
Abstract
Duplex sonography of extracranial arteries is one of the best tools for identifying stenoses and other diseases of the carotid, vertebral, and subclavian arteries. Abnormal Doppler waveforms in vertebral arteries could be evidence of subclavian steal syndrome. The difference of 15 to 20 mm Hg or more in systolic bilateral brachial arterial blood pressure measurements provides important clinical information in patients with subclavian steal syndrome. Complementary to duplex sonographic scanning, radiologists use computerized tomography angiography, magnetic resonance angiography, and digital subtraction angiography for preoperative planning.
Subclavian steal syndrome (SSS) is a relatively rare vascular abnormality that could be challenging to diagnose. Complete understanding of the hemodynamics of SSS, proper sonographic scanning technique, and knowledge of the clinical presentation of the syndrome are the key factors for a successful examination.
Case Presentation
Extracranial arterial duplex sonographic imaging was performed on a woman in her early 80s with atherosclerosis, arterial hypertension, and left arm weakness; she had a history of left subclavian artery stenosis and high-grade left internal carotid artery stenosis, and she had undergone left carotid endarterectomy two years prior to the current test.
The examination started with measuring brachial arterial blood pressure (BABP). The right systolic BABP measured 165 mm Hg; the left was 100 mm Hg (65-mm Hg difference). Duplex sonographic examination of the extracranial arteries was performed after the BABP measurements, using a GE-Logiq 9 (General Electric Medical Systems, Milwaukee, Wisconsin) with a linear 7.5-MHz transducer. The protocol used included bilateral scanning of the common carotid artery (CCA), internal carotid artery (ICA), external carotid artery (ECA), and vertebral artery (VA).
Calcified plaques at the distal right CCA and a large calcific plaque in the right carotid bulb were visualized. There was a high-grade stenosis of the proximal segment of the right ECA. There was 60% to 80% stenosis of the right carotid bulb. Small calcific plaque was visualized in the left carotid bulb. An alternating (to-and-fro) color flow or partial steal pattern of Doppler waveforms in the left VA was detected (Figure 1).
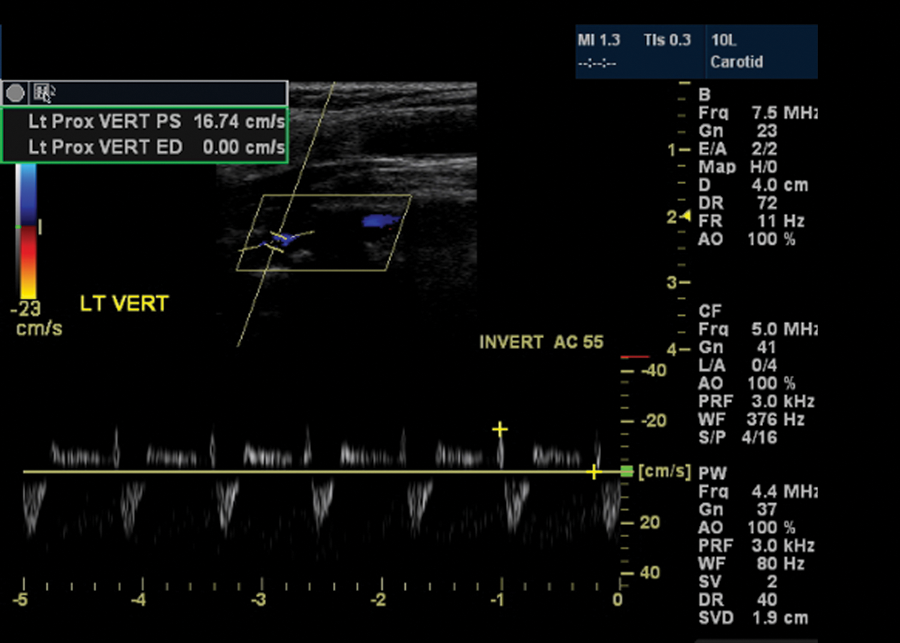
Duplex sonography: a partial steal pattern of Doppler waveforms (above and below the baseline) is in the left vertebral artery (VA). Note the blue coloration in the vertebral artery by color Doppler in the upper half of the image. With the same color setup (see the reference color-box on the left), there was red-coloration only in the nonaffected right VA.
