
Abstract
Non-Hodgkin lymphoma (NHL) is a cancer of the immune system, and accounts for 90% of all lymphomas. When lymphoma is discovered outside of the immune system, it is considered extranodal lymphoma. Any organ can be the primary site of NHL, with the gastrointestinal tract being the most common site of involvement. This case study explores the sonographic discovery of an uncommon presentation of NHL with an extranodal mass originating from the pancreatic body and tail, and further extending into the splenic hilum.
Lymphoma can be categorized into two types, Hodgkin lymphoma and non-Hodgkin lymphoma (NHL). NHL usually originates in the lymph nodes, but can also present in primary extranodal sites, such as the stomach, skin, lungs, and rarely, the pancreas.1,2 NHL can be a result of proliferation of B-cells, T-cells, or both, with B-cell lymphoma being more common than T-cell. 3 This case presents a rare example of B-cell NHL originating from the pancreas tail. Sonography and computed tomography (CT) play an important role in diagnosis, but cannot differentiate between inflammatory lymphadenopathy and malignancy. Therefore, a pathological diagnosis is essential in confirming lymphoma and determining the correct course of treatment. 4
Case Report
A 74-year-old woman presented with weight loss, night sweats, and palpable fullness in the left upper quadrant and was referred for an abdominal ultrasound. A prior complete blood count (CBC) revealed that the patient had a decreased red blood cell count and a decreased hemoglobin of 9.0 g/dL, indicative of anemia. The patient’s white blood cell count and additional lab values were within normal limits. Her history was significant for smoking and occasional alcohol consumption. She provided no history of any familial malignancies.
