
Abstract
Objective:
Interprofessional collaboration is crucial in providing high-quality care for patients. Professional organizations and accrediting agencies recognize the importance of interprofessional education (IPE) and have required that it be incorporated into curricula. The purpose of the study was to assess faculty, from various disciplines, attitudes, knowledge, and barriers associated with IPE.
Materials and Methods:
A descriptive correlational research design was used to assess attitudes, knowledge, and barriers associated with IPE among faculty at a Midwestern college of health sciences.
Results:
Findings indicated that faculty lacking IPE knowledge, barriers of time, motivation, and scheduling were factors that influenced IPE. Overall, faculty indicated that they were enthusiastic about participating and willing to learn. Those who attended an intervention, which consisted of an educational presentation and activity, provided statistically significant perceptions about IPE.
Conclusion:
These results indicate that faculty attitudes, knowledge, and barriers influenced incorporation of IPE into curricula.
Key Takeaways
Interprofessional education (IPE) is essential to ensure faculty have the knowledge and tools to successfully implement activities in the classroom and clinical setting.
Factors that influence IPE implementation include time, scheduling, knowledge, and motivation. These factors must be addressed for successful incorporation of IPE to occur.
Begin IPE incorporation with faculty champions who are more enthusiastic and willing to learn about IPE.
Interprofessional education (IPE) is defined as “learning about, with, and from each other to enable effective collaboration and improve health outcomes.” 1 Moreover, it has become prevalent in the dialogue of quality health care education and a necessary component in health sciences curricula.1,2 Interprofessional collaboration is crucial in providing safe, accessible, quality patient care and improves patient outcomes.2,3 Exposing health care students to IPE in both the classroom and clinical setting helps to cultivate mutual trust and respect, confronts misconceptions and stereotypes, and dispels prejudice and rivalry between professional groups. 4
While the aforementioned conveys many of the benefits associated with IPE, the successful implementation of IPE can fail to gain traction given the presence of various barriers. These barriers include but are not limited to scheduling conflicts, time, complex timetables, and a lack of faculty understanding.2,5,6
Many professional organizations and accrediting agencies have recognized the importance of IPE and have included it as an accreditation standard. 3 As of 2019, at least 20 accrediting agencies in various health care professions have formally endorsed the Health Professions Accreditors Collaborative (HPAC) Guidance on Developing Quality Interprofessional Education for the Health Professions. 7 This is in contrast to a comparative analysis done in 2013, in which it was noted that accrediting agencies, within the United States, lacked similar expectations related to IPE, within their standards. 8 It is of note that nursing and pharmacy, in the 2013 analysis, did include IPE mandates in their accreditation standards.
Since the 2013 analysis, there has been a shift, in the United States, to more health care accreditation commissions and committees mandating IPE standards, within curricula. For example, physician assistant programs, accredited through the Accreditation Review Commission on Education for the Physician Assistant (ARC-PA), along with the Commission on Accreditation for Respiratory Care (CoARC) and the Joint Review Committee for the Accreditation of Educational Programs in Diagnostic Medical Sonography (JRC-DMS) now mandate that IEP is completed, within a program’s curriculum.9–11 The 2021 updated standards of Radiography’s Joint Review Committee on Education in Radiologic Technology (JRCERT) encourage IPE development. 12 Cardiovascular Sonography’s Joint Review Committee for the Accreditation of Educational Programs in Cardiovascular Technology (JRC-CVT), as of the 2015 update, has not included IPE. 13
In pharmacy, the Accreditation Council for Pharmacy Education (ACPE) mandates students are provided IPE as well as demonstrate IPE competencies, as a part of a health care team. 14 The National Association of Boards of Pharmacy (NABP) that oversees the North American Pharmacist Licensure Examination (NAPLEX) lists interdisciplinary and collaborative practice in their competency statements, for the licensure exam. 15 IPE requirements within nursing curricula are mandated by the Accreditation Commission for Education in Nursing (ACEN) and the Commission on Collegiate Nursing Education (CCNE).16,17 Hence, the National Council of State Boards of Nursing (NCBSN) includes collaboration with an interdisciplinary team, in the test plans for the National Council Licensure Examination for Registered Nurses (NCLEX-RN). 18
After exploring multiple organizations’ registry and licensure exam requirements in allied health professions, it was discovered that IPE requirements are not consistent. Registry requirements for the American Registry for Diagnostic Medical Sonography (ARDMS), the American Registry of Radiologic Technologist (ARRT), and Cardiac Credentialing International (CCI) do not have specific statements related to IPE.19–21 If sonography and radiologic health care professions follow the same history, as other accreditation agencies and licensure exams in pharmacy and nursing, then experiences in IPE may become a requirement for taking credentialing exams.
