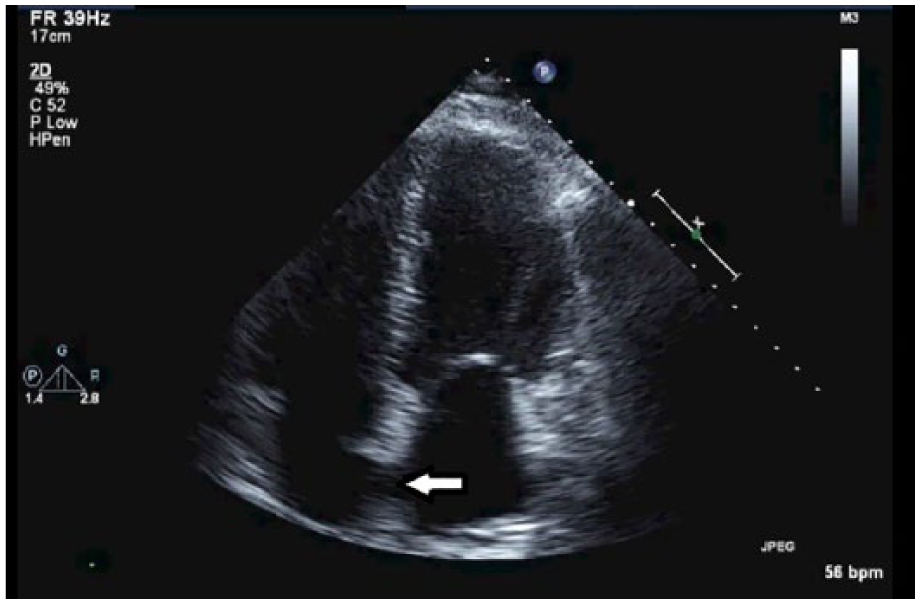
Gray-scale transthoracic echocardiography with patent foramen ovale (PFO). Arrow indicates PFO.
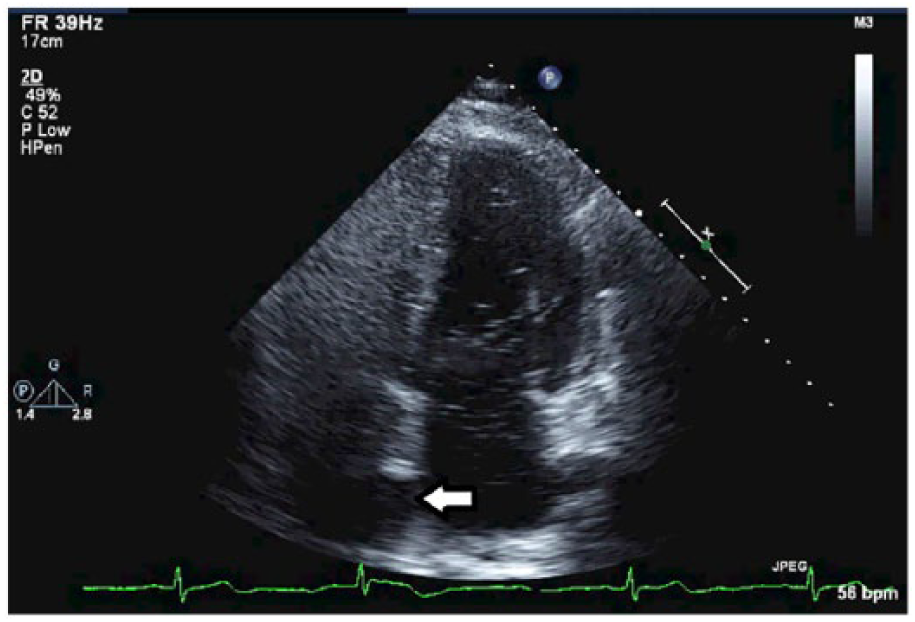
Transthoracic echocardiography bubble study with patent foramen ovale (PFO). Arrow indicates PFO.