A complete abdominal ultrasound was performed using a Philips iU-22 ultrasound equipment system (Philips Medical, Bothell, Washington) with a 5 MHz curved linear transducer. The images showed a large, heterogeneous mass appearing to arise from the pancreatic body and tail (see Figure 1) which measured 15.7 cm x 15.3 cm x 10 cm. Using color Doppler, the mass demonstrated internal vascularity and extended toward and invaded the splenic hilum (see Figure 2). Lymphadenopathy was also noted in the superior pancreatic-region (see Figure 3), as well as a small left-sided pleural effusion and hepatomegaly, with the liver measuring 21.2 cm. A CT was recommended and confirmed a heterogeneous mass in the left upper quadrant extending from the pancreas to the splenic hilum (see Figure 4). Additional blood work showed the patient’s serum lactate dehydrogenase levels were increased, with levels presenting at 886 u/L.
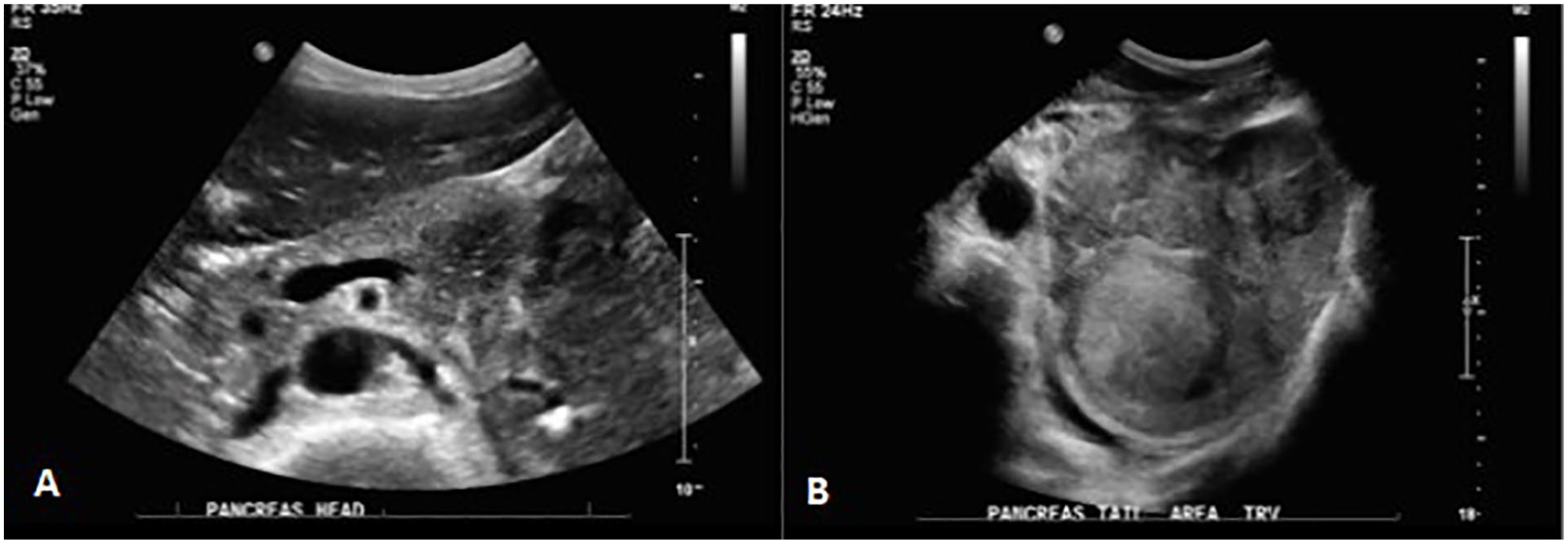
(A) A transverse sonographic image of the pancreatic body showing a portion of the mass (B) A transverse sonographic image of the pancreatic tail region showing mass arising from the pancreatic tail.
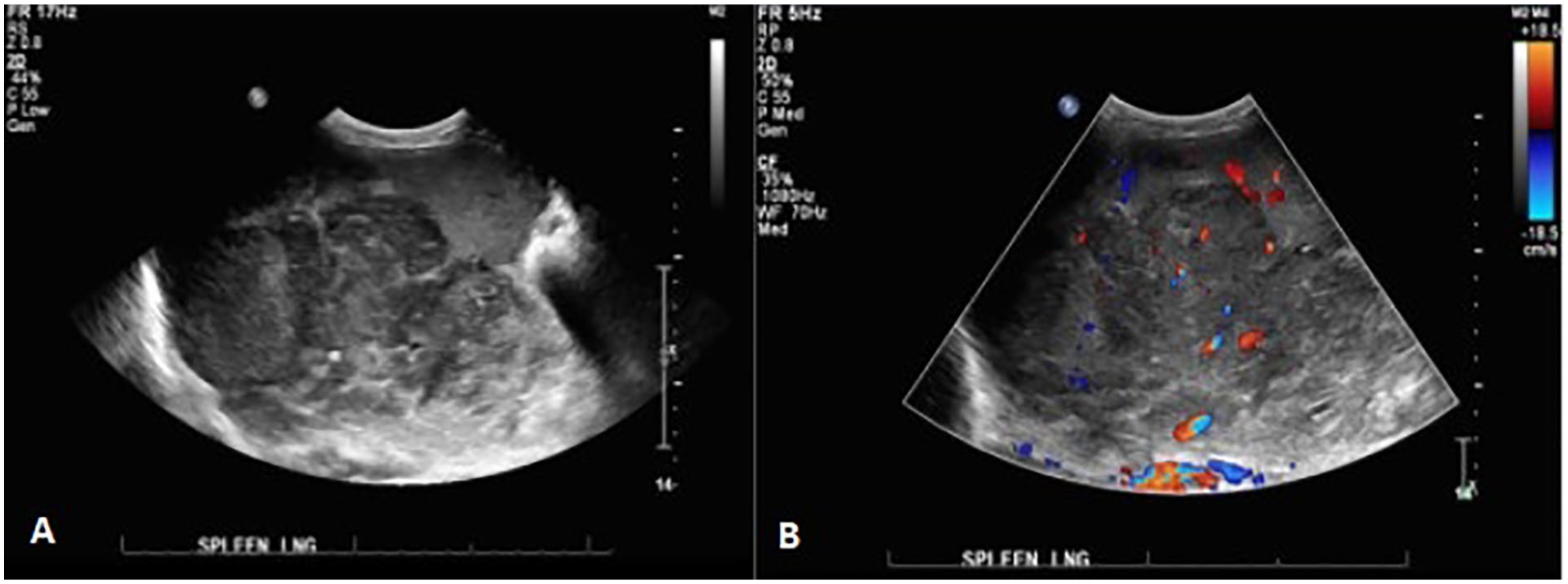
(A) A longitudinal sonographic image of the spleen showing invasion of the pancreatic mass into the splenic hilum (B) A longitudinal sonographic image showing internal vascularity of the mass.