Due to the benefits and accreditation standards, faculty should implement IPE into curricula. However, research is limited when addressing faculty perspectives about IPE. For IPE initiatives to be successful, faculty’s attitudes should be assessed. 22 Negative faculty attitudes may lead to a lack of IPE participation and threaten the implementation and maintenance of activities.2,23,24 Understanding the perceptions that faculty have toward IPE can provide guidance in planning IPE initiatives. 25
A faculty learning community (FLC) was formed at a Midwestern health sciences college to further explore IPE implementation into their curricula. The purpose of this study was to gauge faculty, from various disciplines, attitudes, knowledge, and barriers associated with IPE.
Materials and Methods
The study was a descriptive, correlational survey design. The research setting encompassed a Midwestern health sciences college which included sonography, nursing, biomedical sciences, and graduate programs. Inclusion criteria included participants who were adjunct, part-time, and full-time faculty (see Table 1). Ethical approval for this study was obtained from the Institutional Review Board (IRB) at the Midwestern health sciences college (IRB#1904-001). As participants entered the survey, they were informed that participation was voluntary, and responses were anonymous. Participants were instructed that completion of the surveys served as the informed consent.
Descriptive Information Obtained as Part of the Pre-Post Intervention.
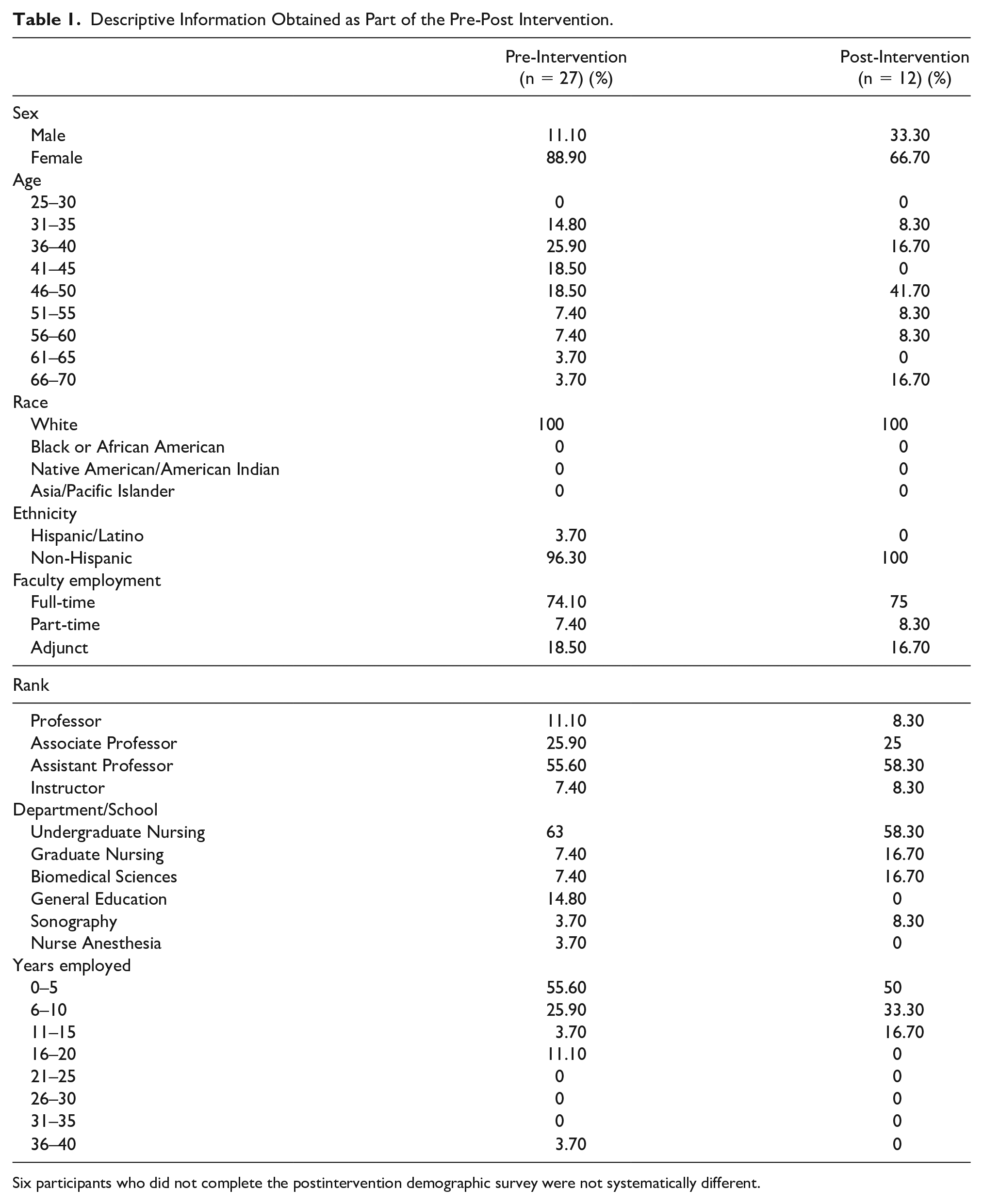
Six participants who did not complete the postintervention demographic survey were not systematically different.
This study used three surveys to collect data from participants. A demographic survey was developed by the authors and assisted in collecting general information about participants (see Supplemental Material). The Attitudes toward Interprofessional Education, a 15-item Likert-type scale, was used after receiving permission from the author. 26 The purpose of the survey was to identify faculty attitudes related to IPE prior to and following a formalized intervention. The 15-item survey uses a 5-point Likert-type scale (5 = strongly agree to 1 = strongly sisagree). A Cronbach’s alpha has been calculated for this survey24,26,27 as 0.88, 0.92, and 0.90. A faculty assessment of IPE survey, developed by the authors, collected information about faculty’s IPE knowledge, participation in IPE experiences, and activities, as well as factors that influence IPE participation (see Supplemental Material).