Transesophageal examination with color Doppler is successful at identifying PFO approximately 5% to 10% of the time. 12 During a TEE examination, the PFO will appear as a hypoechoic foramen in the interatrial septum (Figure 3). Using contrast agents and the Valsalva maneuver improves the chances of PFO detection 12 in TEE up to 25% (Figures 4 and 5). The transcranial Doppler examination relies on the visualization of the middle cerebral artery (MCA) with color and spectral Doppler from the transtemporal window (Figure 6). The administration of a contrast agent and the Valsalva maneuvers are required in order for TCD to diagnose a PFO; without the latter two, a PFO cannot be diagnosed on TCD.
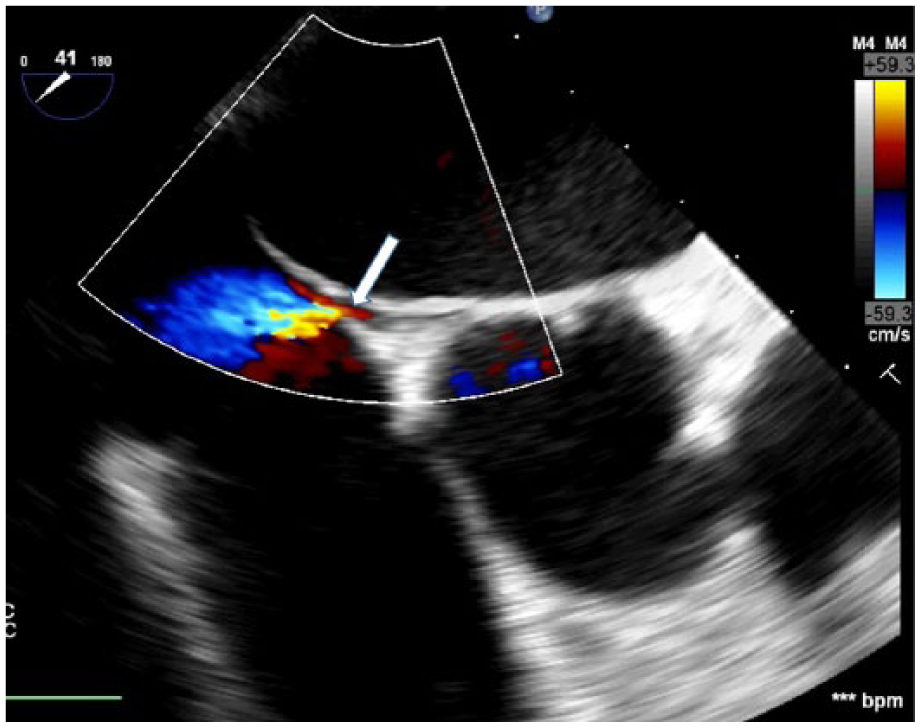
Transesophageal echocardiography with color Doppler demonstrates patent foramen ovale (PFO) flap. Arrow indicates flow beneath the PFO flap.