A longitudinal sonographic image showing an enlarged lymph node superior to the pancreatic head.
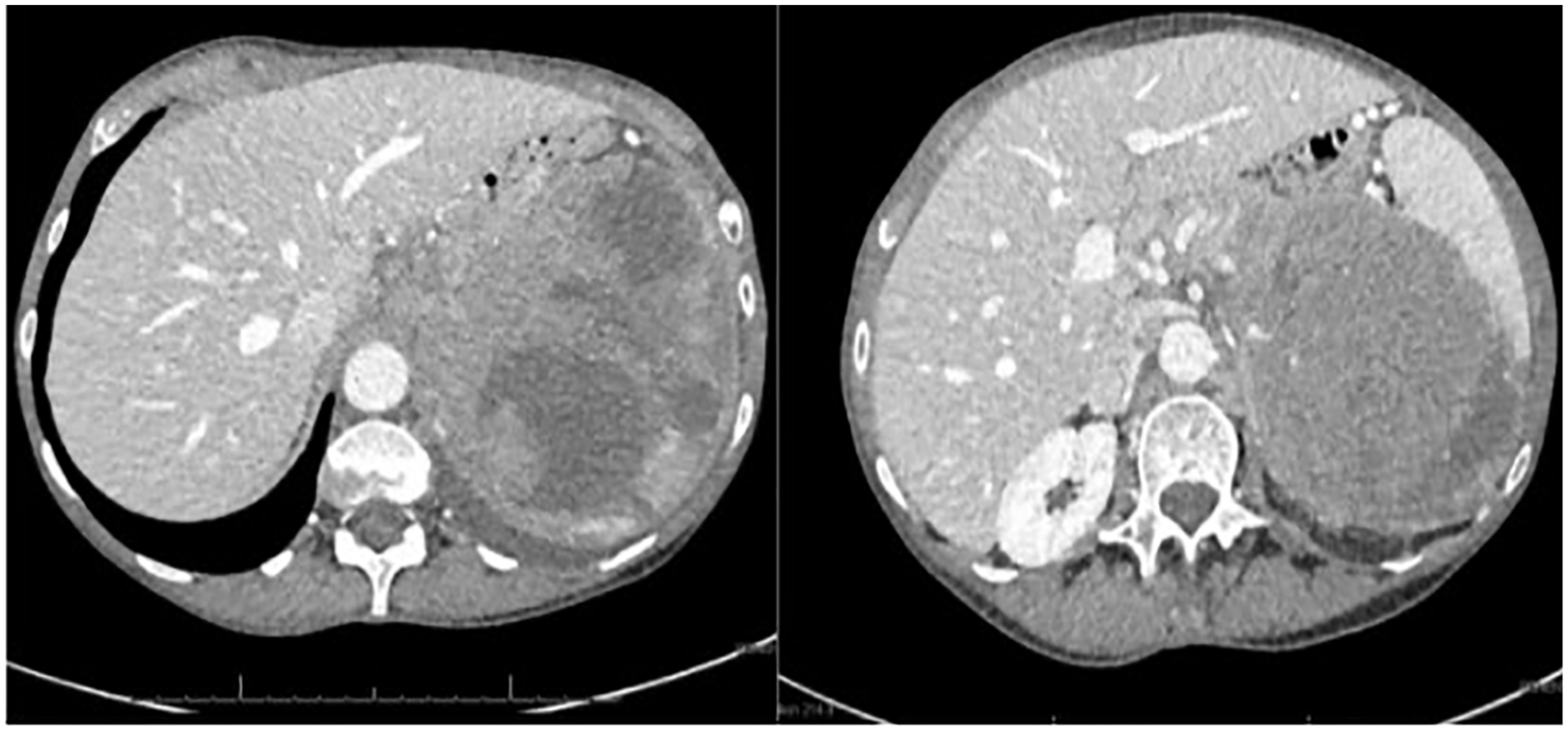
Axial computed tomography (CT) images of the pancreatic mass invading the splenic tissue.
