
Abstract
Non-Hodgkin lymphoma requires an early diagnosis for optimal survival rates. If a diagnosis and treatment are too late, the malignancy has the probability of spreading to extranodal regions. A diagnosis of non-Hodgkin lymphoma may present itself unexpectedly to the young adult patient, as well as the examining sonographer. With a comparable case and images, this case study can aid sonographers, radiographers, and radiologists in making an accurate diagnosis of this malignancy for the most favorable patient treatment and outcome.
Non-Hodgkin lymphoma is the fifth most common cancer in the United States and increases in incidence with age. Only 2.4 cases out of every 100,000 occur in 20- to 24-year-old individuals. 1 Although sonography is not usually considered a diagnostic tool in most cases of non-Hodgkin lymphoma, the use of the modality in the following case was important to the sequence of patient diagnosis and treatment.
Case Report
A woman in her early 20s presented to her physician with a palpable neck lump in the left supraclavicular region. She reported no history of illness or other clinical complaints. The physician ordered a thyroid sonogram, which showed the right lobe of the thyroid to be of homogeneous echogenicity, measuring 4.0 × 0.9 × 1.6 cm. The left lobe demonstrated two small cysts, the largest in the mid pole region measuring 7 × 3 × 7 mm. The left lobe measured 4.2 × 0.7 × 1.4 cm. The isthmus measured 2.3 mm in diameter (Figure 1).
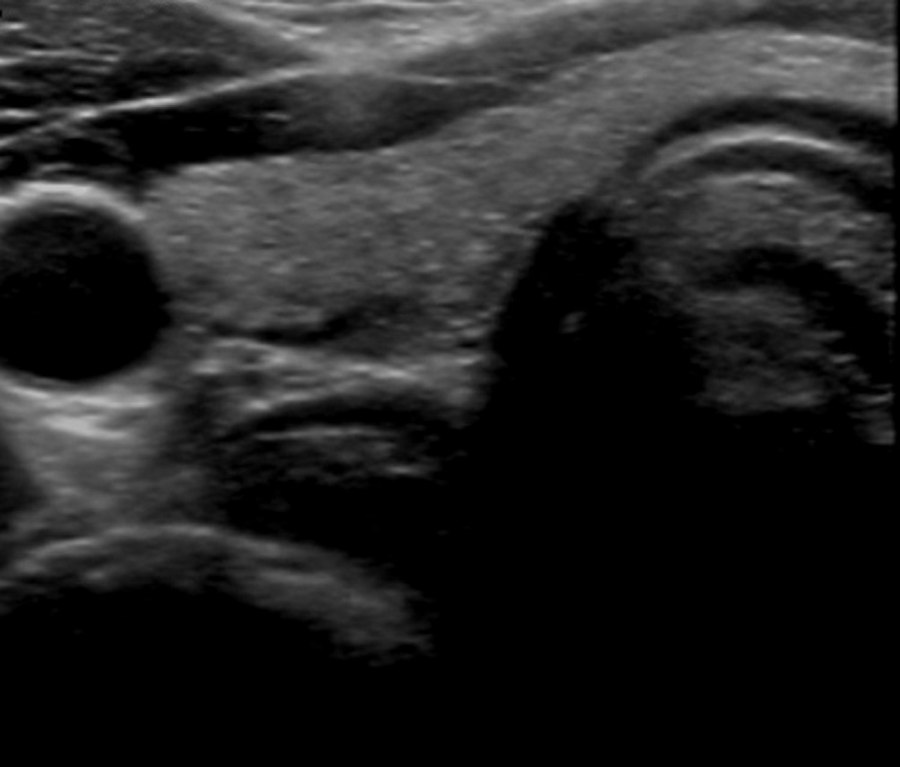
Right lobe of the thyroid demonstrating homogeneity. The thyroid was unremarkable except for two small cysts in the left lobe.
After scanning the thyroid, the sonographer palpated and imaged the lump just superior to the clavicle and left of midline. A solid, heterogeneous mass with smooth margins was seen (Figure 2). The ovoid-shaped mass measured 2.5 × 3.5 × 1.7 cm in diameter. There was moderate hypervascularity in the central portion of the mass (Figure 3), indicating the strong possibility of it being a condition of a lymph node. The mass was bordered posteriorly by the left subclavian artery and medially by the left internal jugular vein (IJV).