Because pulse-Doppler interrogation of the left vertebral artery revealed abnormal waveforms, duplex examination was performed bilaterally, including the proximal segment of the subclavian artery (SA)—proximal to the takeoff of the VA.
Concurrently, a high-grade stenosis of the proximal left SA with a peak-systolic velocity (PSV) of 327 cm/s was detected (Figure 2). The right VA showed normal antegrade Doppler waveforms and normal color flow (Figure 3). The proximal segment of the right SA had normal, high-resistant Doppler waveforms with PSV of 175 cm/s (Figure 4).
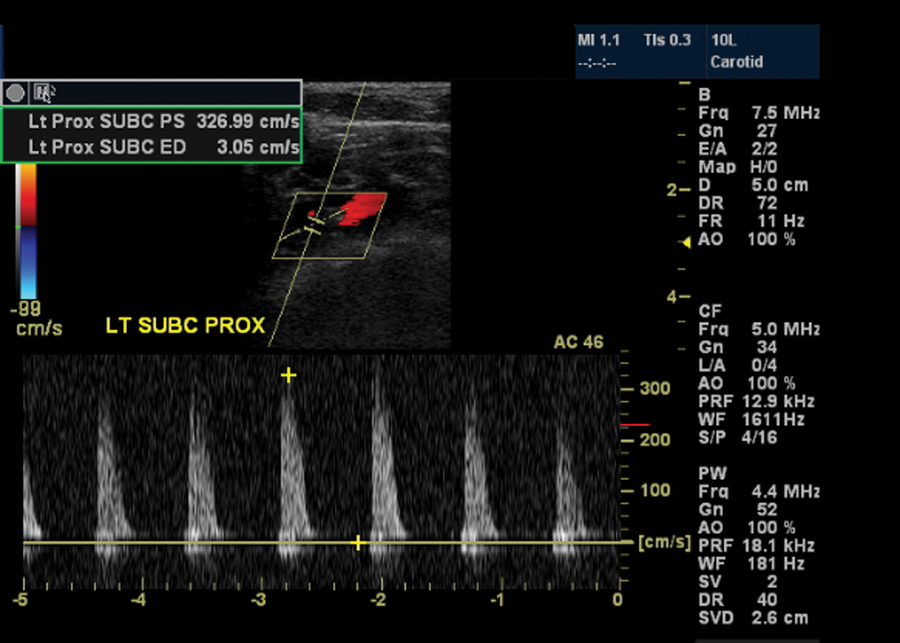
Duplex sonography—subclavicular approach: high-grade stenosis of the proximal (prior to the vertebral artery origin) left subclavian artery with peak-systolic velocity of 327 cm/s.