An endoscopic ultrasound guided fine needle aspiration (FNA) was performed of the mass and multiple malignant appearing lymph nodes were again noted in gastrohepatic ligament, celiac region, and peri-pancreatic region. The FNA pathology results were consistent with B-cell lymphoma. The patient was admitted to the hospital for initiation of treatment which included 6 complete cycles of chemotherapy for diffuse large B-cell NHL.
Discussion
Lymphoma is a cancer of the lymphatic system, which is made of the lymph nodes, spleen, thymus, and bone marrow. 5 Lymphoma can be further categorized into Hodgkin lymphoma and NHL, with NHL being the most common in about 90% of cases. 6 NHL can be subdivided into two forms, depending on which cell the lymphoma arises from: B-cells or T-cells. B-cell presentation is the most common form, representing 85% to 90% of NHL. 3 Additionally, NHL may spread from the lymphatic system or present as extranodal disease.
As lymphoma is a cancer of the lymphatic system, it will most commonly begin in one of the lymph nodes and spread throughout the immune system to various places within the body or it may be contained in the lymphatic system. 7 The exact cause of NHL is still not known, but it has been shown that the risk is increased in older, white males, preexisting autoimmune diseases, and immune-suppressing viruses, like human immunodeficiency virus (HIV). 5 A common early clinical sign of NHL involves painless swelling of one or more of the 600+ lymph nodes within the body. However, key clinical features may help to differentiate and diagnose NHL from other cancers which are referred to as “B symptoms.” B symptoms include fever, night sweats, and unexplained weight loss. 7 While these symptoms are important in differentiating NHL from other malignancies, lab values play an important role as well. When NHL is suspected in a patient, a CBC can relay a lot of information about how the invasion is affecting the body. 5 Upon discovery of NHL, about 40% of patients present with decreased red blood cells and hemoglobin, causing anemia. Additional laboratory findings may include leukopenia or leukocytosis, thrombocytopenia, and thrombocytosis. 8
There are 2 types of extranodal NHL. When NHL starts in tissue within organs outside of the lymphatic system, like the pancreas, this is known as primary extranodal disease. This occurs in 25% of NHL, with the gastrointestinal tract being the most common location, followed by the skin. 1 Although lymphoma is not a rare malignancy, primary extranodal disease is uncommon, particularly when arising from the pancreatic body or tail which is referred to as primary pancreatic lymphoma. Less than 2% of patients with NHL have involvement of the pancreas upon presentation. 2 Extranodal lymphoma is classified as secondary if there is involvement of lymph nodes or if there is more than one extra nodal site. Secondary involvement of the pancreas is more common than primary pancreatic lymphoma; however, the overall involvement of the pancreas is rare. 9 The presented case is classified as secondary extranodal pancreatic lymphoma due to involvement of surrounding organs and presence of lymph node metastasis. The Dawson/Behrns criteria help to differentiate primary pancreatic lymphoma (PPL) from secondary, stating that the main criteria for PPL are absence of superficial or mediastinal adenopathy, normal leukocyte count, and confined peripancreatic disease, without hepatic or splenic involvement.10,11 Another key differentiating factor is the location of the lesion as primary pancreatic malignancies typically arise from the pancreatic head. 10 The diagnosis of pancreatic lymphoma may be difficult because the symptoms and initial imaging can closely mimic those of other pancreatic tumors, such as adenocarcinoma or a functioning/non-functioning neuroendocrine tumor.
