
Abstract
This case study presents the sonographic features of recurrent dermatofibrosarcoma protuberans, an uncommon soft tissue neoplasm. The original primary tumor presented five years earlier and was surgically excised. The current presentation demonstrates sonographic evaluation of several superficial left lower quadrant masses suspicious for tumor recurrence. This was confirmed by core needle biopsy and was followed by wide surgical excision. No evidence of metastasis was found, and no chemo or radiotherapy was offered.
Dermatofibrosarcoma protuberans (DFSP) is a rare soft tissue neoplasm with intermediate- to low-grade malignant potential. Although metastasis rarely occurs, DFSP is a locally aggressive tumor with a high recurrence rate. It accounts for less than 0.1% of all malignant neoplasms and approximately 1% of all soft tissue sarcomas.1,2 The annual incidence of DFSP in the United States is reported as 4.2 cases per million population from nine population-based cancer registries from 1973 to 2002. 3 DFSP has been reported in persons of all races, and no racial predilection seems to exist in previous reports. The neoplasm usually occurs in adults aged 20 to 50 years. 4 Surgical excision is the mainstay of treatment. Chemotherapy is rarely used, and radiation therapy can be used as an adjunct to surgery when clear surgical margins are not confident.5,6
Case Study
A man in his mid-20s presented for sonographic evaluation of several nontender superficial subcutaneous masses in his left lower quadrant. The firm irregular nodules were several centimeters in diameter. The skin surface varied in color from flesh to reddish brown. There was a large surgical scar inferior to the nodules. The patient’s clinical history was significant for surgical removal of similar nodules in the same area five years earlier. The nodules appeared in the skin of the left lower quadrant and grew in size over the course of 36 months. Core needle biopsy of the nodules revealed a cellular pattern consistent with DFSP. The patient states that computed tomography (CT) imaging of the chest, abdomen, and pelvis revealed no evidence of metastasis. (The previous pathology and imaging reports could not be located.) The masses were removed using a wide surgical excision. No postoperative chemotherapy or radiation therapy treatments were performed.
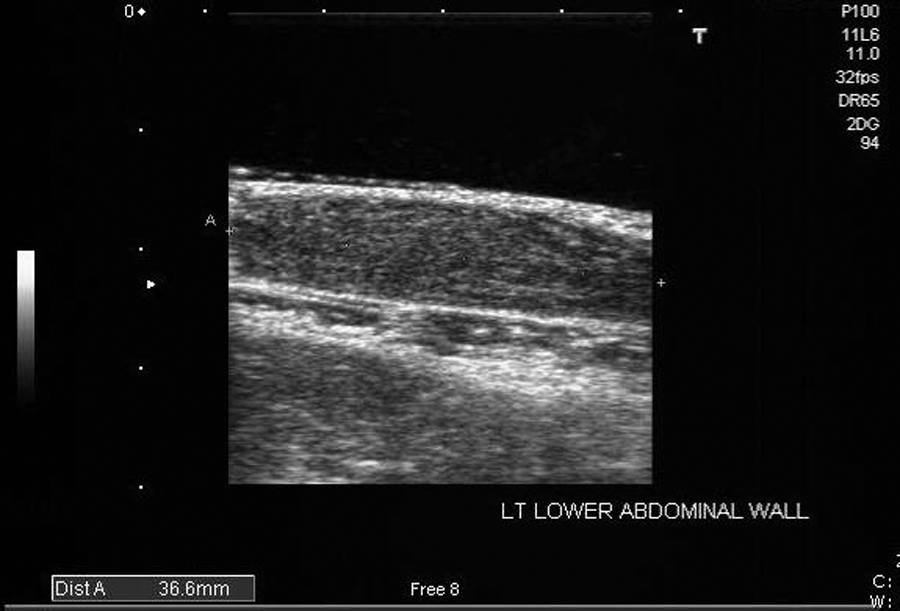
The current masses began appearing four years after the initial surgery. They continued to increase in size over the 12 months leading up to the current presentation. The sonographic evaluation was performed on a Toshiba Nemio sonographic system (Toshiba, Tustin, California) using a linear array 11-MHz transducer. A 3 × 9-cm soft tissue standoff pad (Parker Laboratories, Fairfield, New Jersey) was used for better near-field resolution. Three complex subcutaneous nodules were identified measuring 10 mm, 32 mm, and 37 mm, respectively (Figures 1–3). The nodules had well-defined margins and demonstrated moderate through transmission. Power color Doppler demonstrated moderate internal vascular flow in all of the lesions (Figure 4). Sonographic evaluation of the region, including the left inguina, found no additional masses, muscular/facial involvement, or enlarged lymph nodes. Core needle biopsy of the masses revealed interwoven bundles of spindle cells with plump nuclei arranged in a storiform pattern, and immunohistochemical staining was CD34 positive. The suspected diagnosis of recurrent dermatofibrosarcoma was confirmed. The masses were removed using a wide surgical excision. Postoperative CT and positron emission tomography (PET) body imaging revealed no evidence of metastasis. The patient was advised to have annual CT and PET body imaging for the next four to five years to rule out recurrence.

Long-axis image of the 32-mm lesion demonstrating a complex echo architecture.