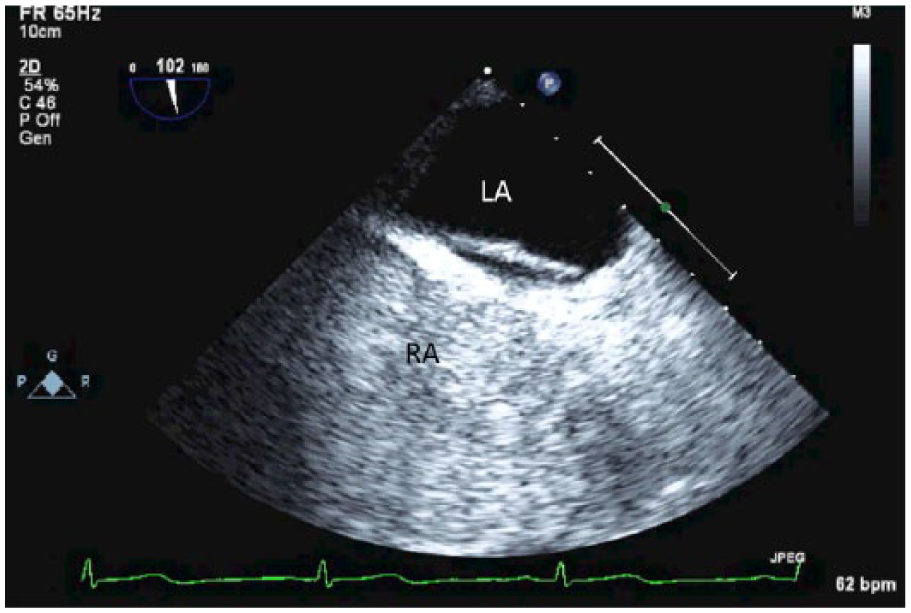
Patent foramen ovale diagnosed on transesophageal echocardiography with micro-bubbles without Valsalva. Bubbles are not entering the left atrium.
Patent foramen ovale on transesophageal echocardiography with micro-bubbles with Valsalva. Right atrium to left atrium shunting of microbubbles is demonstrated.
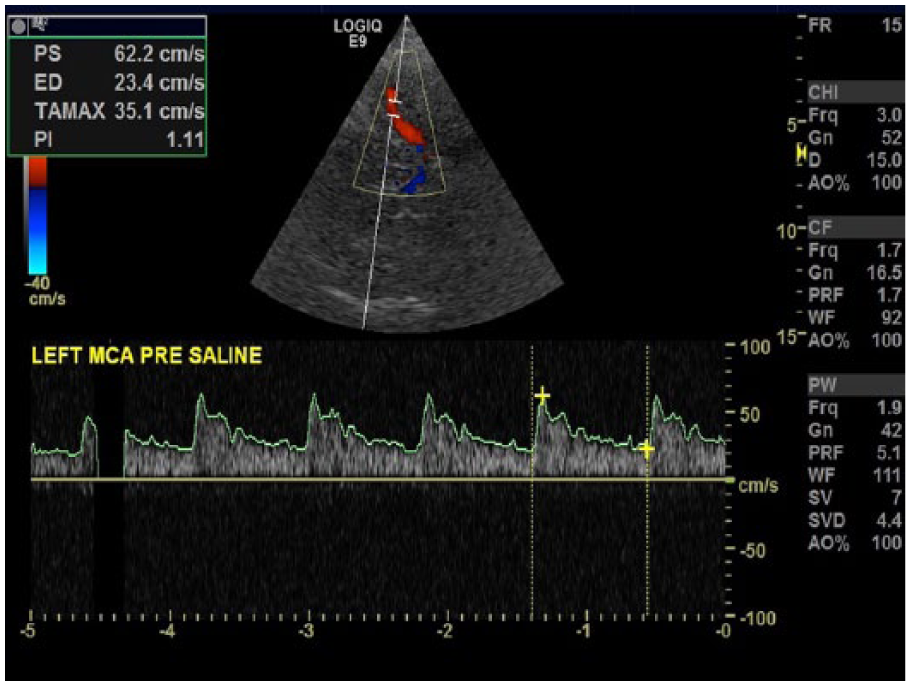
Middle cerebral artery precontrast injection. Image courtesy of Patrick Washko, BSRT, RDMS, RVT, FSVU.
All three of these sonographic techniques require the use of contrast agents to detect an RLS. Mixtures of saline and air are rapidly mixed between two syringes to agitate the solution, creating bubbles, which are then injected into an intravenous site. These contrast mixtures produce micro-bubbles, which are brightly displayed on the screen.