Faculty were invited to participate by completing preintervention surveys. The collected data were analyzed using the Statistical Package for the Social Sciences (SPSS).
After surveying the faculty, an intervention was provided by consultants from the Center for Interprofessional Practice, Education and Research from a local university and encompassed an educational presentation. The presentation discussed the importance of IPE in health care, defined essential terms, recognized current national standards, and identified ways to incorporate IPE into curricula. During this presentation, the consultants facilitated a 20-minute classroom IPE learning activity, which included a case study of a client who had an appointment at a free community health clinic. Faculty, from various disciplines, worked together to plan a comprehensive plan of care for this client. The goal of the activity was to show faculty that IPE can be incorporated into the classroom and that activities do not require an abundance of resources to be effective.
Participants were asked to complete the postintervention surveys. The postintervention consisted of participants taking the three original surveys that were completed as a preintervention.
Results
Preintervention survey results showed that 29.6% of faculty were knowledgeable about IPE, whereas 44.4% were somewhat knowledgeable and 18.5% identified they were not knowledgeable. Only 25.9% of the faculty indicated that they received previous IPE training. There were no significant differences associated with the faculty’s past IPE training and their attitudes toward IPE. However, when asked pre-intervention about their enthusiasm to participate in IPE, 68% of faculty were enthused or very enthused and 81% were willing or very willing to learn about IPE. Faculty identified time (85.2%), scheduling (77.8%), knowledge (74.1%), attitudes (59.3), collegiality (51.9%), and motivation (51.9%) as factors that influenced IPE participation (see Figure 1). Collaboration, promotion of knowledge, education, and academic and clinical excellence were faculty’s perceptions of how IPE fulfills the college mission.