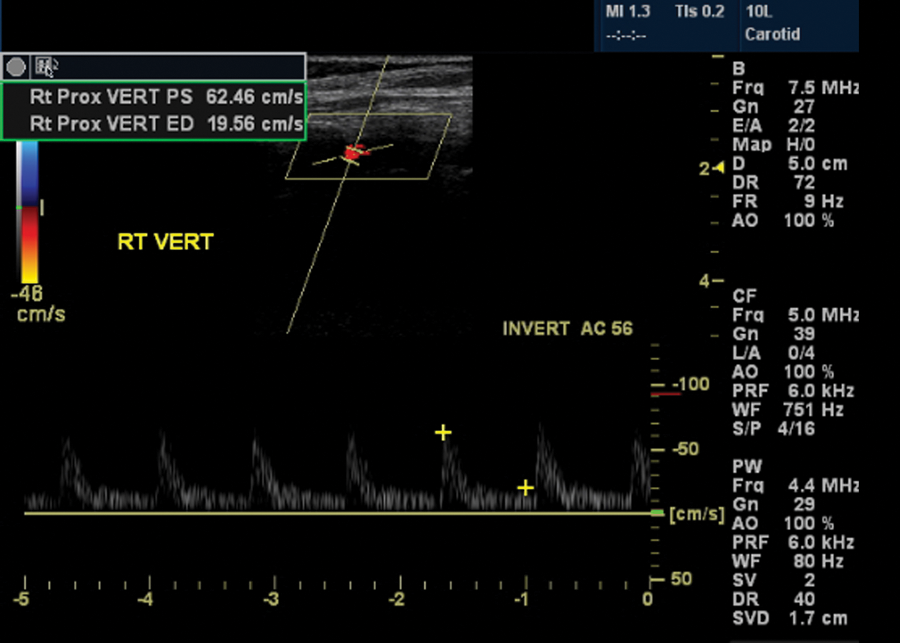
Duplex sonography: normal right vertebral artery: normal Doppler waveforms and normal peak-systolic velocity.
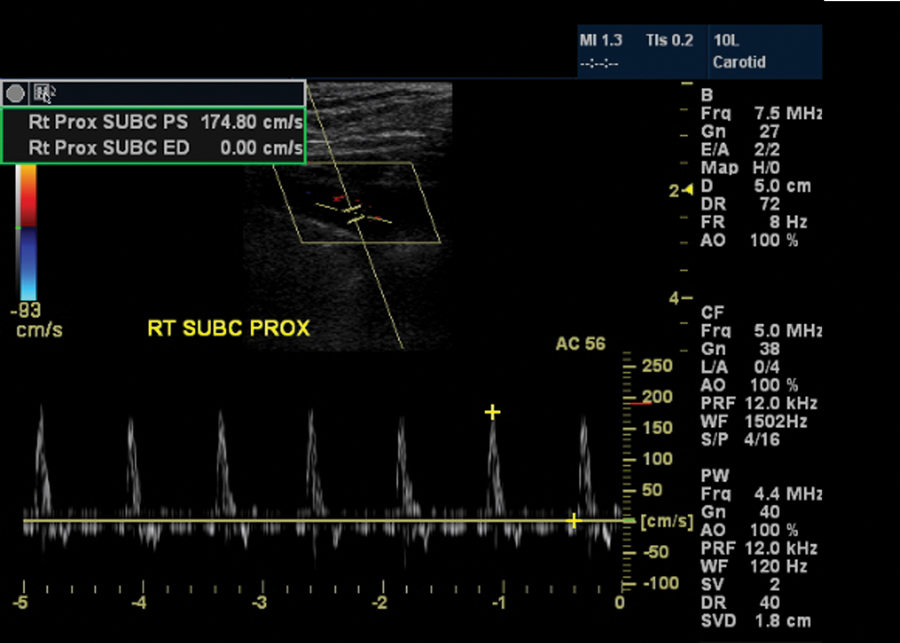
Duplex sonography—subclavicular approach: normal right subclavian artery: normal Doppler waveforms and normal peak-systolic velocity.
The PSV in the right CCA was 58 cm/s. The PSV in the right ICA was 160 cm/s, which corresponds to the increased right ICA/CCA ratio of 2.72 (normal <1.8). PSV in the left CCA was 88 cm/s, the PSV in the left ICA was 79 cm/s, and the left ICA/CCA ratio measured 0.89 (normal). These findings were compared with the results of the patient’s prior examinations.