Several diagnostic characteristics can help differentiate extranodal lymphoma from adenocarcinoma including size and location of the pancreatic mass. The pancreas is composed of a variety of cells including acinar cells, ductal cells, and stromal cells. Acinar cells make up the majority of the pancreas, however, ductal cells are the most common cells to produce a malignant lesion, therefore any mass produced within the pancreas is likely to arise from ductal cells, such as ductal adenocarcinoma. 11 The size of adenocarcinomas are typically less than 10 cm in size while about 60% of pancreatic lymphomas measure above 6 cm. Additionally, the presence of peripancreatic lymphadenopathy and splenomegaly, seen with extranodal lymphoma, are less associated with adenocarcinoma. 10
An additional differential for extranodal lymphoma are pancreatic endocrine tumors (PETs) which are classified by size, clinical symptoms, biologic behaviors, and histologic parameters. Functioning endocrine tumors produce distinct clinical symptoms, while non-functioning do not. PETs vary in size, ranging from less than 1 cm up to 20 cm, with a majority falling into the 1 to 5 cm range. Sonographically, smaller tumors typically present as homogeneous, while larger tumors are typically heterogeneous with areas of necrosis and cystic changes, similar to the appearance of extranodal pancreatic lymphoma. 12 Despite the rarity of PPL or SPL, lymphoma should always be considered as a primary differential in the presence of a large and rapidly growing mass. 10 Laboratory values and biopsy of a mass are key in diagnosing and initiating treatment specific to the tumor, especially because treatments specific to lymphoma vary greatly from those used for primary pancreatic lesions. 10
Treatment for B-cell NHL is the same, regardless of where the mass originates. For patients with NHL, 3 to 6 cycles of a combination of rituxan, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). R-CHOP chemotherapy has been recommended for best results.1,7 This can be followed by radiation, depending on the response to the initial chemotherapy regimen. 1 Like many cancers, early diagnosis and initiation of chemotherapy is important for improving prognostic outcomes. The International Prognostic Index (IPI) may be used for patients with NHL to determine an overall survival prognosis following treatment. Increased risk factors contributing to morbidity are outlined in the IPI and include patients over the age of 60 years, elevated serum LDH, cancer TNM stage of III or IV, an eastern cooperative oncology group (ECOG) performance status more than or equal to 2, and extranodal involvement of more than one organ. Each of those factors is assigned one point, with the scale ranging from 0 to 5. Using this scale, 0 to 1 points is considered low risk/good prognosis, 2 is an intermediate risk, and greater than 3 is considered a high risk. 1
Although CT is the diagnostic modality of choice for evaluating diffuse lymphadenopathy, sonography can still play a very important role in evaluating lymphoma. 4 It is important to document any associated lymphadenopathy in the areas surrounding abdominal masses, as this can be an important indicator of lymphoma.13,10 Sonographically, normal lymph nodes have an elongated shape and a fatty hilum. Lymph nodes that have been invaded by lymphoma are typically homogenous, enlarged and often have a rounded appearance. In the case of lymphoma infiltrating the pancreas, peripancreatic adenopathy is important to note.13,10 Sonography also plays an important role in the guidance of endoscopic guided fine needle aspiration by enabling real-time images while sampling target lesions and providing a minimally invasive access to masses. 4 Diagnostic imaging is useful for characterizing masses and lymph nodes; however, pathology is needed for a definitive diagnosis.
Conclusion
Although NHL is a malignancy that typically originates in the lymph nodes and spreads throughout the immune system, lymphoma may also present as primary or secondary extranodal disease. Extranodal pancreatic NHL is not common, but may be evaluated with multiple imaging modalities. While CT is considered the gold standard for evaluation of lymphoma associated lymphadenopathy and extranodal masses, sonography can also be a valuable imaging tool and can play an important role in guidance for procedures to obtain samples of masses. It is important to consider extranodal lymphoma when sonographically evaluating masses within soft tissue organs. Sonography can aid in earlier diagnosis and initiation of treatment which can improve prognostic outcomes.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.