Long-axis image of the 10-mm lesion, which appears heterogeneous and predominantly solid.
Long-axis image of the 37-mm lesion with a very homogeneous texture.
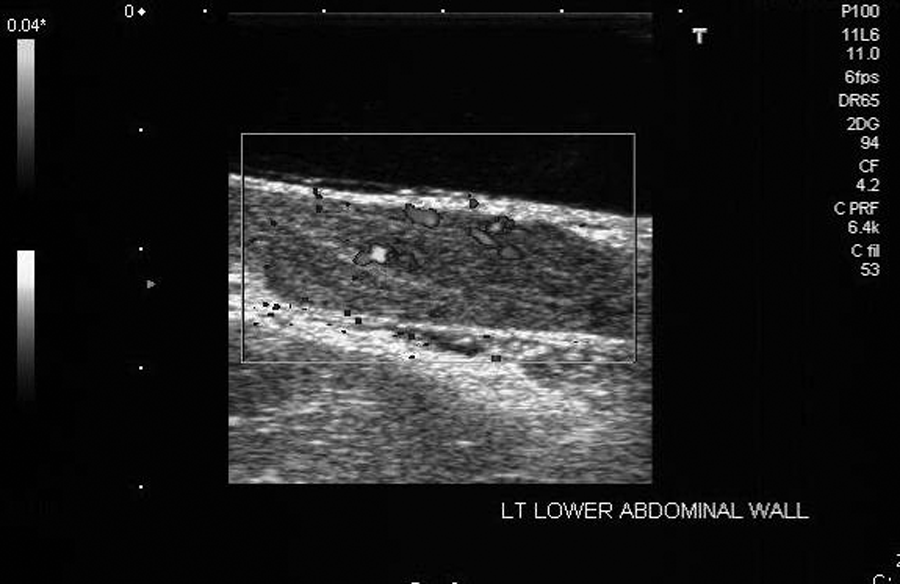
Power color Doppler showing vascular flow within the largest lesion.
Discussion
DFSP is an uncommon soft tissue neoplasm with an intermediate- to low-grade malignant potential. Although metastasis rarely occurs, DFSP is a locally aggressive tumor with a high recurrence rate. It is a cutaneous malignancy that arises from the dermis and invades deeper subcutaneous tissue (e.g., fat, fascia, muscle, bone). DFSP is a very slow-growing tumor. Because of the slow progression, the diagnosis is often delayed for months to years. It usually starts as a small asymptomatic papule that is likely ignored. The tumor gradually enlarges into a lumpy nodule.1,2
The cellular origin of DFSP is not clear. Evidence supports the cellular origin being fibroblastic, histiocytic, or neuroectodermal. It manifests partial features of each. Therefore, many authorities suggest pluripotential progenitor cells, such as undifferentiated mesenchymal cells, may be the origin of DFSP because they have the capacity to differentiate into all three cell types. 7 In 10% to 20% of patients with this tumor, trauma at the site seems to be incriminating. Surgical and old burn scars and sites of vaccinations have all been reported as sites of DFSP.8,9
DFSP accounts for less than 0.1% of all malignant neoplasms and approximately 1% of all soft tissue sarcomas. It is the most common type of cutaneous sarcoma. In a most recent study based on data from nine cancer registries from 1973 to 2002, the annual incidence of DFSP in the United States is reported at 4.2 cases per million population per year. The relative five-year survival rate for DFSP is 99.2%. 3 Although metastasis is rare (only 1%–4% reported), almost all metastatic cases have been associated with local recurrence. DFSP has been reported in persons of all races, and no racial predilection seems to exist in previous reports. The neoplasm usually occurs in adults aged 20 to 50 years. 4
The differential diagnosis of DFSP includes dermatofibroma, epidermal inclusion cyst, keloid and hypertrophic scar, malignant melanoma, metastatic carcinoma of the skin, and morphea, as well as fibroma and lymphoma. 7
Surgical excision remains the mainstay of treatment for DFSP. Because of its infiltrating growth pattern, it commonly extends far beyond the clinical margins; this accounts in part for the high recurrence rate after surgical excision. Hence, a wide excision of 2 to 3 cm or more of the margins beyond the clinically identifiable tumor border, down to and including the fascia, is recommended for the treatment of DFSP.9–11
Currently, chemotherapy is rarely used in the treatment of DFSP. Limited case reports have not shown any significant value of conventional chemotherapy in the treatment of this neoplasm. 5 Radiation therapy has had a limited role in the past, but recently, it has been used as an adjunct to surgery. Radiation therapy may be recommended for patients when clear surgical margins are not confident or for situations in which adequate wide excision alone may result in major cosmetic deficits. Postoperative adjuvant external beam radiotherapy doses range from 50 to 70 Gy. Overall, the risk of severe complications from radiotherapy is low. Close follow-up care is warranted because some DFSP tumors may become more aggressive. 6
Conclusion
Because of its ease and superior superficial resolution, sonography is an extremely useful diagnostic tool in the identification of cutaneous and subcutaneous masses. Furthermore, it can help in identifying local and regional lymph node involvement as well as muscular and fascial invasion associated with metastasis. It should be the imaging modality of choice for most cutaneous and subcutaneous masses.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.