Two years prior to the current duplex scan of the extracranial arteries, the patient had magnetic resonance angiography (MRA) of the neck with and without contrast. That examination was performed on a GE 1.5 Tesla Signa Horizon LX magnetic resonance scanner (General Electric Medical Systems). The contrast portion of the examination was performed with an intravenous bolus administration of 30 cc of Optimark, 0.5 mmol/mL (Mallinckrodt, St. Louis, Missouri). Severe stenosis (approximately 75%) of the left SA, proximal to the origin of the left VA, was detected (Figure 5). The innominate right SA, bilateral CCA, and bilateral VA were patent without significant stenoses (Figure 6). Moderate stenosis of the origin of the right ICA and mild stenosis of the proximal cervical segment of both ICAs were also found.

Magnetic resonance angiography with contrast (coronal view): severe stenosis of the left subclavian artery, proximal to the origin of the left vertebral artery. The left vertebral artery is clearly seen.

Magnetic resonance angiography with contrast (coronal view): normal right subclavian artery without evidence of hemodynamically significant stenosis. The right vertebral artery is clearly seen.
The patient has also had a computerized tomography angiography (CTA) of the neck with and without contrast in the same year as the MRA. CTA of the neck was obtained on a GE Discovery LS 1.5 Tesla scanner (General Electric Medical Systems), using 1.25-mm collimation, following the intravenous administration of 125 cc of Optiray 320 (Mallinckrodt).
CTA images of the proximal left SA demonstrated a circumferential mural thickening with a high-grade stenosis, just prior to the left VA origin, with luminal narrowing measuring 0.17 cm, distally measuring 0.63 cm, resulting in approximately 75% stenosis (Figure 7). The right VA origin was normal. There were also calcific and noncalcific plaques involving the right proximal SA without stenosis (Figure 7). There was also a mild stenosis of the origin of the right ICA measuring approximately 32% by North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria. Extensive calcific and noncalcific plaques were demonstrated at the origin of the right ECA, which resulted in a high-grade stenosis. The left carotid bifurcation and ICA were normal.
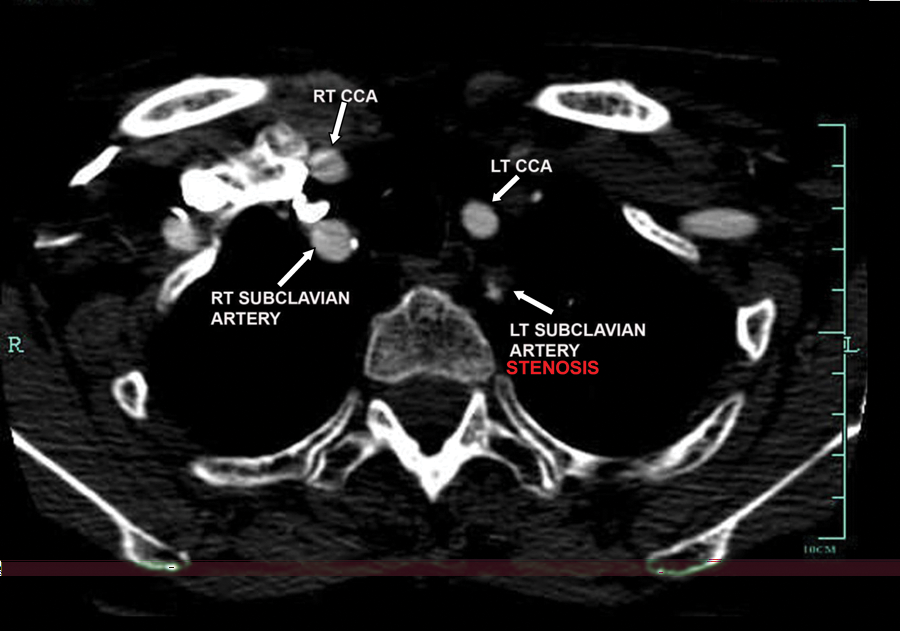
Computerized tomography angiography with contrast (axial view): both stenotic left subclavian artery and normal right subclavian artery are seen in this picture.