Following the injection of the contrast agent, patients should perform a Valsalva maneuver. Patients should be educated on how to perform Valsalva before beginning any examination. To confirm the effectiveness of a Valsalva maneuver in TTE or TEE, a bulging of the interatrial septum into the LA or collapse of the RA should be observed. 14 Appropriate Valsalva during TCD can be verified by a 25% decrease of the MCA flow velocity. 14 The maneuver should be repeated at least three times with each examination and should be held for a minimum five seconds. 14 Valsalva is important in detecting PFO because most defects require the atrial pressure shift to shunt the micro-bubbles. If patients cannot perform Valsalva, the study cannot be deemed effective.
During TTE and TEE, the micro-bubbles appear as round bright reflectors inside the heart chambers. An RLS is diagnosed when one or more micro-bubbles are seen passing directly into the LA within three cardiac cycles following the appearance of micro-bubbles in the RA.14,15 The Valsalva maneuver is then performed to increase pressure, which, if a PFO is present, will cause the bubbles to shunt from the right to the left side of the heart. The number of micro-bubbles in the LA determines the grading of the PFO. A small shunt consists of less than 10 micro-bubbles in the LA, medium when over 10 micro-bubbles are present, and large when the LA is completely filled with micro-bubbles. 15 During TCD, if a right to left shunt is present, the micro-bubbles appear as bright lines on the spectral Doppler display and are referred to as high-intensity transient signals (HITS) (Figures 7 and 8). 13 The HITS are expected to appear within 25 seconds after injection and within approximately 25 seconds after the Valsalva maneuver. 13 Physicians count the number of HITS seen crossing the shunt to grade the shunt severity. Grade 0 indicates no HITS, grade 1 is 1 to 10 HITS, grade 2 is 11 to 30 HITS, grade 3 is 31 to 100 HITS, grade 4 is 101 to 300 HITS, and grade 5 is over 300 HITS or uncountable (Figure 9). 16

Middle cerebral artery postcontrast injection demonstrating bright echogenic high-intensity transient signals in the Doppler spectral display (arrow). Image courtesy of Patrick Washko, BSRT, RDMS, RVT, FSVU.
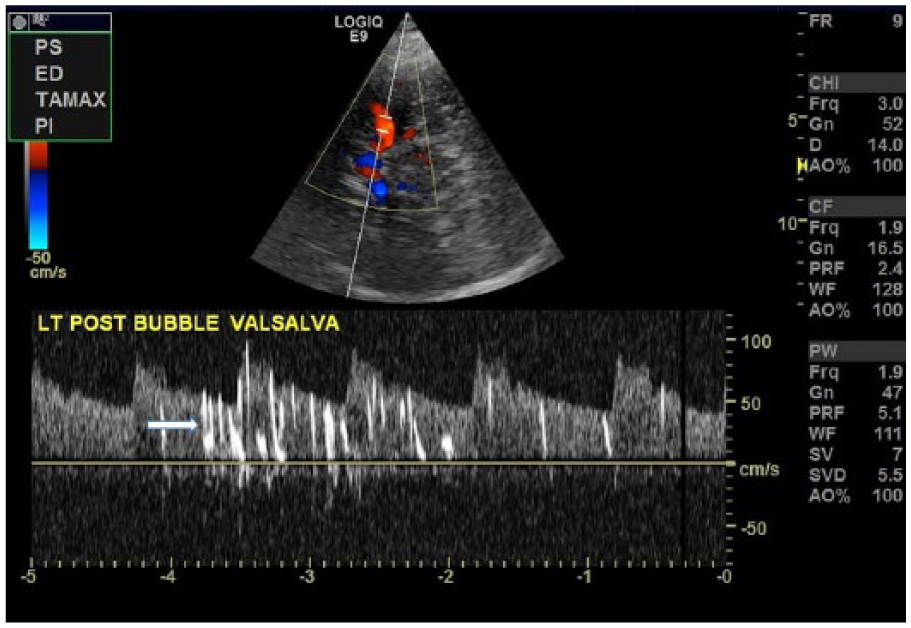
Middle cerebral artery postcontrast injection with Valsalva maneuver demonstrating high-intensity transient signals in the Doppler spectral display (arrow). Image courtesy of Patrick Washko, BSRT, RDMS, RVT, FSVU.