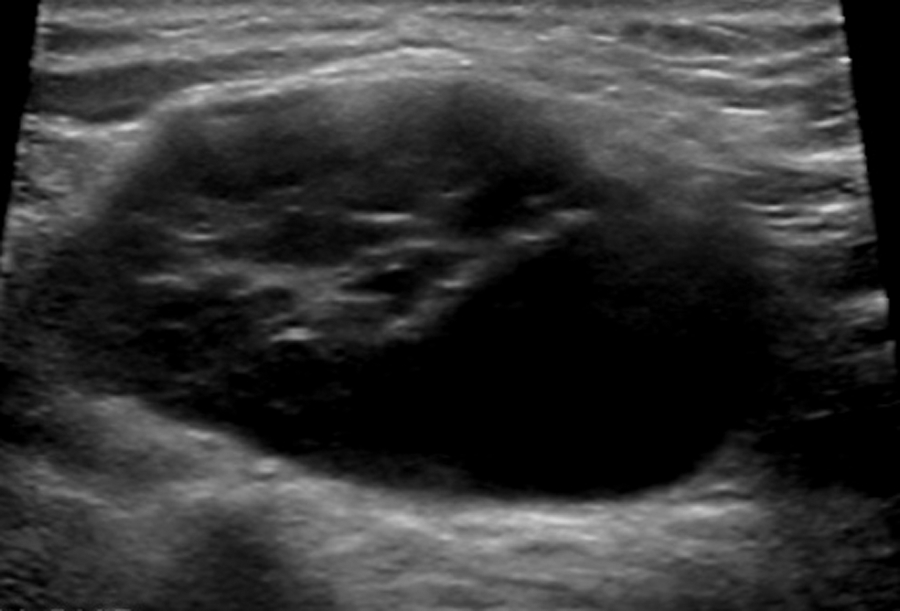
The suspicious mass demonstrating smooth margins and heterogeneity was located superior to the left clavicle. The mass measured 2.5 × 3.5 × 1.7 cm.
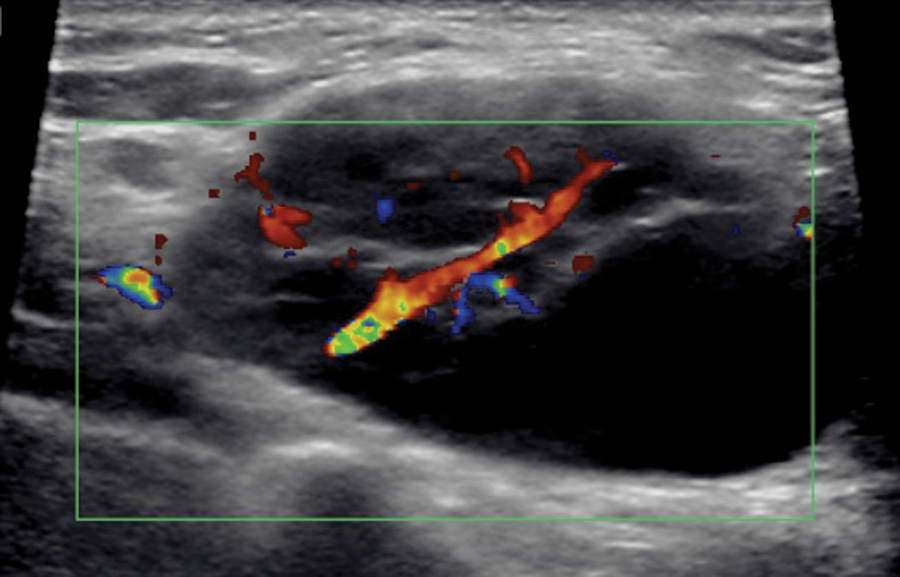
Using color Doppler, the suspicious mass appeared largely vascular, indicative of a lymph node.
Based on the sonographic images, a differential diagnosis of a malignant neoplasm versus reactive lymphadenopathy was made. The recommendation was made for a follow-up computed tomography (CT) scan of the patient’s neck and chest and an ultrasound-guided biopsy.