Discussion
Subclavian steal syndrome is a hemodynamic phenomenon when a stenotic or occluded subclavian artery (or innominate artery) pulls blood from the contralateral side because of significantly decreased blood pressure in poststenotic parts of the affected artery. Arterial blood from the VA flows to the ipsilateral SA (or innominate artery) via a junction of the two vertebral arteries (Figure 8); the diseased subclavian artery “steals” blood from the vertebrobasilar system.
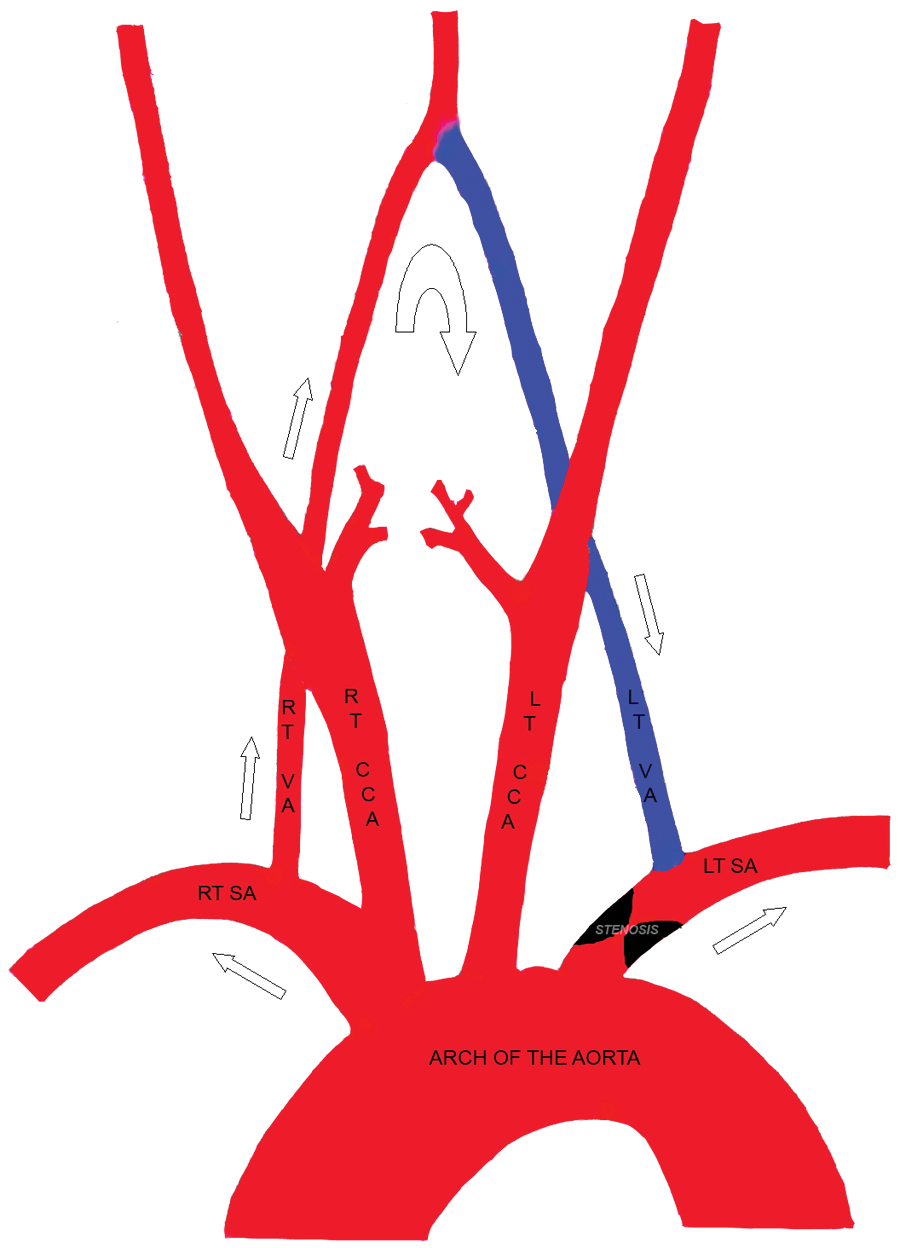
Diagram of hemodynamics in subclavian steal syndrome with high-grade stenosis of the left subclavian artery (SA). The left SA “steals” blood from the right SA via a junction of two vertebral arteries—at the origin of the basilar artery. Red color depicts normal direction of arterial blood flow; blue color shows abnormal blood outflow from the left vertebral artery (VA) into the poststenotic part of the left SA. CCA, common carotid artery; LT, left; RT, right.