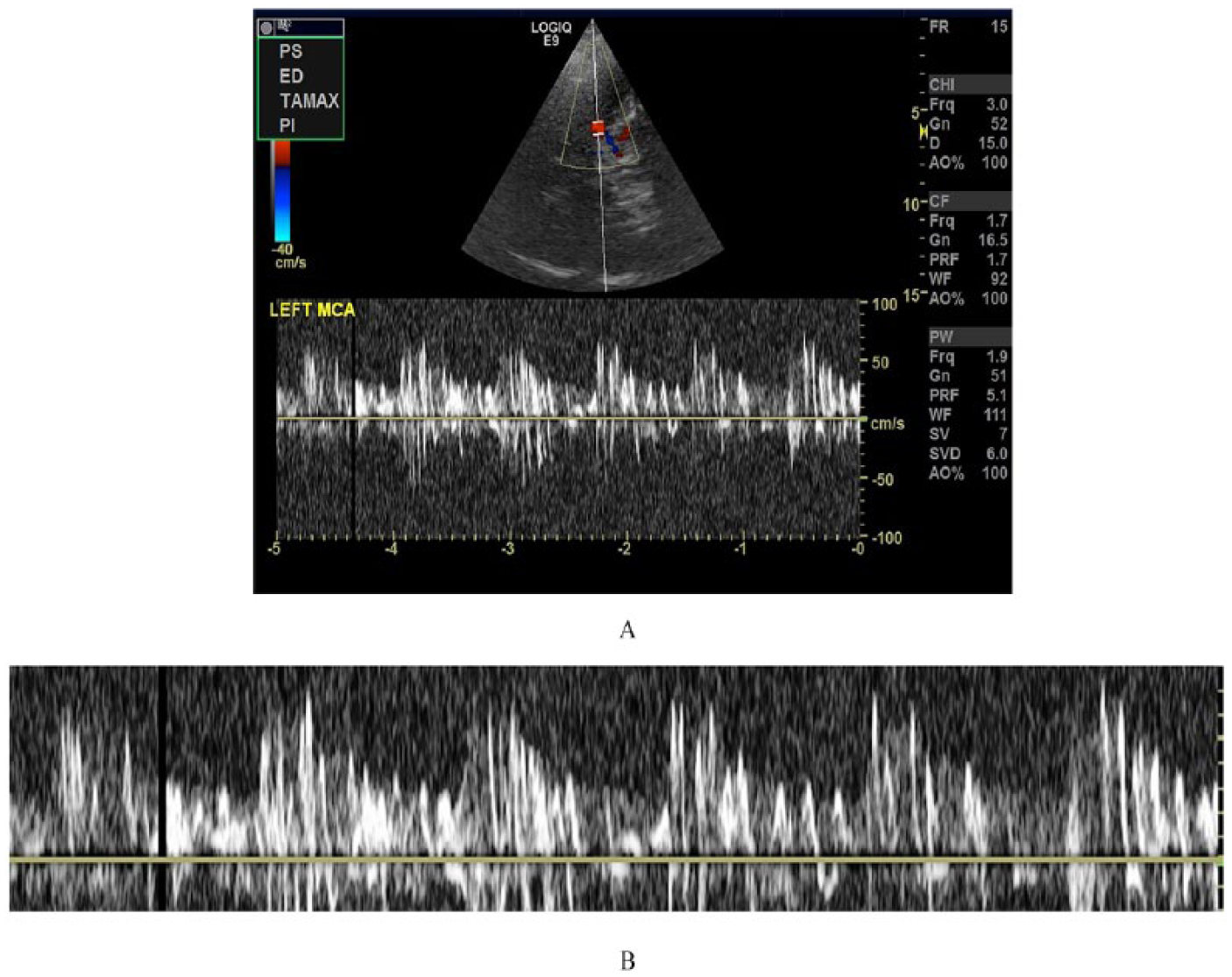
(A) Middle cerebral artery postcontrast injection demonstrating multiple high-intensity transient signals (HITS). (B) Magnified Doppler spectral display demonstrating multiple HITS. Image courtesy of Patrick Washko, BSRT, RDMS, RVT, FSVU.