A contrast-enhanced CT scan demonstrated the supraclavicular ovoid mass with the same solid appearance that resembled a pathologically enlarged lymph node (Figure 4). The mass measured 2.1 × 3.7 cm in anterior-posterior (AP) and transverse diameter. The scan also demonstrated multiple pathologically enlarged lymph nodes located medially on the left at the base of the neck as well as in the medial portion of the axilla. Several of these measured over 1.5 cm in diameter. The right subclavicular area demonstrated at least two enlarged lymph nodes that measured 2.1 × 1.9 cm and 2.0 × 1.6 cm in AP and transverse planes. Small, benign lymph nodes measuring less than 1 cm were visualized in the mid and upper portions of the neck. Limited imaging of the upper abdomen revealed a normal-size spleen.
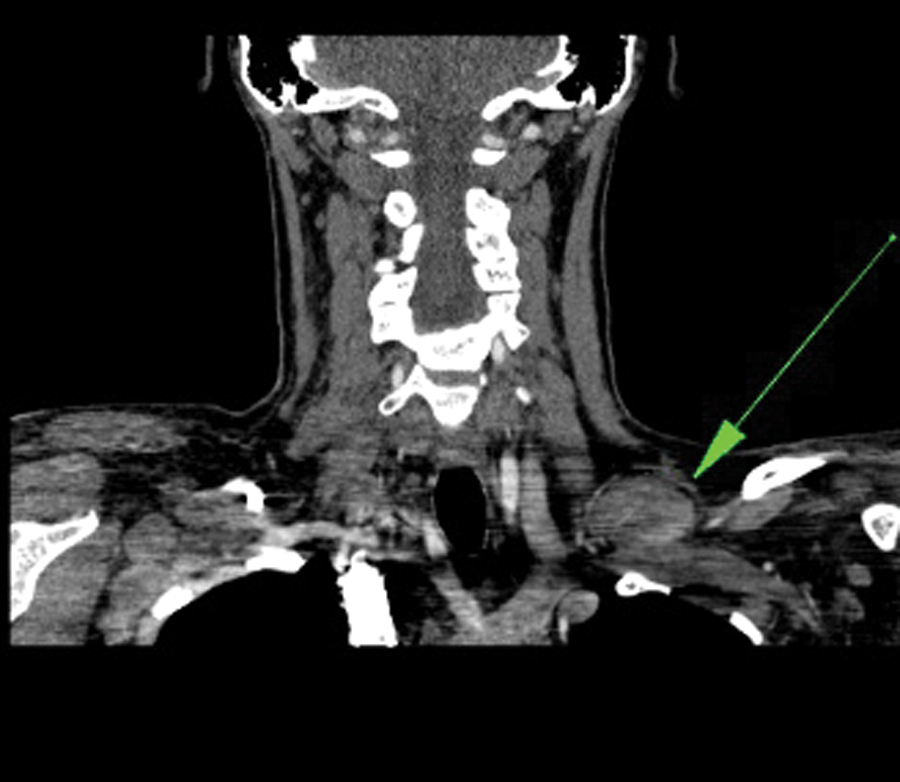
Computed tomography (CT) image demonstrating the pathologic mass, as indicated by the arrow. The CT also identified multiple pathologically enlarged lymph nodes in the left neck and axilla.
A core biopsy of the suspicious mass was performed with real-time sonographic guidance. After localizing the mass sonographically, the area of interest was prepped and draped following aseptic procedures and a local anesthetic was administered. Using an 18-gauge needle, five samples were taken from the mass (Figure 5). The procedure was complicated by the proximity of the mass to the subclavian artery and the IJV and the patient’s anxiety; however, the procedure was completed without any morbidity. Histopathology of the biopsy specimens was read as non-Hodgkin lymphoma.