One of the first scientific papers that used the term subclavian steal syndrome was published in 1963 by Fischer and Mattey. 1 The first surgical treatment of SSS was described in 1964 by Parrott. 2
SSS affects mostly the left side (up to 85% of all cases). 3 The most common cause of SSS is atherosclerotic plaque formation with subsequent stenosis or occlusion of the proximal part of the SA (or innominate artery) prior to the VA’s takeoff. Other factors that cause SSS include vasculitis, dissection, trauma, or a neoplastic mass. 3
Usually, hemodynamically significant (50%–60% or higher) stenosis of the proximal SA leads to the development of SSS.4,5 Depending on the severity of SA stenosis, there are different variants of abnormal Doppler waveforms in the affected VA (Figure 9).4,6
Different variants of Doppler waveforms in the normal and affected vertebral artery. Occult subclavian steal corresponds to the milder form of hemodynamically significant subclavian artery stenosis, partial subclavian steal corresponds to the moderate form, and complete steal is observed in severe cases.
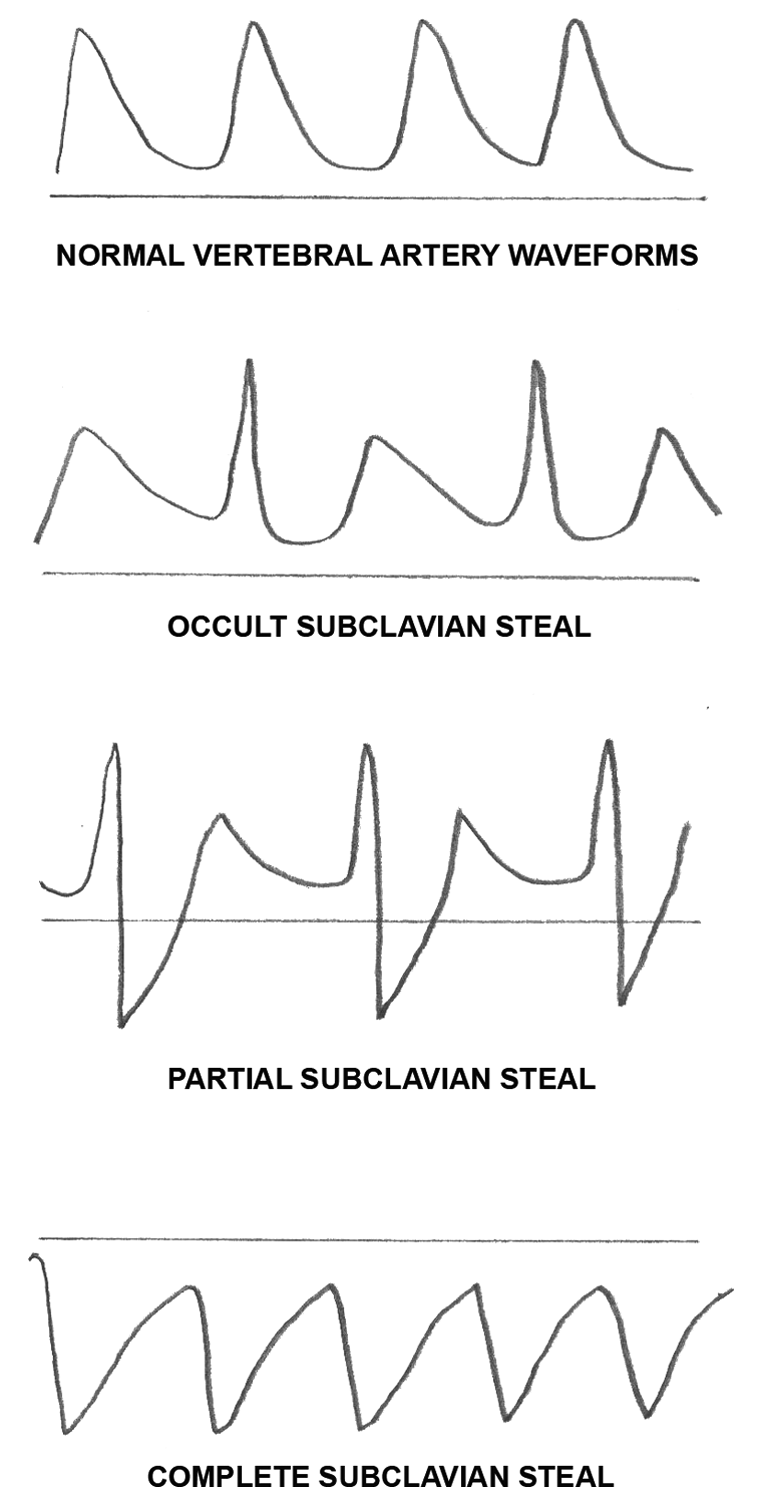
Occult subclavian steal (the affected side’s VA Doppler waveforms demonstrate antegrade flow with mid-systolic notch—the “bunny sign”) corresponds to the milder form of hemodynamically significant SA stenosis, partial subclavian steal (alternating “to-and-fro” waveforms) corresponds to the moderate form, and complete steal (retrograde flow in the VA) is observed in severe cases. This classification is approximate because some other factors influence the hemodynamics between the subclavian and vertebral arteries such as congenital variations of the circle of Willis, congenital hypoplasia and patency of VA, development of collaterals, extension of atherosclerotic plaques, and so on.