Diagnostic Accuracy
Transthoracic echocardiography17–20 has reported sensitivities ranging from 32% to 100% and specificities that range from 55% to 97% (Table 1). False negatives are of greatest concern for TTE examinations because they are typically the first modality of choice when a screening for a PFO. False-negative17–20 findings ranged from 18% to 43% while false positives were low, ranging from 5% to 8%. Transthoracic echo accuracy improves as the shunt size increases.15,17–20 Souteyrand et al. 15 showed that TTE missed 71% of small shunts detected by TCD but only missed 21% of large shunts. Most of the positive TTE findings in the studies reviewed were on medium to large shunts.15,17–20
Sensitivity and Specificity Rates of Transthoracic Echocardiography.

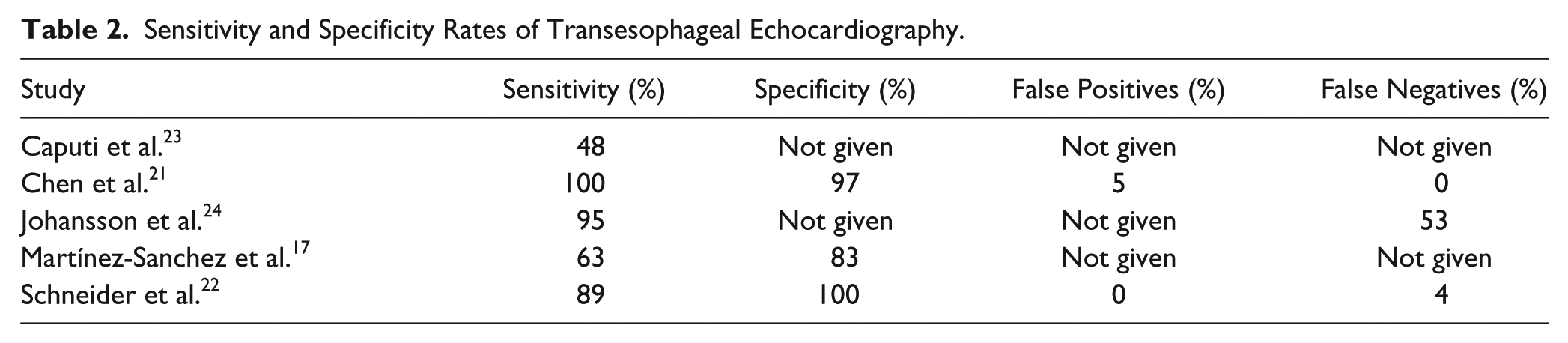
Transesophageal echocardiography has a wider range of sensitivity and specificity17,21–24 as compared to TTE, with sensitivities ranging from 48% to 100% and specificities from 83% to 100%. False-negative findings22,24,25 range from 4% to 53%, with positive predictive values (PPVs)17,22 ranging between 93% and 100% (Table 2). Transesophageal echocardiography accuracy has been shown to increase as the size of the RLS increases.15,16,23 Larger RLS results in greater sensitivity,15,16,23 and smaller shunts lead to more false-negative findings.14,16 Transesophageal echocardiography requires sedation, which may be the underlying cause of the low sensitivity and high percentage of false-negative findings.15,17,20,22,23 Sedation diminishes the Valsalva maneuver and thus does not allow for the change in pressures needed to shunt the micro-bubbles.15,23 Another limitation of TEE is the complex structure of the PFO in the atrial septum. 23 If 3D technologies are not used, the PFO requires imaging in two different planes (midesophageal four chamber and bicaval) to acquire an accurate measurement. 23 This limitation can affect PFO quantification and closure treatments.
Sensitivity and Specificity Rates of Transesophageal Echocardiography.