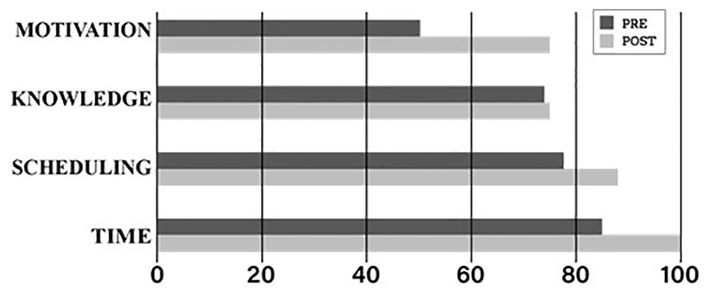
Percentage of leading factors influencing participation in IPE pre-post intervention. IPE, interprofessional education.
Comparisons were completed using a t-test that examined the mean ratings for participants who rated themselves as less enthusiastic to participate in IPE. Similarly, comparisons were made for those less willing to learn IPE with the mean ratings of those who rated themselves as more enthusiastic and more willing. Faculty who were more enthusiastic and more willing to learn IPE demonstrated statistically significant (P < .05) ratings in the following statements from the Attitudes toward Interprofessional Education survey (see Table 2).
Statistically Significant Statements Identified by the Faculty Who Were More Enthusiastic and Willing to Learn About IPE.
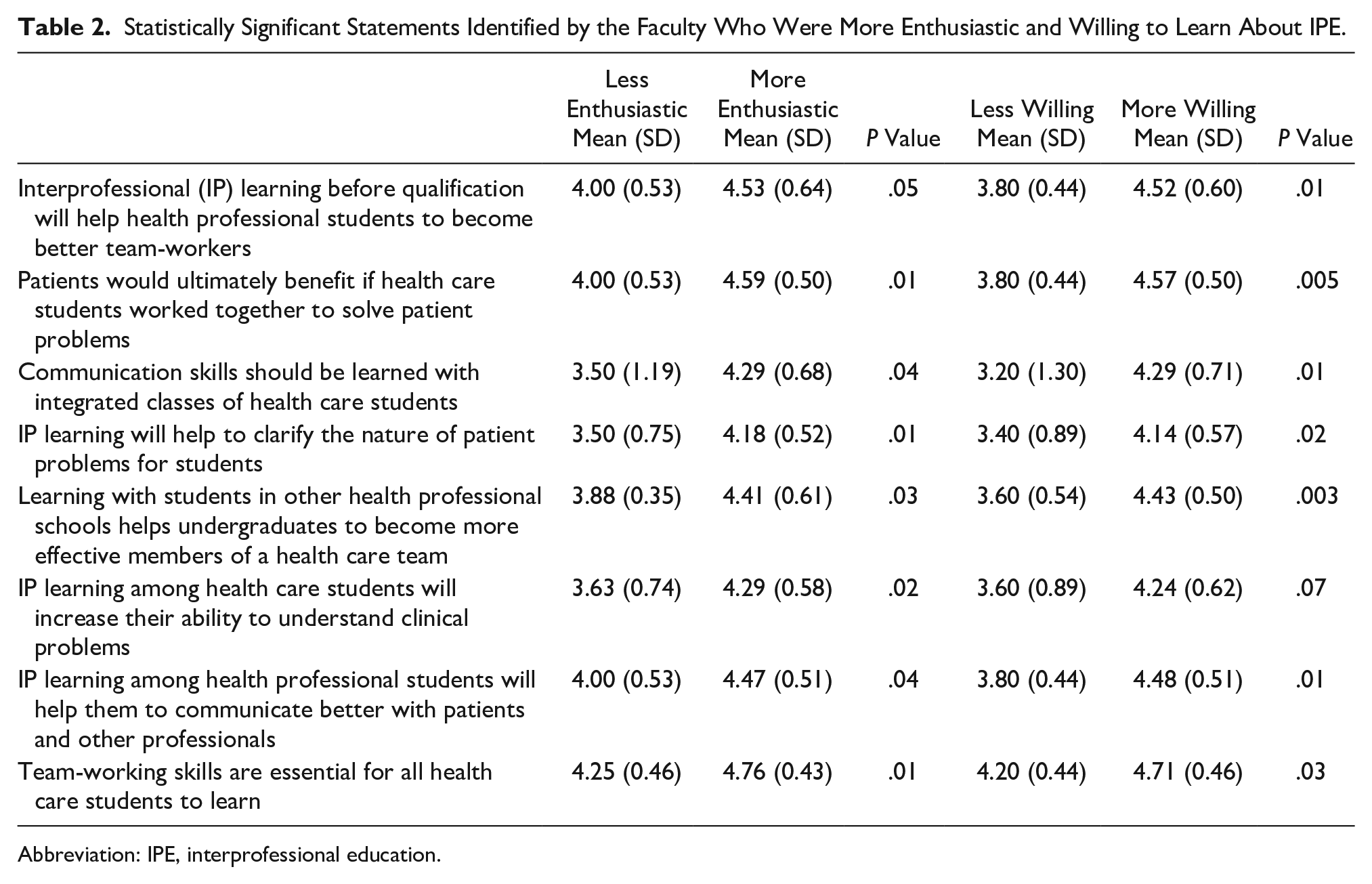
Abbreviation: IPE, interprofessional education.
Of the 18 faculty who completed the survey post-intervention, 44% indicated that they attended the presentation and learning activity. Of those who attended, 62.5% indicated they were knowledgeable about IPE, 25% somewhat knowledgeable, and 12.5% very knowledgeable. Results showed that faculty, who attended the presentation and learning activity, remained enthused (25%) or were very enthused (50%) to participate in IPE while remaining willing (25%) or very willing (75%) to learn about IPE. The factors identified that influenced IPE participation post-intervention were time (100%), scheduling (88%), knowledge (75%), and motivation (75%) (see Figure 1). A t-test set of comparisons revealed the mean response of the Attitudes toward Interprofessional Education survey from those who attended and those who had not; significant findings (P < .05) were found. Those who attended the intervention provided significantly higher ratings on the following statements (see Table 3).
Statistically Significant Statements Identified by Faculty Who Attended the IPE Interventional Session.

Abbreviation: IPE, interprofessional education.
Discussion