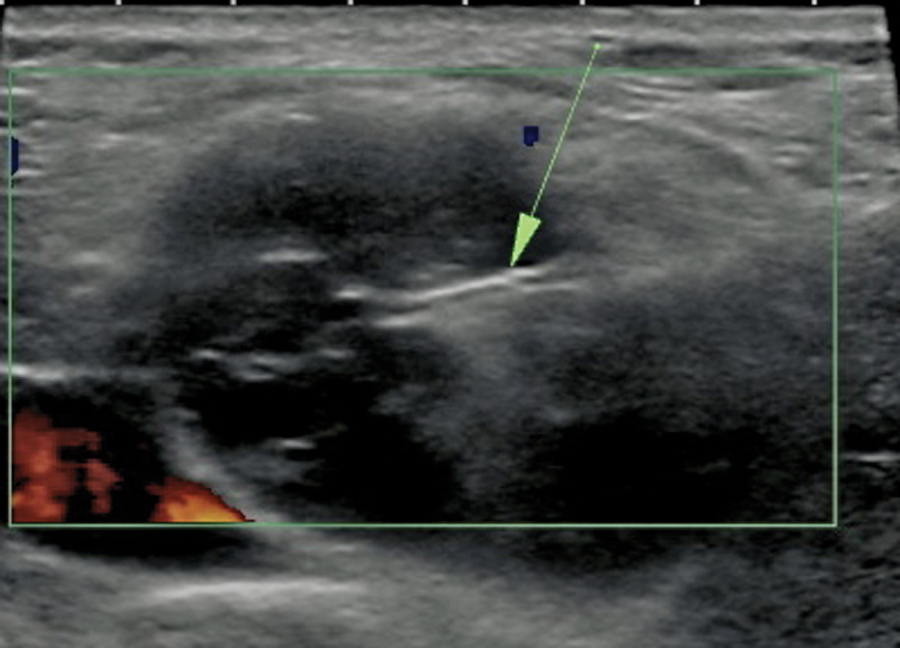
A core biopsy was performed by taking five tissue samples with a biopsy needle, as shown by the echogenic line. Pathologic reports indicated the mass was non-Hodgkin lymphoma.
Discussion
Non-Hodgkin lymphoma is a malignancy that begins in the lymphatic system. 2 This disease is likely to occur more frequently in older, immunocompromised individuals who have had mononucleosis caused by Epstein-Barr virus, have undergone an appendectomy or tonsillectomy, are taking immunosuppressive drugs following an organ transplant, or have an acquired or congenital immune deficiency syndrome. 3
Most malignancies of the lymphatic system are related to abnormalities of B lymphocytes, which may occur at several phases of cellular differentiation. 4 These lymphocytes are transformed from normal cells into malignant cells by different factors such as environmental, hereditary, or acquired factors. 2 These associated genetic lesions initiate a sequence of proto-oncogenes and interrupt tumor suppression genes. 4 Extranodal sites, including the spleen, thymus, tonsils, adenoids, and bone marrow, can also be involved with lymphoid malignancies. 2 Fewer than 25% of patients present with a neck lump. 4 Diagnosis is usually made by obtaining a thorough patient history, physical examination, core tissue biopsy, and diagnostic imaging examinations. Laboratory testing to acquire biochemical indicators such as a blood cell count are also supportive in forming a diagnosis, but these cannot alone diagnose non-Hodgkin lymphoma. 5
This case of non-Hodgkin lymphoma is unique primarily because of the patient characteristics. The patient’s gender and age suggest she would be an unlikely candidate to be diagnosed with this disease, as non-Hodgkin lymphoma is more likely to occur in men and individuals older than age 65. 6 Furthermore, the patient reported having no immunocompromising conditions. Common clinical cases in adolescent and young adult females present with masses involving the abdominal lymph nodes and/or ovaries and may be associated with abdominal ascites. 7 Also, many published clinical cases report involvement of major organs. Computed tomography is the most commonly used modality to diagnose and stage non-Hodgkin lymphoma. Uniquely, in this case, sonography was the primary modality, offering a detailed look at the internal complexity of the mass as well as its vascularity. It also provided a safe method of obtaining a tissue biopsy.
Although some cases of non-Hodgkin lymphoma offer a poor prognosis, this patient’s prognosis is good. Her lymphoma was multicentric, but major organs such as the spleen and bone marrow had not been affected. Because of her young age and early diagnosis, she will most likely fully recover with chemotherapy treatment.
Conclusion
The use of sonography in the case proved useful in evaluating and diagnosing the suspicious neck mass. From obtaining accurate measurements to guiding a biopsy needle into the lesion, sonography proved invaluable in the diagnosis and management of this case. The sonographer’s diligence to go beyond the “ordered” thyroid exam and demonstrate the actual problem was a key action. In these situations, it is the sonographer’s responsibility to thoroughly document the presenting problem to aid in the diagnostic work of other health professionals involved in the case. With the appropriate teamwork of sonographers, radiographers, radiologists, and the patient, diagnosis and the necessary care can be given promptly to allow for adequate patient treatment, as shown in this presented case.
Footnotes
The author declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author received no financial support for the research and/or authorship of this article.