Transcranial Doppler has reported sensitivities15,18,20,26–31 ranging from 91% to 100% and specificities18,20,23,26,29–31 ranging from 78% to 100%. Transcranial Doppler has a narrower range of false negatives in studies compared to TTE or TEE,15,18,20,23,26–31 with ranges from 0% to 13%. Transcranial Doppler has a PPV14,20 range of 98% to 100%, with the highest PPV occurring when the HITS occur in under nine seconds. 14 False-positive results may be seen if intrapulmonary shunts are present22,30 or when there is a prolonged timeframe for evaluating HITS. 30 If the suggested timeframe for cardiac shunting (7–27 seconds) is used, false positives due to intrapulmonary shunts should not occur.13,17,23,27,28
The accuracy of PFO detection by TCD increases as the shunt size increases.15,16,23 Compared to TTE or TEE, transcranial Doppler is accurate at detecting medium and large shunts 16 but is the most accurate technique 15 for imaging small shunts. Because transcranial Doppler does not visualize the heart, exact anatomical information about the shunt is not obtained. In addition, variations in cerebral arterial anatomy and poor transtemporal windows can limit or prohibit obtaining a spectral tracing. 15 Unilateral versus bilateral readings can affect TCD results, and timing differences can make comparisons between studies difficult. 20
Discussion
Based on the review of this literature, TCD has the highest sensitivities15,18,20,23,26,27,30 ranging between 91% and 100%, and the majority of studies reviewed had sensitivities of 95% or above.15,18,23,27,31 The TCD specificity rates ranged between 78% and 100%, and with the exception of Caputi et al., 23 who reported 78%, the remaining studies10,15,19,23,26–31 reviewed all reported specificities above 90% (Table 3). The sensitivities for TEE range from 48% to 100% and TTE from 32% to 100%, a much wider range of findings when compared to TCD.15,17–24 The specificities rates for TTE17–20 and TEE also had wider ranges of findings: 55% to 97% for TTE and 83% to 100% for TEE.17,21–24 Although the ranges for specificities appear to be narrower for TTE than TCD, four studies with TTE studies reported specificities,17–20 while seven TCD studies reported specificities, with most of those being 90% or higher.11,18,20,23,29–31 Therefore, it appears that TCD has the narrower range of specificities and is probably more consistently able to detect normalcy. More research comparing TEE to TCD should be done to determine which one is more specific.
Sensitivity and Specificity Rates of Transcranial Doppler.

Transcranial Doppler identifies a high number of positive examinations in studies that were originally found to be negative on TEE.14,16,22 Around 7% to 27% of TEE examinations are found to be false negatives that are later identified as positive on TCD. 14 Martínez-Sanchez et al. 17 found that TCD detected PFOs in twice as many patients compared to TTE and in 25% more cases than with TEE. Tobe et al. 16 demonstrated that 15% of positive PFOs identified by TCD were missed on TEE, even in cases of high-grade shunts.
Transthoracic echo was shown to have the highest rates of false negatives compared to TCD and TEE.18,20 Likewise, the negative predictive values of TTE and TEE indicated that these modalities cannot confidently rule out PFOs, even if the examination is negative. 17 Martínez-Sanchez et al. 17 state that due to the high number of false negatives on TTE and TEE, TCD is the best modality to detect PFOs. Although there is thought that false negatives in TEE are related to poor Valsalva maneuver,17,20,22 Caputi et al. 23 found that even without performing Valsalva, TCD still yielded higher accuracy than TEE.