Most patients with subclavian steal syndrome are asymptomatic. Up to 35% of patients with SSS could have dizziness, drop attacks, and exercise-induced pain in the arm on the affected side (arm claudication).7,8 Initial diagnosis of SSS is based on the results of physical examination, especially the systolic BABP difference between arms. The arm that has the lower blood pressure is on the affected side.9,10 Different imaging methods are used to diagnose SSS. Usually, duplex sonography of extracranial arteries, including vertebral and subclavian arteries, confirms SSS and gives the first estimation of the severity of the SA stenosis. MRA, CTA, and/or digital subtraction angiography (DSA) are used for a preoperative evaluation of the degree of SA stenosis and comprehensive evaluation of collaterals, congenital anomalies, and so on. 3 Surgical treatment of symptomatic SSS includes angioplasty (with or without stent deployment) of the stenotic portion of the SA, CCA-to-SA bypass, or innominate-to-SA bypass. 3
Conclusion
Bilateral arterial brachial blood pressure measurement provides important clinical data for SSS assessment and should be recorded in all patients with SSS. Duplex sonographic examination is one of the best modalities for the diagnosis of stenoses and other diseases of the carotid, vertebral, and subclavian arteries. If abnormal Doppler waveforms in the VA are found, duplex interrogation of both SAs should be performed (even if a SA scan is not a part of your routine protocol). Vascular technologists should visualize the most proximal segment of the SA prior to the origin of the VA. To ensure that the correct part of the SA is being scanned, first find the VA origin, and then sample the SA proximal to the VA’s origin with color and pulsed Doppler. If this approach is not successful or technically impossible, an alternative technique is to visualize the proximal innominate artery and the left SA via the suprasternal notch using an electronic sector transducer. Proficiency in the anatomy and pathophysiology of SSS paired with adequate scanning skills of a vascular technologist are paramount for the accurate detection of SSS.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.