Members of the FLC assumed that faculty at a Midwestern health sciences college had inherent knowledge about IPE and knew how to incorporate it into curricula. This study found that this was not apparent and overall faculty influenced the occurrence of IPE experiences. The barriers to participation, in IPE, were identified by faculty as knowledge, motivation, scheduling, and time.
Pre-intervention, the majority of faculty indicated that they were knowledgeable (29.6%), somewhat knowledgeable (44.4%), or lacked knowledge (18.5%) about IPE. Faculty also indicated that knowledge was a leading factor that influenced participation. Of those who attended the intervention, the majority indicated they were knowledgeable (65.5%) or somewhat (25.5%) knowledgeable about IPE; no one indicated that they lacked knowledge. However, faculty still identified that knowledge was a leading factor that influenced participation. This substantiates that education did improve knowledge of faculty, but evidence suggests that additional education is needed for faculty to feel comfortable in implementing IPE. This finding was consistent with the literature in that it was recognized that faculty development was essential for the successful implementation of IPE.5,28,29 Faculty development should include knowledge about IPE, address beliefs and attitudes that may impact IPE, establish skills on how to teach it, and provide knowledge on how incorporate it into curricula. 5 In addition, administrative support for faculty development is essential. 28
Motivation was identified as a factor that influenced IPE participation, by half of the faculty surveyed pre-intervention. Prior to the intervention, the majority of the faculty (72%) indicated that they were somewhat enthused or enthused about IPE, whereas half of the participants (50%) indicated that they were somewhat willing or willing to learn about IPE. Of those who attended the intervention, there was an increase in enthusiasm for IPE in that half (50%) indicated that they were enthusiastic, with the remainder (50%) of participants indicating they were somewhat enthused or enthused.