A suggestion has been made to replace TTE with TCD for initial screening for PFOs because it is a highly sensitive, noninvasive, and portable, and it allows for optimal Valsalva.14,17,25–29 Transcranial Doppler proves to be a superior screening method than TTE or TEE for PFO, especially in patients younger than 55 years who are experiencing cryptogenic stroke.14,17,25,28,29
Due to the anatomical limitations of TCD and the invasiveness of TEE, most research considers TCD and TEE as complementary examinations to one another.17,23,27,28 Therefore, most studies suggest that the combination of TCD and TEE should be considered the “gold standard” in diagnosing PFOs.13,15,19,23,27,28 Overall, 6 of 14 authors suggested TCD to be the gold standard in diagnosing PFOs, while 8 of 14 authors suggested the combination of TCD and TEE.15–27 Transesophageal echocardiography should follow up large or severe PFOs detected by TCD that are subject for closure treatments. The highest accuracy in diagnosing PFOs is found when the two are used in combination.17,23,27,28
The results of this review may suggest an alternate protocol for ordering examinations for PFO detection. Figure 10 displays the suggested protocol. Health care professionals could use this protocol to diagnose PFOs more accurately without ordering unnecessary examinations. Future studies should focus on the accuracy in quantification of PFOs. Many studies use different scales for counting micro-bubbles or HITS. A gold standard scale could be set for quantifying PFOs. Likewise, many methods and equipment are used for TCD examinations. Future research could focus on the efficacy of different TCD protocols and create a standard protocol that is suggested for detecting PFOs.
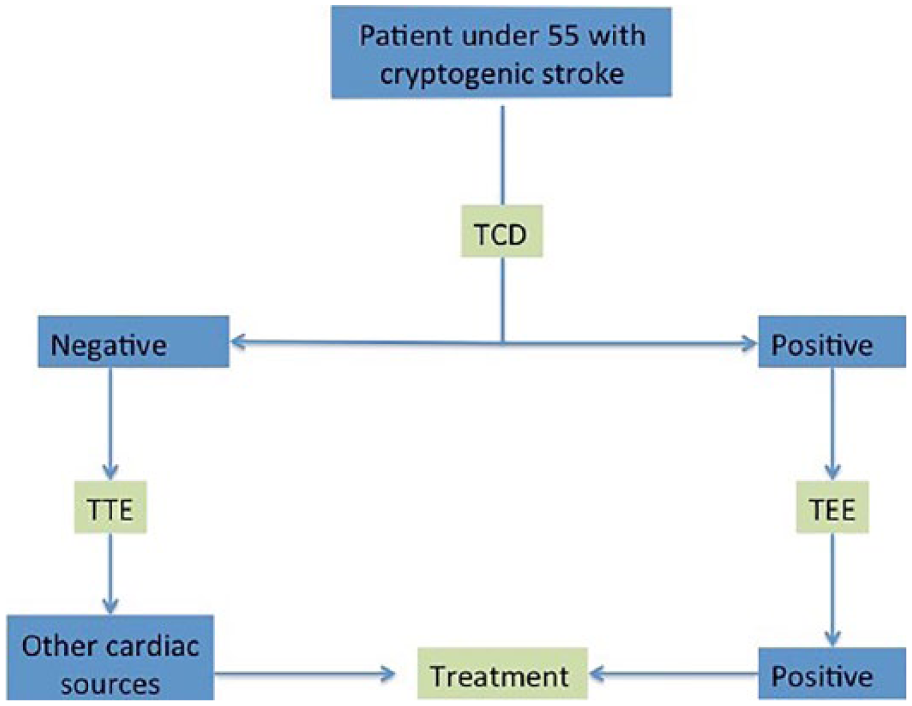
Suggested protocol for the diagnosis of PFOs in patients presenting with cryptogenic stroke. TCD, transcranial Doppler; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
Conclusion
For patients younger than age 55 years who are experiencing cryptogenic stroke, accurate detection of the origin is essential. Because of a high prevalence of PFO in this patient population, a quick reliable method for detecting them is necessary. Transcranial Doppler is an accurate method for detecting PFOs, and more research should be conducted regarding its potential as a primary screening modality. Transesophageal echocardiography is still needed for patients undergoing closure treatments to analyze the anatomy of the defect. Future studies should focus on creating a standard protocol in order for TCD to become the most widely used initial screening examination in patients with cryptogenic stroke.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.