There was also an increase in willingness in that the majority of faculty (75%) indicated that they were very willing to learn IPE, with 25% of faculty being somewhat willing or willing to learn. Faculty, who attended the intervention, provided statistically significant perceptions on the benefits of IPE. These results were linked to an increase in motivation in faculty post-intervention.
Faculty investment is essential for IPE engagement and development. 29 A predictor of success identified in the literature was the utilization of faculty champions, who were cultivated through faculty development. Faculty champions promote and role-model IPE to administration, students, and faculty. 6 This study supported this recommendation in identifying faculty champions based on their enthusiasm, willingness to learn, and motivation about IPE.
Time was another factor that was identified as a barrier. Faculty at the Midwestern health sciences college had a misperception about what IPE consisted of. Most faculty identified that IPE experiences were an all-day event, requiring multiple resources. Through the intervention, it was discovered that IPE learning activities, such as a brief 20-minute case study, could be incorporated into both the classroom and clinical setting. The goal was to illustrate to faculty that IPE activities do not require many resources, such as time, while still being effective. All participants who attended the intervention indicated that time continues to be an influencer but recognized this may be a positive influence on IPE implementation.
Scheduling was identified in the literature as a barrier to IPE implementation, which consisted of lack of space large enough to accommodate a group along with finding time in which all programs can participate. 28 This was consistent with the findings from this study in that faculty identified scheduling as an influence both pre- and post-intervention. The literature suggested strategies to overcome this barrier. First, time and space can be mandated within an institution, for dedicated IPE activities. Online asynchronous activities should be considered if time and space are an issue. The scheduling of small group experiences may also be an option. 28
Limitations
The research design was pre-experimental and therefore has threats to internal and external validity. In addition, the pre-post survey participants were of a small, nondiverse sample. The sample of participants also varied between pre and post surveys, which was recognized as an additional limitation. The postintervention demographic survey was separated from the survey per IRB requirement. Because of this, six participants did not complete the postintervention demographic survey and were not systematically different from other participants.
Conclusion
As more accrediting bodies, such as JRC-DMS, JRCERT, and CoARC, incorporate IPE into their standards and guidelines, it will likely also need to be implemented into curricula.10–12 Health care students should be exposed to IPE experiences as they will be expected, within their professional role, to work collaboratively to improve patient outcomes.
The results of this study found faculty influence IPE incorporation into curricula. Faculty education about IPE and activities that promote it within the classroom and clinical setting is essential. Future recommendations include additional faculty education about IPE and how it can be easily implemented within the classroom and clinical setting. Additional research is necessary to determine how much education is needed to effectively support faculty. Replication of this study is encouraged with a larger, more diverse sample that includes other health care professions.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793221088813 – Supplemental material for Are your Faculty Onboard With Interprofessional Education (IPE)?
Supplemental material, sj-docx-1-jdm-10.1177_87564793221088813 for Are your Faculty Onboard With Interprofessional Education (IPE)? by Julie A. Skrabal, Stacey A. Shutts, Julie K. Morbach, Paul L. Stevens and Barbara J. Sittner in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793221088813 – Supplemental material for Are your Faculty Onboard With Interprofessional Education (IPE)?
Supplemental material, sj-docx-2-jdm-10.1177_87564793221088813 for Are your Faculty Onboard With Interprofessional Education (IPE)? by Julie A. Skrabal, Stacey A. Shutts, Julie K. Morbach, Paul L. Stevens and Barbara J. Sittner in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The authors would like to acknowledge the following individuals for their support and encouragement when completing the research project: Kelsi Anderson, PhD, June Smith, PhD, Lindsay Kruse, MEd, Andrea Dinkelman, PharmD, MS, and Robin Spangler, MSN, RN.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bryan College of Health Sciences provided financial support for consultants from the Center for Interprofessional Practice, Education and Research at a local university which encompassed an educational presentation and learning activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.